This document reviews clinical trials that have investigated the therapeutic effects of Nigella sativa (black seed) and its main active constituent, thymoquinone. It finds that black seed and thymoquinone have been shown to have anti-inflammatory, antimicrobial, analgesic and anti-epileptic properties. Several studies found black seed to be safe and well-tolerated, with few or mild side effects reported. However, more clinical and animal studies are still needed to fully understand the effects and applications of black seed and thymoquinone.
![Review on Clinical Trials of Black Seed (Nigella sativa )
and Its Active Constituent, Thymoquinone
Alireza Tavakkoli1
, Vahid Mahdian2
, Bibi Marjan Razavi3
, Hossein Hosseinzadeh4
*
Abstract
Objectives: Nigella sativa (black seed or black cumin),
which belongs to the Ranunculacea family, is an annual
herb with many pharmacological properties. Among
its many active constituents, thymoquinone (TQ) is
the most abundant constituent of the volatile oil of Ni-
gella sativa (N. sativa) seeds, and it is the constituent to
which most properties of this herb are attributed.
Methods: PubMed-Medline, Scopus, and Web of Sci-
ence databases were searched to identify randomized
control trials (RCTs) investigating the therapeutic effects
of N. sativa and/or TQ. In this review, we investigated
the clinical uses of N. sativa and TQ in the prevention
and the treatment of different diseases and morbidity
conditions in humans.
Results: Black seed and TQ are shown to possess multi-
ple useful effects for the treatment of patients with sev-
eral diseases, such as inflammatory and auto-immune
disorders, as well as metabolic syndrome. Also, other
advantages, including antimicrobial, anti-nociceptive
and anti-epileptic properties, have been documented.
The side effects of this herbal medicine appear not to be
serious, so it can be applied in clinical trials because of
its many advantages.
Conclusion: Some effects of N. sativa, such as its
hypoglycemic, hypolipidemic and bronchodilatory
effects, have been sufficiently studied and are suffi-
ciently understood to allow for the next phase of clini-
cal trials or drug developments. However, most of its
other effects and applications require further clinical
and animal studies.
1. Introduction
Nigella sativa (black seed or black cumin), which be-
longs to the Ranunculacea family, is an annual herb
with many pharmacological properties [1]. The use of
N.sativa(NS)seedsandoilintraditionalremediesgoes
back more than 2000 years, and the herb is described
as ‘the Melanthion’ by Hippocrates and Discroides [2].
Black seeds and their oil have a long history of folklore
usage in the Indian and the Arabian civilizations as
food and medicine and have been commonly used as
treatment for a variety of health conditions pertaining
to the respiratory system, digestive tract, kidney and
liver functions, cardiovascular system, and immune
system support, as well as for general well-being [3, 4].
NS contains many active components, such as thymo-
quinone (TQ), alkaloids (nigellicines and nigelledine),
saponins (alpha-hederin), flavonoids, proteins, fatty
acids, and many others, that have positive effects in the
treatment of patients with different diseases [5, 6]. TQ
Review
article
Key Words
black seed, clinical trials, diseases, Nigella sativa, safety,
thymoquinone
ISSN 2093-6966 [Print], ISSN 2234-6856 [Online]
JournalofPharmacopuncture2017;20[3]:179-193
DOI: https://doi.org/10.3831/KPI.2017.20.021
This is an Open-Access article distributed under the terms of the Creative Commons
Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/)
which permits unrestricted noncommercial use, distribution, and reproduction in any
medium, provided the original work is properly cited.
This paper meets the requirements of KS X ISO 9706, ISO 9706-1994 and ANSI/NISO
Z39.48-1992 (Permanence of Paper).
*
Corresponding Author
Hossein Hosseinzadeh. Pharmaceutical Research Center, Department of Pharmacody-
namics and Toxicology, School of Pharmacy, Mashhad University of Medical Sciences,
Mashhad, Iran.
Tel: +98-51-1881-9042 Fax: +98-51-1882-3251
E-mail: hosseinzadehh@mums.ac.ir
ⓒ 2017 Korean Pharmacopuncture Institute http://www.journal.ac
Received: Apr 28, 2017 Reviewed: Aug 21, 2017 Accepted: Aug 30, 2017
1
Department of Pharmacognosy, School of Pharmacy, Mashhad University of Medical Sciences, Mashhad, Iran
2
Student Research Committee, School of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran
3
Targeted Drug Delivery Research Center, Department of Pharmacodynamics and Toxicology, School of Pharmacy, Mashhad University
of Medical Sciences, Mashhad, Iran
4
Pharmaceutical Research Center, Department of Pharmacodynamics and Toxicology, School of Pharmacy, Mashhad University of Medi
cal Sciences, Mashhad, Iran](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-1-320.jpg)
![http://www.journal.ac
180
is the most abundant constituent in the volatile oil of NS
seeds, and most of the herb’s properties are attributed to it.
Cell culture studies and animal models have indicated
several therapeutic potentials, such as anti-cancer [5, 7-9],
antimicrobial [10, 11], analgesic [12, 13], antipyretic [14],
contraceptive and anti-fertility, anti-oxytocic [3], anti-
tussive [15], anti-inflammatory [12, 16], and anti-oxidant
[17-19] potentials, for black seed and its active component
TQ. NS or TQ anticancer activity has been demonstrated
for blood, breast, colon, pancreatic, liver, lung, fibrosar-
coma, prostate, and cervix cancer cell lines and in animal
models of lung, kidney, skin, colon, and breast cancer [7].
