Introduction
• According torecent statistics sudden cardiac arrest is rapidly becoming the
leading cause of death.
• Once the heart ceases to function, a healthy human brain may survive without
oxygen for up to 4 minutes without suffering any permanent damage.
Unfortunately, a typical EMS response may take 6, 8 or even 10 minutes.
• It is during those critical minutes that CPR (Cardio Pulmonary Resuscitation)
can provide oxygenated blood to the victim's brain and the heart, dramatically
increasing his chance of survival and if properly instructed, almost anyone can
learn and perform CPR.
3.
What is BLS?
• Basic Life Support (BLS) refers to the care healthcare providers and
public safety professionals provide to patients who are experiencing
respiratory arrest, cardiac arrest or airway obstruction.
• BLS includes psychomotor skills for performing high-quality
cardiopulmonary resuscitation (CPR), using an automated external
defibrillator (AED) and relieving an obstructed airway for patients of all
ages.
4.
Timeline of CPR
•0 to 4 minutes, unlikely development of brain damage
• 4 to 6 minutes, possibility of brain damage
• 6 to 10 minutes, high probability of brain damage
• 10 minutes and over, probable brain damage
Goals of Resuscitation
•To support and restore effective:-
- oxygenation
- ventilation
- circulation with return of intact neurologic function
• ROSC (Return of spontaneous circulation) is an
intermediate goal
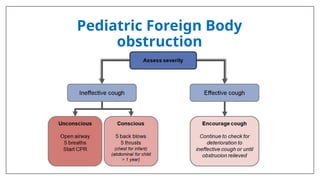
b.) For Pediatric
•Emergencies in children and infants are not usually
caused by the heart. Children and infants most often
have breathing problems that trigger cardiac arrest.
The first and most important step of the Pediatric Chain
of Survival is prevention
CAUTION
Use of cricoidPressure
• The routine use of cricoid pressure in cardiac patients is not recommended.
• Cricoid pressure in nonarrest patients may offer some measure of protection
to the airway from aspiration and gastric insufflation during bag and mask
ventilation. However, it also may impede ventilation and interfere with
placement of a supraglottic airway or intubation
12.
In 2020 Guideline
•The importance of early initiation of CPR by lay rescuers has been re-
emphasized. The risk of harm to the patient is low if the patient is not in
cardiac arrest. Bystanders should not be afraid to start CPR even if they are
not sure whether the victim is breathing or in Cardiac Arrest.
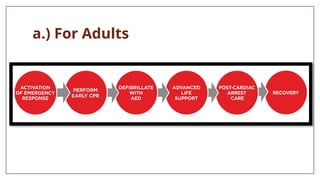
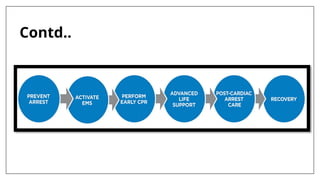
• A sixth link, Recovery, was added to the Chains of Survival for both
Pediatric and Adults.
• Care of the patient after return of spontaneous circulation (ROSC) requires
close attention to oxygenation, blood pressure control, evaluation for
percutaneous coronary intervention, targeted temperature management, and
multimodal neuroprognostication.
13.
How to approacha patient ?
Ans- A Systematic Approach is used
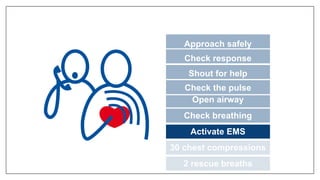
APPROACH SAFELY!
• Scene
•Rescuer
• Victim
• Bystanders
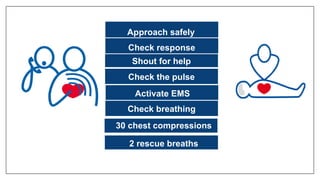
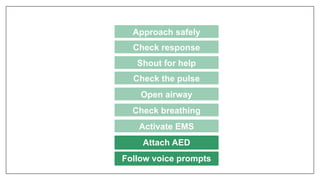
Approach safely
Check response
Check the pulse
Open airway
Check breathing
Activate EMS
30 chest compressions
2 rescue breaths
Shout for help
18.
