This document discusses childhood asthma, including its prevalence, pathophysiology, risk factors, diagnosis, impact, and barriers to effective management. Some key points:
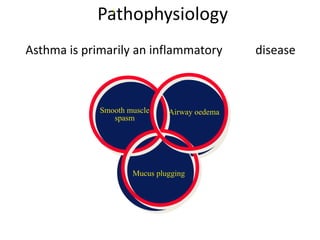
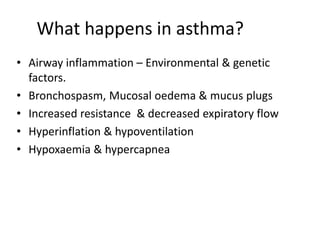
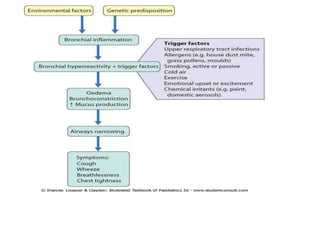
- Asthma is a common chronic respiratory disorder affecting 15-20% of children globally. It causes inflammation and narrowing of the airways.
- It has physical, social, and emotional impacts on children and families, including limitations on activities, school absenteeism, feelings of isolation, and increased stress.
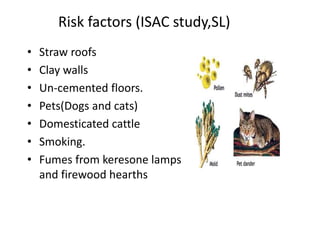
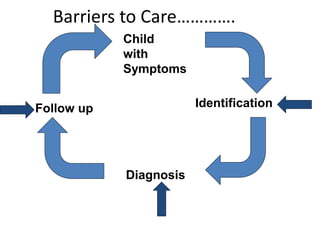
- Barriers to effective management include late or under diagnosis, lack of education, cultural beliefs, non-adherence to treatment, and limited healthcare resources.
- Improving primary care, education programs for families and healthcare providers,