Black seed’s antimicrobial effects include those on gram-
negative and gram-positive bacteria, viruses, parasites,
Schistosoma, and fungi pathogens [10]. NS was also found
to be able to relieve the symptoms of or cure patients with
several diseases, such as hypertension, dyslipidemia, met-
abolic syndrome, diabetes [5, 20, 21], asthma [3], convul-
sion [22-24], and natural and chemical toxicities [25, 26].
Additionally, a suggestion was made that NS and TQ uti-
lization could prevent many disorders [6], including neu-
robehavioral [27], kidney [28, 29], and liver [4] disorders.
For these reasons, in this review, we investigated the clini-
cal uses of NS and TQ in the prevention and treatment of
different diseases and morbidity conditions in humans.
Fig. 1.
Journal of Pharmacopuncture 2017;20(3):179-193
Figure 1 Schematic description for the effects of Nigella sativa in different parts of the human body.](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-2-320.jpg)
![http://www.journal.ac 181
Journal of Pharmacopuncture 2017;20(3):179-193
2. Methods
PubMed-Medline, Scopus, and Web of Science databases
were searched to identify randomized control trials (RCTs)
investigating the therapeutic effects of NS and/or TQ. We
reviewed the existing literature published until April 2016
by using the following keywords: Nigella sativa'', black
cumin'', black seeds'', thymoquinone'', and patient'',
clinic'' or clinical trial''. All studies assessing the effects
of NS or TQ, topical use or oral intake, on human health
conditions were included.
3. Results
3.1. Safety
Administration of NS oil (5 mL/day) to healthy volunteers
for 8 weeks was reported not to have any notable liver,
kidney, or gastrointestinal side effects [30, 31]. NS oil in-
take (equivalent to oil obtained from 0.7 g of seeds) for 40
days showed reasonable kidney and liver safety in patients
with type 2 diabetes mellitus (DM); neither did it alter the
platelet or the total leukocyte count [32]. Another study
performed on 39 centrally obese men demonstrated that
intake of NS seeds (3 g/day for 3 months) had no detect-
able side effects [33]. Qidwai et al reported that the admin-
istration of NS seeds (2 g/day for 6 weeks) did not affect the
serum alanine aminotransferase (ALT) or the serum creat-
inine (Cr) levels in adults [34]. Furthermore, NS at doses of
1, 2 and 3 g/day for 3 months did not adversely affect either
the renal or the hepatic functions of diabetic patients [35].
Another study revealed that NS seed powder intake for 40
days caused no significant change in total leukocyte and
platelet count [36].
Treatment with NS tea (5 g/day) added to the usual oral
anti-diabetic drugs, diet, and exercise for 6 months showed
significant decreases in aspartate aminotransferase (AST),
ALT, serum total, direct and indirect bilirubin, serum Cr,
and blood urea levels in type 2 diabetic patients, as well as
improved liver and kidney functions [37]. The intake of NS
extract (200 or 400 mg/day) for 2 months was also reported
to cause no observable complications in patients with mild
hypertension [38].
No adverse effects were reported in applications of NS
oil twice daily for six months to the lesions of vitiligo pa-
tients [39]. Intake of NS oil (0.05 mL/kg/day) in osteopenic
postmenopausal women for three months showed no
beneficial effects; however, no adverse side effects were
produced, either [40]. In another study conducted on Ira-
nian infertile men in order to assess the impacts of NS oil
(5 mL/day) on abnormal semen quality, no side effects
were observed [41]. Whereas no severe side effects were
reported in administration of NS oil (5 mL/day) to func-
tional dyspeptic patients, some mild adverse impacts were
observed, including nausea, bloating, and burning sensa-
tion [42]. On the other hand, some cases of epigastric pain
and hypoglycemia were reported as adverse effects when
NS oil capsules were used to treat patients with hepatitis
C virus (HCV) [43]. Dirjomuljono et al demonstrated the
safety of NS extract (1,080 mg/day) when used to treat pa-
tients with acute tonsillopharyngitis [44]. In another study
that investigated the anti-cestodal effects of NS powdered
seeds (40 mg/kg body weight) on children infected with
cestodes, no serious side effects were reported [45].
Treatment of seasonal allergic rhinitis patients with NS
seeds (250 mg/day) for two weeks has been reported not
to cause any adverse effects [46]. However, some patients
with allergic rhinitis when treated using nasal drops of
NS oil showed nasal dryness [47]. Dogar et al confirmed
that side effects produced by treatment of children with
acute lymphoblastic leukemia (ALL), aged between 2 - 18
years, with NS powder (40 mg/kg in two equal doses for 3
months), along with conventional therapy, were remark-
ably less than they were for L-asparaginase and conven-
tional therapy (note: conventional therapy includes dau-
norubicin, vincristine, and prednisolone). Thus, one can
conclude that NS powder, as an anti-cancer agent, is a
beneficial substitute for L-asparaginase in the treatment of
patients with ALL [48].