CHECK RESPONSE
Approach safely
Checkresponse
Check the pulse
Open airway
Check breathing
Activate EMS
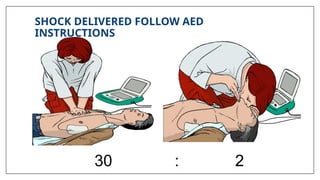
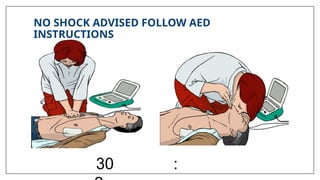
30 chest compressions
2 rescue breaths
Shout for help
19.
Shake shoulders gently
Ask“Are you all right?”
If he responds
• Leave as you find him.
• Find out what is wrong.
• Reassess regularly.
Contd..
20.
SHOUT FOR HELP
Approachsafely
Shout for help
Check the pulse
Open airway
Check breathing
Activate EMS
30 chest compressions
2 rescue breaths
Check for response
21.
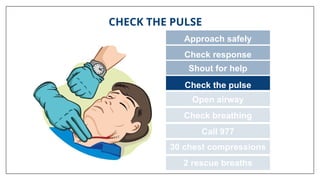
CHECK THE PULSE
Approachsafely
Check response
Check the pulse
Open airway
Check breathing
Call 977
30 chest compressions
2 rescue breaths
Shout for help
22.
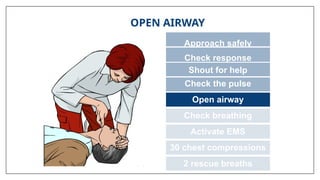
OPEN AIRWAY
Approach safely
Checkresponse
Check the pulse
Open airway
Check breathing
Activate EMS
30 chest compressions
2 rescue breaths
Shout for help
23.
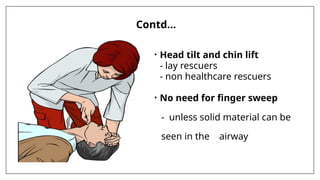
Contd…
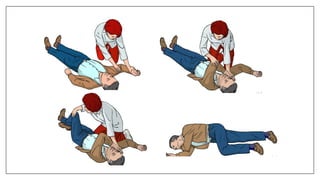
• Head tiltand chin lift
- lay rescuers
- non healthcare rescuers
• No need for finger sweep
- unless solid material can be
seen in the airway
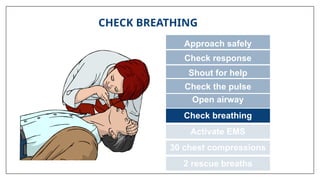
CHECK BREATHING
Approach safely
Checkresponse
Shout for help
Open airway
Check breathing
Activate EMS
30 chest compressions
2 rescue breaths
Check the pulse
26.
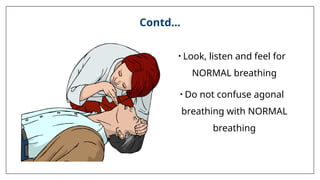
Contd…
• Look, listenand feel for
NORMAL breathing
• Do not confuse agonal
breathing with NORMAL
breathing
27.
CAUTION
• Agonal gaspsare not normal breathing. Agonal gaps may be present in
the minutes after sudden cardiac arrest.
• Occurs shortly after the heart stops
in up to 40% of cardiac arrests
• Described as barely, heavy, noisy or gasping breathing
Recognise as a sign of cardiac arrest
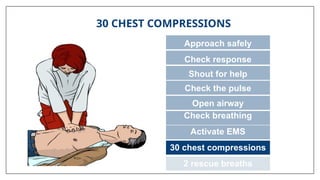
30 CHEST COMPRESSIONS
Approachsafely
Check response
Shout for help
Open airway
Check breathing
Activate EMS
30 chest compressions
2 rescue breaths
Check the pulse
31.