Nevertheless, in a patient suffering from DM, along with
coronary artery disease and hypertension, acute renal fail-
ure due to the use of NS tablets (2,000 – 2,500 mg/day) was
reported to have occurred 6 days after the start of treat-
ment [49]. Bamosa suggested that this adverse effect could
not have been related to NS because other clinical trials
with many more human subjects had demonstrated the
safety of NS in higher doses over longer periods of intake
and that the adverse effect could probably be attributed
to contamination of the tablets with other products [50].
Ibraheim also reported that only the total oil showed sig-
nificant increases in the AST and the ALT levels while both
the oil and the crushed seeds showed significant increases
in the γ-GT and the alkaline phosphatase (ALP) activities
[51]. A case of systemic and contact bullous drug eruption
as erythematous plaques with vesicles and bullous lesions
because of topical application and digestion of NS oil was
reported [52]. In addition, another report showed that the
use of NS at 5 g/day inhibited CYP2D6- and CYP3A4-me-
diated metabolism of dextromethorphan in healthy hu-
man volunteers, showing that it may interact with other
CYP2D6 and CYP3A4 substrates [53].
Taken together, NS has been established as a safe herbal
product. Nevertheless, according to the mentioned stud-
ies, some adverse effects, including nausea, bloating, and
burning sensation, have been reported after administra-
tion of NS oil in functional dyspeptic patients, and a slight
increase in liver and kidney enzymatic markers has been
shownfollowingconsumptionofNSoilandcrushedseeds.
3.2. Metabolic syndrome
Metabolic syndrome is a cluster of cardio-metabolic
conditions that include obesity, insulin resistance, ather-
ogenic dyslipidemia, and high blood pressure (BP) [54]
and is a major contributor to the development of diabetes
[55]. A RCT done on 60 patients with metabolic syndrome
showed that NS oil (5 mL/day) used in combination with
atorvastatin and metformin could decrease fasting blood
sugar (FBS), LDL, and TC significantly after six weeks](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-3-320.jpg)
![http://www.journal.ac
182
of use, but had no significant effect on body mass index
(BMI) or waist circumference (WC) [56].
Another study by Amin et al evaluated the effect of black
seeds (1.5 g/day) alone and concurrent with turmeric
(900 mg and 1.5 g/day, respectively) on 250 patients with
metabolic syndrome. The results show that NS and tur-
meric alone improved BMI, WC and BF% after 4 weeks,
compared to baseline. Combination therapy improved
all parameters including BMI, BF%, WC, hip circumfer-
ence (HC), BP, total cholesterol (TC), triglyceride (TG),
and C-reactive protein (CRP) except HDL-cholesterol with
lower FBG and LDL-cholesterol as compared to placebo
after four weeks. After 8 weeks, NS reduced lipids and FBG,
whereas turmeric decreased LDL-cholesterol and CRP.
Combination therapy showed an improvement in all pa-
rameters and reduced BF%, FBG, cholesterol, TG, LDL-
cholesterol, CRP and increased HDL-cholesterol [57].
In another study, premenopausal women underwent the
following protocol: 12-week administration of NS-powder
capsules (1,600 mg/day), a 2-week washout period, and
12-week administration of a placebo, and vise versa. The
authors of the study concluded that NS could help to con-
trol weight gain, the lipid profile, and the blood glucose
and hormonal levels [58]. According to a clinical trial by
Najmi et al, NS (500 mg/day) after 8 weeks was able to im-
prove the efficacy of the therapeutic protocol (metformin
+ atorvastatin + aspirin) in patients with metabolic syn-
drome and poor glycemic control so that NS-treated pa-
tients indicated significant improvements in their FBG,
postprandial blood glucose (PPBG), haemoglobin A1c
(HbA1c), and LDL-C levels [59].
The effects of NS and TQ on different components of met-
abolic syndrome and cardiovascular disease risk factors,
including high BP, obesity, dyslipidemia, and high blood
glucose, have been established [21]. The clinical uses of NS
and TQ in the prevention and treatment of these factors
will be discussed in subsequent subsections.
3.3. Hypertension
Hypertension (HT) is a lifestyle-related disease, and di-
etary modifications are effective for its management and
prevention. In a study performed by Dehkordi and Kam-
khah, which evaluated the anti-hypertensive effect of NS,
the intake of NS extract (200 or 400 mg/day) for 2 months
was reported to decrease both the systolic and the diastolic
BP in patients with mild HT as compared with the baseline
and the placebo values [38]. Another study by Huseini et al
on healthy volunteers who received NS oil (5 mL/day) for
two months revealed the hypotensive effect of NS, with the
systolic and the diastolic BP being lowered significantly as
compared with both the placebo and the baseline values
[31].
3.4. Obesity
Obesity, defined as excess fat mass, increases the risks for
multiple metabolic diseases, such as type 2 diabetes, car-
diovascular disease, and several types of cancer [60]. Some
RCTs demonstrated that NS oil in combination with a low-
calorie diet decreased weight in obese women in compari-
son to the placebo level [61, 62]. It also caused the super-
oxide dismutase (SOD) level to be elevated [61] and the TG
and the LDL-C levels to be decreased [62].
Another study was performed on 39 centrally obese men
to evaluate the effect of NS on body weight, WC, and some
biochemical parameters [33]. The results of that study
showed that intake of NS seeds (3 g/day for 3 months)
caused a very significant reduction in body weight and
WC, but insignificant reductions in the serum free testo-
sterone level, as well as the systolic and the diastolic BP,
and an insignificant increase in the adiponectin level. The
reduction of serum free testosterone in the control group,
who received two capsules of 750 mg flour twice daily, was
more than it was in the treatment group, thus indicating
that NS can inhibit the decrease in the serum free testo-
sterone level.
3.5. Dyslipidemia
Dyslipidemia is defined as the derangements of one or
more of the lipoproteins in blood, such as elevated TC,
LDL-C, and/or TG, or low levels of HDL-C alone [63].
Moeen-ud-din et al reported that the intake of 2 teaspoons
of NS seeds for 6 weeks by hyperlipidemic patients de-
creased their LDL-C (P-value 0.001) and increased their
HDL-C (P-value 0.01) as significantly as niacin [64]. The
results of another RCT indicated that compared to mineral
oil, administration of NS oil (5 mL/day) to healthy volun-
teers for 8 weeks induced significant decreases in the fast-
ing blood cholesterol, LDL, TG, glucose, and HbA1C levels
[30]. Administration of NS seeds (two spoons/day) to male
and female hyperlipidemic patients for 4 weeks signifi-
cantly (P-value 0.001) increased HDL-C and decreased
body weight [65].
Menopausal women are one of the high risk groups for
developing dyslipidemia. In a study by Ibrahim et al, the
administration of powdered NS seeds (1 g/day) over a two-
month intervention was found to decrease significantly
the TG, LDL-C and TC levels, but to increase the HDL-C
level [66]. However, one month after cessation of treat-
ment, the lipid profiles in the NS-treated group tended to
change towards the pretreatment levels. Another clinical
trial done for a similar duration showed that a supplement
of powdered NS seeds (1 g/day) could improve some bio-
chemical parameters, including the lipid profile and blood
glucose, in menopausal women, but had no significant ef-
fect on their body weight [67].
According to a World Health Organization (WHO) report,
coronary heart disease is a major cause of mortality in the
world [68]. The results of a study which examined the ef-
fects of NS on the lipid profiles in patients with stable coro-
nary artery disease indicated that intake of NS powder (500
mg/day) for 6 months concurrent with statin (10 - 20 mg/
day) both decreased the serum levels of TG, VLDL, LDL,
and TC and elevated the HDL level significantly whereas
statin alone decreased neither the TG, VLDL, LDL nor TC
level [69].
Journal of Pharmacopuncture 2017;20(3):179-193](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-4-320.jpg)
![http://www.journal.ac 183
In healthy female volunteers, administration of both
crushed seeds and the formulated total oil of NS caused
significant reductions in the prolactin, glucose, triglycer-
ide, and cholesterol levels. Additionally, administration
of the crushed seeds caused a significant increase in the
white blood cell count (WBC) and the hemoglobin level
whereas administration of NS oil only increased the hemo-
globin level significantly [51]. In another study, Bamosa et
al suggested that the administration of NS at 2 g/day for 2
weeks decreased the blood levels of both glucose and cho-
lesterol in healthy volunteers [70].
A large RCT compared the effects of simvastatin (10 mg/
Journal of Pharmacopuncture 2017;20(3):179-193
Study design Population
Part of the herb, dose,
and duration of treat-
ment
Result References
Randomized,
double-blind,
placebo-controlled
trial
72 Type 2 DM patients
(men and women aged
30 - 60 years old)
NS oil (3 g/day)
12 weeks
↓ BMI, insulin level and insulin
resistance as well as HDL-C as
compared with baseline ,
↓ FBS, TG, LDL-C and HbA1c as
compared to the placebo group
[77]
-
41 Type 2 DM patients
(men and women aged
30 - 60 years old)
NS oil (equivalent to
oil obtained from 0.7 g
of seeds)
40 days
↓ FBS ,↑ insulin, but reversed
after 40 days of placebo adminis-
tration
[36]
Prospective study
60 patients with insulin
resistance (men and
women)
NS oil (5 mL/day) +
atorvastatin (10 mg/
day) and metformin
(1 g/day)
6 weeks
↓ TC, LDL-C and FBS [78]
Randomized,
double blind,
placebo-controlled
clinical trial
43 Type 2 DM patients
(men and women)
NS oil extract
(1 g/day)
8 weeks
↓ TG, LDL-C, TC, and LDL-C to
HDL-C ratios as compared to the
placebo
[79]
-
41 type 2 DM patients
(men and women)
NS tea (5 g/day) +
usual oral anti-dia-
betic drugs, diet, and
exercises
6 months
↓ FBG, PPBG and HbA1c [37]
-
94 type 2 DM patients
(men and women)
NS seeds 2 g/day or 3
g/day
12 weeks
↓ FBG, 2hPG, and HbA1c,
↓ Insulin resistance ,
↑ β-cell function; no significant
change in body weight
[35]
NS seeds 1 g/day,
12 weeks
Insignificant changes [35]
-
41 type 2 DM patients
(men and women aged
30 - 60 years old)
NS seed powder,
40 days
↓ FBG, TC, LDL-C and TG,
↑ HDL-C and insulin; all men-
tioned values except HDL signifi-
cantly reversed again after 40 days
of placebo intake
[36]
Table 1 Effects of Nigella sativa supplementation on patients with diabetes
DM, Diabetes mellitus; NS, Nigella sativa; BMI, Body mass index; HDL-C, High density lipoprotein-cholesterol; TG, Triglyceride; LDL-
C, Low density lipoprotein-cholesterol; HbA1c, Haemoglobin A1c; FBS, Fasting blood sugar; TC, Total cholesterol; FBG, Fasting blood
glucose; PPBG, Postprandial blood glucose; 2hPG, 2 hours postprandial glucose.](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-5-320.jpg)
![http://www.journal.ac
184
day)aloneandconcurrentwithNSseeds(500mg/day)and
garlic oil (0.625 mg/day) on the lipid profile in 258 patients
with hyperlipidemia over an 8-week treatment [71]. In that
study, a comparison of mean values between the two treat-
ment groups indicated a highly significant difference (P =
0.01) for cholesterol, TG, non-HDL, and LDL reductions
and a significant difference (P = 0.03) for HDL elevation
[71]. Sabzghabaee et al reported that the TC, LDL, and TG
serum levels in hypercholesterolemic patients who took
NS at 2 g/day for 4 weeks decreased significantly [72]. The
uses of NS extract at 200 and 400 mg/day for 2 months were
also reported to have decreased both the total and the LDL
cholesterol in patients with mild HT as compared with the
baseline [38].