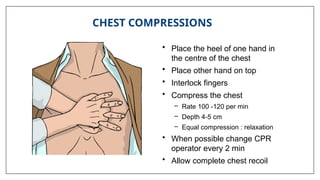
• Place theheel of one hand in
the centre of the chest
• Place other hand on top
• Interlock fingers
• Compress the chest
– Rate 100 -120 per min
– Depth 4-5 cm
– Equal compression : relaxation
• When possible change CPR
operator every 2 min
• Allow complete chest recoil
CHEST COMPRESSIONS
32.
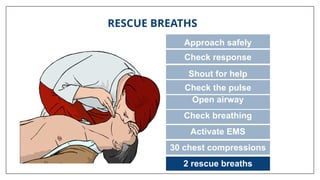
RESCUE BREATHS
Approach safely
Checkresponse
Shout for help
Open airway
Check breathing
Activate EMS
30 chest compressions
2 rescue breaths
Check the pulse
33.
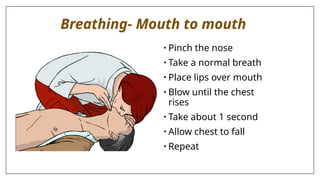
Breathing- Mouth tomouth
• Pinch the nose
• Take a normal breath
• Place lips over mouth
• Blow until the chest
rises
• Take about 1 second
• Allow chest to fall
• Repeat
34.
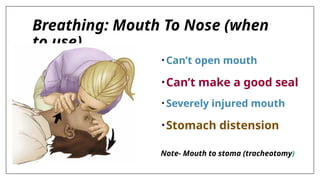
Breathing: Mouth ToNose (when
to use)
• Can’t open mouth
•Can’t make a good seal
• Severely injured mouth
•Stomach distension
Note- Mouth to stoma (tracheotomy)
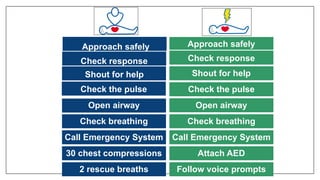
Approach safely
Check response
Shoutfor help
Open airway
Check breathing
Call Emergency System
30 chest compressions
2 rescue breaths
Check response
Approach safely
Shout for help
Check the pulse
Open airway
Check breathing
Call Emergency System
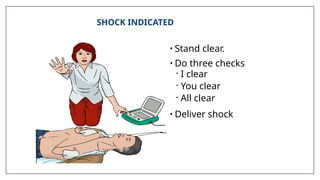
Attach AED
Follow voice prompts
Check the pulse
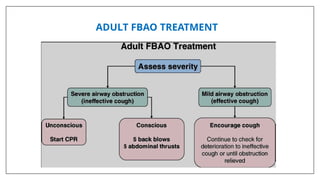
How to identifyobstruction ?
• Patent Airway - If the patient responds in a normal voice.
• Partial Obstruction- Signs of a partially obstructed airway include a changed
voice, noisy breathing (eg, stridor), and an increased breathing effort.
• Complete Airway obstruction- With a completely obstructed airway, there is no
respiration despite great effort (ie, paradox respiration, or “see-saw” sign).
49.
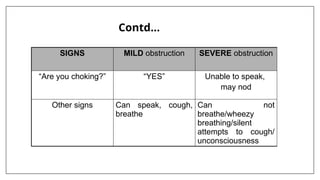
SIGNS MILD obstructionSEVERE obstruction
“Are you choking?” “YES” Unable to speak,
may nod
Other signs Can speak, cough,
breathe
Can not
breathe/wheezy
breathing/silent
attempts to cough/
unconsciousness
Contd…
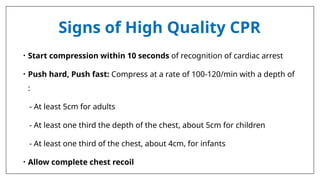
Signs of HighQuality CPR
• Start compression within 10 seconds of recognition of cardiac arrest
• Push hard, Push fast: Compress at a rate of 100-120/min with a depth of
:
- At least 5cm for adults
- At least one third the depth of the chest, about 5cm for children
- At least one third of the chest, about 4cm, for infants
• Allow complete chest recoil
58.