Of course, some controversies exist in the clinical trial
results. Qidwai et al reported that NS seeds (2 g/day) ad-
ministration had not affected the BMI, waist-hip ratio, BP,
FBS or serum lipids in adults after 6 weeks of use [34]. Un-
like pervasive evidence for the effects of NS use on the lipid
profile, the administration of powdered NS seeds was re-
ported to have had no significant effect on BP, serum lipid
levels,bloodsugar,orbodyweightinadults[73].According
to some meta-analyses, overall, the use of NS was shown
to reduce the plasma levels of TC, LDL-C and TG, but its
effect on HDL-C was not significant [74, 75]. Whereas the
use of NS seed oil was observed to have greater effects on
the serum TC and the LDL-C levels, versus the use of seed
powder, elevation of the HDL-C levels was found only after
supplementation with NS seed powder [75].
3.6. Diabetes
DM is characterized by chronic elevation of blood glu-
cose, which is a central factor in the production of reactive
oxygen species (ROS) that, in turn, promote cellular dam-
age and contribute to the development and progression
of diabetic complications [76]. In a report by Heshmati et
al, although the administration of NS oil at 3 g/day for 12
weeks was stated to have caused insignificant decreases in
the BMI, insulin level, and insulin resistance, as well as an
increase in the HDL-C level, in patients with type 2 diabe-
tes, the FBS, TG, LDL-C, and HbA1c levels were observed
to have been lowered significantly in the intervention
group as compared to the placebo group [77].
Another clinical trial showed that NS oil intake (equiva-
Journal of Pharmacopuncture 2017;20(3):179-193
Table 2 Clinical effects of Nigella sativa supplementation on the nervous system
NS, Nigella sativa.
Study design Population
Part of the herb, dose,
and duration of treat-
ment
Result References
Double-blinded
crossover clinical trial
23 epileptic children
Water extract of black
seed (40 mg/kg/8 h),
10 weeks
Significant reduction of
mean frequency of seizures
[80]
Pilot, double-blinded
crossover clinical trial
22 epileptic children
Thymoquinone
(1 mg/kg), 10 weeks
Significant reduction of
frequency of seizures
[81]
Prospective,
randomized,
single-blinded,
controlled,
crossover pilot study
30 intractable
epileptic patients
40 - 80 mg/kg/day of
black seed oil,
10 weeks
No beneficial effects in the
frequency and
severity of seizures
[82]
Placebo-controlled
clinical trial
40 healthy
elderly volunteers
500 mg NS seed cap-
sule twice a day,
9 weeks
Improvement of cognition,
memory, and attention
[83]
Placebo-controlled
clinical trial
48 healthy
adolescent males
500 mg NS capsule
once daily, 4 weeks
Enhancements of mood,
anxiety, and cognition
[84]
- 35 male opiate addicts
500 mg NS daily,
12 weeks
Significant reduction of
withdrawal effects
[85]
Randomized, triple-
blind, active, and
placebo-controlled
clinical trial
52 women with cyclic
mastalgia
Topical 600 mg
NS oil twice a day,
2 months
Significant improvement of
the pain scores
[86]](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-6-320.jpg)
![http://www.journal.ac 185
lent to oil obtained from 0.7 g of seeds) for 40 days caused a
significant reduction of FBS and a significant rise of insulin
in type 2 DM patients [32]. In still another study, the ad-
dition of NS oil at 5 mL/day to atorvastatin at 10 mg/day
and metformin at 1 g/day was shown to have induced sig-
nificant reductions in the TC, LDL-C, and FBS levels after
6 weeks of use in patients with insulin resistance [78]. Fur-
thermore, according to a study performed by Hadi et al on
43 type 2 diabetic patients, after an 8-week treatment, the
administration of NS oil extract at 1 g/day decreased the
serum levels of TG, LDL-C, and TC, as well as the LDL-C
to HDL-C ratio, significantly in comparison to the placebo
[79]. Moreover, treatment with NS tea at 5 g/day added to
the usual oral anti-diabetic drugs, diet, and exercise for 6
months led to significant decreases in the FBG, PPBG, and
HbA1c level in type 2 diabetic patients [37]. Another clini-
cal trial showed that the administration of NS at a dose of
2 g/day over a 12-week treatment caused significant de-
creases in the FBG, 2hPG, and HbA1c levels without any
significant change in body weight [35]. In that study, in-
sulin resistance, calculated by using a homeostatic model
assessment, was also reduced while β-cell function was
increased significantly. However, a dose of 1 g/day caused
insignificant changes, and no further increments in the
beneficial responses were observed with a dose of 3 g/day,
indicating that 2 g/day was the optimum dose. Bilal et al
reported the highly significant decreases in the FBG, TC,
LDL-C and TG levels and increases in the HDL-C and the
insulin levels were observed in patients with type 2 diabe-
tes after 40 days of NS seed powder intake [36]. However,
in that study, all mentioned values, except the HDL level,
significantly reversed again after 40 days of placebo intake.
Table 1.
3.7. Nervous system
Akhondian et al demonstrated that treatment of intracta-
ble pediatric seizures with water extract of black seed (40
mg/kg/8 h) versus placebo, as an adjuvant therapy to anti-
epileptic drugs, led to a significant reduction in the mean
frequency of seizures [80]. A similar clinical trial done by
the same author had similar outcomes, although TQ (1
mg/kg) was administered as an add-on therapy instead of
water extract of black seed [81]. On the other hand, anoth-
er study conducted by Shawki et al had a different result;
after administration of 40 - 80 mg/kg/day of black seed oil
as an adjuvant therapy for 4 weeks, no beneficial effects on
the frequency and severity of seizures in intractable epi-
leptic children were observed [82].
In a placebo-controlled clinical trial addressing memory
and cognition, healthy elderly volunteers took a 500-mg
NS capsule twice a day over a period of 9 weeks [83]. At the
end of that period, through special tests, the authors ob-
served improved cognition, memory, and attention. Simi-
larly, another CT performed on healthy adolescent males
aged 14 to 17 years established the modulatory effects on
cognition, mood, and anxiety of NS taken in the form of a
500-mg NS capsule once a day for four weeks [84].
Sangi et al introduced NS administration as a effective
non-opiate treatment for opioid dependence [85]. They
found that NS treatment offers some advantages in con-
trast with opiate treatments, such as relieving the with-
drawal effects, maintaining the physiological parameters,
and improving appetite. Table 2.
3.8. Analgesic effects
Huseini et al showed that as compared with the topi-
cal administration of diclofenac, topical administration
of NS oil had significant therapeutic effects on patients
with cyclic mastalgia without any adverse effects [86]. In
that study, 600 mg of NS oil (in the first treatment group)
and 20 mg of topical diclofenac (in the second treatment
group) were applied to the painful area twice daily for two
months.
3.9. Dermatology
Vitiligo is an autoimmune skin disease occurring due to
the destruction of skin melanocytes that produce skin pig-
ment. A RCT comparing the efficacy of applying NS oil and
fish oil to the lesions of vitiligo twice a day for six months
indicated that the former is more effective than the latter in
reducing the size of the lesions [39].
Hand eczema is a pruritic papulovesicular dermatitis se-
verely influencing the patient's quality of life. Yousefi et al
compared the effects of NS ointment, betamethasone, and
eucerin on the severity of hand eczema and the patients'
quality of life [87]. In that study, for new cases of hand ec-
zema in patients between 18 and 60 years of age the men-
tioned drugs were applied twice daily for 4 weeks. Through
particular measures, the authors concluded that NS may
be as effective as betamethasone in enhancing quality of
life and alleviating the severity of eczema and that both
were more effective than eucerin.
In contrast, for a comparison of the therapeutic effects of
NS oil ointment and aplacebo on patients with atopic der-
matitis (eczema), 20 patients were asked to apply NS oil on
one arm and a placebo on the other every day for 4 weeks
[88]. The authors of that study reported that no meaning-
ful difference could be found in terms of the parameters
measured, e.g., severity, pruritis, transepidermal water
loss, and skin hydration, between the treatment with NS
oil ointment and with a placebo.
Arsenical keratosis manifests itself in both the palms of
the hands and the soles of the feet due to chronic arsenic
consumption caused by drinking contaminated water.
Taking capsules of NS oil (500 mg) and vitamin E (200 mg)
for eight weeks has been shown to reduce the body’s ar-
senic load, thereby contributing to an overall alleviation of
the symptoms in patients with this disease [89].
3.10. Infectious diseases
Infection with HCV often leads to chronic hepatitis,
which, in turn, results in liver cirrhosis and hepatocellular
carcinomas. A study conducted in Egypt on HCV patients
Journal of Pharmacopuncture 2017;20(3):179-193](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-7-320.jpg)
![http://www.journal.ac
186
demonstrated that ethanolic extracts of NS and Zingiber
officinale (Z. officinale), alone and together, had benefi-
cial effects on HCV patients; i.e., their liver function was
improved and the viral load was decreased [90]. In that
study, a mixture of these extracts was observed to be more
effective than each one alone. Patients included in that
study were treated with capsules containing 500 mg of NS
and/or Z. officinale twice daily for one month. In a similar
study, HCV patients received capsules of NS oil (450 mg)
three times a day over a 3-month period. That treatment
led to the same results reported in Ref. 90, i.e., decreased
viral load and improved liver function [43].