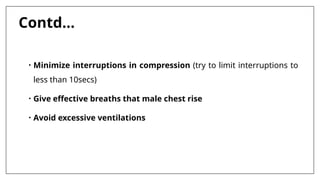
Contd…
• Minimize interruptionsin compression (try to limit interruptions to
less than 10secs)
• Give effective breaths that male chest rise
• Avoid excessive ventilations
59.
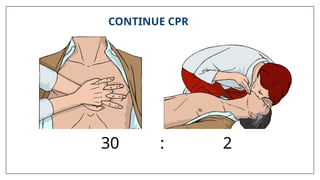
CONTINUE RESUSCITATION UNTIL
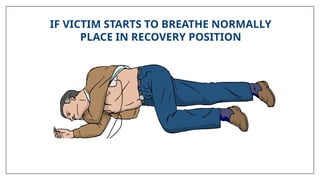
•Qualified help arrives and takes over
• The victim starts breathing normally
• Rescuer becomes exhausted
60.
When Can IStop CPR ?
• Victim revives
• Trained help arrives
• Too exhausted to continue
• Unsafe scene
• Physician directed (do not resuscitate orders)
• Cardiac arrest of longer than 30 minutes
61.
Injuries Related toCPR
• Rib fractures
• Laceration related to the tip of the sternum, Liver, lung,
spleen
62.
Complications of CPR
•Vomiting
• Aspiration
• Place victim on left side
• Wipe vomit from mouth with fingers wrapped in a cloth
• Reposition and resume CPR
AIRWAY
• Is theairway patent ?
• Is an advanced airway indicated?
• Is proper placement of airway device confirmed?
• Is tube secured and placement confirmed frequently?
68.
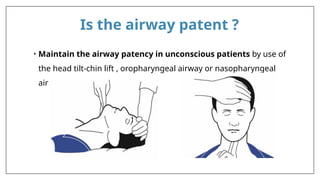
Is the airwaypatent ?
• Maintain the airway patency in unconscious patients by use of
the head tilt-chin lift , oropharyngeal airway or nasopharyngeal
airway
69.
Is an advancedairway indicated?
• Use advanced airway management if needed (eg- laryngeal
mask ,laryngeal tube , oesophageal –tracheal tube, endotracheal tube)
NOTE:- Health care providers must weighs the benefit of advanced
airway placement against adverse effects of interrupting chest
compressions. If bag-mask ventilation is adequate, health care
providers may defer insertion of advanced airway.
70.
Contd…
If using advancedairway devices:-
• Confirm proper integration of CPR and ventilation
• Confirm proper placement of advanced airway devices by
- Physical examination
- Quantitative waveform capnography
• Secure the device to prevent dislodgement
• Monitor airway placement with continuous quantitative waveform
capnography
71.
Continuous waveform capnography
•Quantitative waveform capnography is the continuous,
noninvasive measurement and graphical display of end-tidal
carbon dioxide/ETCO2 (also called PetCO2). Capnography uses a
sample chamber/sensor placed for optimum evaluation of expired
CO2.
• The inhaled and exhaled carbon dioxide is graphically displayed as a
waveform on the monitor along with its corresponding numerical
measurement.
72.
Contd..
Two very practicaluses of waveform capnography in CPR are:
1.) evaluating the effectiveness of chest compressions, and
2.) identification of ROSC. Evaluating the effectiveness of chest
compressions is accomplished in the following manner:
Measurement of a low ETCO2 value (< 10 mmHg) during CPR in an
intubated patient would indicate that the quality of chest compressions
needs improvement.
• Normal ETCO2 in the adult patient should be 35-45 mmHg.
• High quality chest compressions are achieved when the ETCO2 value is at least 10-
20 mmHg.
73.
Contd..
• When ROSCoccurs, There will be a significant increase in the
ETCO2. (35-45 mmHg) This increase represents a drastic
improvement in blood flow (more CO2 being dumped in the lungs
by the circulation) which indicates circulation.
74.
Contd..