Onifade et al confirmed that treatment of a sero-positive
human immunodeficiency virus (HIV) infected man with
NS concoction (10 mL twice/day for six months) resulted
in the reduction of the viral load to an undetectable level
in 3 months, an elevation of the CD4 count, an allevia-
tion of the symptoms, and a sustained sero-reversion [91].
Similarly, another study conducted by the same author on
a sero-positive HIV infected woman revealed the efficacy
of NS and honey therapy (10 mL thrice/day for 1 year)
for sustained sero-reversion [92]. These effects can be as-
cribed to the probable virucidal activity of NS [91].
The helicobacter pylori (H. pylori) bacterium can cause
many diseases, such as peptic ulcers and gastric cancer.
Infection with H. pylori has a high prevalence worldwide.
Salem et al stated that in a four-week course, the efficacy
of NS powder (2 g/day) administered together with ome-
prazole to eradicate an H. pylori infection in non-ulcer
dyspeptic patients was relatively the same as that of triple
therapy, although 1 g/day or 3 g/day of NS powder given
together with omeprazole was not as effective, indicating
that the optimal dose of NS was 2 g/day [93]. (Triple thera-
py includes clarithromycin, amoxicillin, and omeprazole.)
In a study conducted on children who were infected with
cestodes, the efficacy of single oral administration of NS
powdered seeds and ethanolic extract (40 mg/kg body
weight) was proven to reduce the percentage of fecal eggs
per gram, which means NS has an anti-cestodal effect
[45]. Furthermore, in a RCT in which 100 infected women
were included, the therapeutic effects of black seed cap-
sules (500 mg twice daily) used together with clotrimazole
vaginal cream on C. albicans vaginitis were compared
with those of placebo capsules (500 mg twice daily) used
in combination with the same vaginal cream [94]. In that
study, after a 7-day treatment, the black seed capsules
used with clotrimazole vaginal cream were more impres-
sive in reducing the symptoms of the disease, such as vagi-
nal itching, discharge, irritation, vulvovaginal redness and
inflammation [94].
3.11. Reproductive system
Kolahdooz et al proved that treatment of infertile Iranian
men with 2.5 mL of NS oil twice a day for two months, in
contrast with a placebo treatment in the same manner,
could enhance sperm parameters, including sperm count,
motility and morphology, semen volume, pH, and its
round cells [41]. Other beneficial effects of NS on Leydig
cells, reproductive organs, and sexual hormones in infer-
tile men have also been confirmed [95].
3.12. Respiratory system
As for lower respiratory tract illnesses (LRTI), Boskabady
et al investigated the antiasthmatic effects of NS boiled
extract (50 and 100 mg/kg), theophylline (5 mg/kg), and
salbutamol (200 μg) [96]. In that study, 15 asthmatic pa-
tients were recruited, and each patient received one of
these 4 treatments in random order at intervals of 48 hours
for 2 weeks. The results of that study demonstrated that
in spite of the fact that both doses of NS boiled extract
showed bronchodilatory effects, their efficacies for pul-
monary function test (PFT) elevation were less than those
of theophylline and salbutamol. The results also revealed
the prophylactic effects of NS boiled extract on adult asth-
matic patients. In another study, over a 3-month period,
the daily intake of 15 mL/kg of 0.1% NS boiled extract led
to more impressive improvements in the PFT parameters
and alleviations of the symptoms of asthma than the intake
of the placebo solution did [97]. Ahmad et al conducted a
study on 5- to15-year-old LRTI patients with wheezing and
investigated the beneficial impacts of the standard treat-
ment alone and the standard treatment combined with the
use of NS oil [98]. The authors of that study concluded that
the standard treatment when administered with NS oil (0.1
mg/kg for 14 days) had more beneficial effects in reducing
the pulmonary index and improving the peak expiratory
flow rate [98]. In another study, daily administration of
0.375 mL/kg of 50% NS boiled water extract, as compared
with a placebo solution to victims of chemical warfare, as
compared with a placebo solution, for two months effect-
ed meaningful improvements in the PFT measures and the
respiratory symptoms, indicating that the use of NS had a
prophylactic impact on victims of chemical warfare [99].