• The 2020AHA Guidelines for ACLS recommend using quantitative
waveform capnography in intubated patients during CPR. Waveform
capnography allows providers to monitor CPR quality, optimize chest
compressions, and detect ROSC (return of spontaneous circulation)
during chest compressions.
• Also, according to the AHA, continuous waveform capnography along
with clinical assessment is the most reliable method of confirming
and monitoring correct placement of an ET tube.
75.
BREATHING
• Are ventilationand oxygenation adequate?
• Are quantitative waveform capnography and
oxyhemoglobin saturation monitored?
76.
Contd..
• Give supplementaryoxygen when indicated
- For cardiac arrest patients, administer 100% oxygen
- For others, titrate oxygen administration to achieve oxygen saturation of
94% or greater by pulse oximetry
• Monitor the adequacy of ventilation and oxygenation by
- Clinical criteria( chest rise and cyanosis)
- Quantitative waveform capnography
- oxygen saturation
• Avoid excessive ventilation
77.
CIRCULATION
• Are chestcompressions effective?
• What is the cardiac rhythm?
• Is defibrillation or cardioversion indicated?
• Has IV/IO access been established?
• Is ROSC present?
• Is the patient with a pulse unstable?
• Are medications needed for rhythm or blood pressure?
• Does the patient need volume (fluid) for resuscitation?
78.
Contd..
• Monitor CPRquality
- Quantitative waveform capnography (if PETCO₂ is less than 10 mm Hg, atte
to improve CPR quality)
- Intra-arterial pressure (if relaxation phase [diastolic] pressure is less than
20 mm Hg, attempt to improve CPR quality)
• Attach monitor/defibrillator for arrhythmias or cardiac arrest rhythms
(eg, tricular fibrillation [VF], pulseless ventricular tachycardia [PVT], asystole,
pulse electrical activity [PEA])
• Provide defibrillation/cardioversion
79.
Contd..
• Obtain IV/IOaccess
• Give appropriate drugs to manage rhythm and blood pressure
• Give IV/IO fluids if needed
• Check glucose and temperature
• Check perfusion issues
80.
DISABLITY
• Check forneurologic function
• Quickly assess for responsiveness, levels of consciousness, and
pupil dilation
• Assess for AVPU
A - Alert
V - Voice
P - Painful
U- Unresponsive
81.
EXPOSURE
• Remove clothingto perform a physical examination, looking for
obvious signs of trauma, bleeding, burns, unusual markings, or
medical alert bracelets
82.
SECONDARY ASSESSMENT
• Secondaryassessment involves the differential diagnosis, including
a focused medical history and searching for and treating underlying
causes (H;s and T;s)
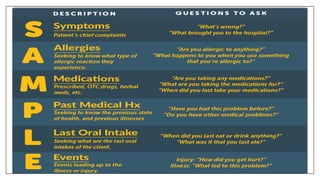
• Ask specific question related to the patient's presentation consider
using memory aid SAMPLE
#2 According to recent stats, more than 70% SCA or Sudden Cardiac Arrests occur at home or similar private settings.
95% of Sudden Cardiac Arrest victims die prior to even reaching the hospital. Out of all these numbers, only 6% survive cardiac arrest.
Effective CPR provided by a bystander in the first few minutes of cardiac arrest can increase the chances of survival by 2x or 3x.
If a bystander does not perform CPR, the survival chances of a victim will decrease 7% in every single minute of delay.



![Contd..
• Monitor CPR quality
- Quantitative waveform capnography (if PETCO₂ is less than 10 mm Hg, atte
to improve CPR quality)
- Intra-arterial pressure (if relaxation phase [diastolic] pressure is less than
20 mm Hg, attempt to improve CPR quality)
• Attach monitor/defibrillator for arrhythmias or cardiac arrest rhythms
(eg, tricular fibrillation [VF], pulseless ventricular tachycardia [PVT], asystole,
pulse electrical activity [PEA])
• Provide defibrillation/cardioversion](https://image.slidesharecdn.com/blsppt-251008164133-a1be3774/85/BLS-ppt-ppt-FOR-BASIC-LIFE-SUPPORT-BY-AHA-78-320.jpg)