Allergic rhinitis (AR) is an inflammatory response of the
nasal mucosa to natural allergens and is characterized by
sneezing, rhinorrhea, nasal congestion, and itching [47,
100]. Moreover, a study comparing the therapeutic effects
of NS seeds (250 mg/day) and montelukast (10 mg/day) on
patients with seasonal allergic rhinitis over a course of two
weeks illustrated that both improved the daytime and oph-
thalmic symptoms considerably, although NS was more
efficient in alleviating the nighttime symptoms [46]. Simi-
larly, Nikakhlagh et al showed the positive effects of NS oil
capsule consumption over four weeks on the symptoms of
allergic rhinitis, i.e., nasal mucosal congestion, nasal itch-
ing, runny nose, sneezing attacks, turbinate hypertrophy,
and mucosal pallor [100]. Like the previous studies, that
of Alsamarai et al demonstrated that nasal drops of NS oil,
in comparison with nasal drops of ordinary food oil, could
significantly improve the symptoms of AR patients, as well
as their ability to tolerate exposure to allergens [47]. In that
study, each drop comprised 15 mL of oil, and the patients
applied 2 drops nasally (one in each nostril) 3 times dai-
ly for 6 weeks. In an additional study of AR patients who
underwent a month of allergen-specific immunotherapy
and then received treatment with NS seeds (2 g/d) dur-
ing the next month, in contrast with the AR patients who
only received immunotherapy for two months, the former
Journal of Pharmacopuncture 2017;20(3):179-193](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-8-320.jpg)
![http://www.journal.ac 187
showed more progress in their immune status, e.g., PMN
functions and CD8 counts [101]. That study showed that
NS administration contributed to a more effective immu-
notherapy. According to a study by Oysu et al, some of the
nasal symptoms of geriatric patients, for example, nasal
dryness, obstruction, and crusting, can be significantly
improved by using NS oil [102].
As for patients with tonsillopharyngitis, the results of a
study by Dirjomuljono et al indicated that NSPN capsules
containing 360 mg of NS and 50 mg of Phyllanthus niruri
extracts, as compared with a placebo, if given three times
a day for 7 days to patients with acute tonsillopharyngitis,
could significantly alleviate the symptoms of the disease
due to their anti-inflammatory and immuno-modulatory
effects [44]. In another study, which was undertaken on
patients with inhalation allergy, the beneficial impacts of
NS oil on the immune status of those patients, including
enhancement of the NK cell count and percentage of lym-
phocytes, were confirmed [103].
3.13. Skeletal system
Rheumatoid arthritis (RA) is a chronic systemic disease
characterized by inflammation of the joints, degeneration
of collagen fibers in mesenchymal tissues, and atrophy of
bones. Although the etiology is not well understood, au-
toimmunity seems to play a role in the etiology of RA. A
study on 40 female RA patients who received placebo cap-
sules twice a day in the first month and 500-mg NS oil cap-
sules twice a day in the next month observed that the use
of NS oil capsules notably improved the disease’s activity
Journal of Pharmacopuncture 2017;20(3):179-193
Table 3 Effects of Nigella sativa supplementation on patients with some diseases of the respiratory system
NS, Nigella sativa.
Disease Study design Population
Part of the herb,
dose, and duration
of treatment
Result References
Lower
respiratory
tract
illnesses
-
15 asthmatic
patients
NS boiled extract
(50 and 100 mg/kg)
NS was less effective than
theophylline and salb-
utamol, on pulmonary
function tests
[96]
Controlled
clinical trial
29 asthmatic
adults
15 mL/kg/day of
0.1% NS boiled
extract, 3 months
Prophylactic effects of NS
on asthmatic patients
[97]
Prospective,
randomized,
open study
84 patients of
wheeze associated
LRTI
NS oil (0.1 mg/kg),
14 days
More beneficial effects in
reducing the pulmonary
index and improving the
peak expiratory flow rate
[98]
Randomized,
double-blind,
placebo-
controlled trial
40 chemical war
victims
0.375 mL/kg/day of
50 g NS boiled water
extract,
2 months
Prophylactic effect of NS
on chemical war victims
[99]
Allergic
rhinitis
Single-blind
comparative
clinical trial
47 untreated adult
patients with
seasonal allergic
rhinitis
NS seeds
(250 mg/day),
2 weeks
Decreasing daytime, oph-
thalmic, and nighttime
symptoms
[46]
Double-blind
clinical trial
68 patients with
allergic rhinitis
Nasal drops of NS
oil (each drop: 15
mL oil), 6 weeks
Notable symptomatic
improvement of patients
[47]
Tonsillo-
pharyngitis
Comparative,
parallel, randomized,
double-blind,
placebo-controlled
study
186 acute tonsil-
lopharyngitis
patients
NSPN capsule
(360 mg NS and
50 mg Phyllanthus
niruri extracts),
thrice/day, 7 days
Treatment of the symp-
toms of the disease
[44]](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-9-320.jpg)
![http://www.journal.ac
188
score and alleviated its symptoms, which could be attrib-
uted to the modulatory effect of NS on the immune system
[104].
A clinical trial conducted on osteopenic postmenopausal
women showed that the intake of NS oil (0.05 cc/kg/d) for
three months had no considerable effects on bone turno-
ver markers [40]. Furthermore, in another clinical trial,
in which 15 osteoporotic postmenopausal women were
included, no beneficial effects of consuming NS extract
(0.05 mL/kg/d for three months) on bone turnover were
observed [105].
3.14. Gastrointestinal system
Celiac disease (CD) is characterized by increased sen-
sitivity to gluten and by inflammation and destruction of
the small intestine mucosa due to an autoimmune mecha-
nism. In a study by Osman et al, the prescription of a glu-
ten free diet (GFD) together with the consumption of a
NS oil capsule (450 mg) twice daily as dietary supplement
for one year was more effective than a GFD alone in the
treatment of patients with iron deficiency anemia associ-
ated with refractory CD; i.e., the hematological and im-
munological indices and the duodenal histology recovery
were improved [106]. Dermatitis herpetiformis (DH) is an
autoimmune skin disease caused by CD and is character-
ized by itchiness, a burning sensation, and chronic derma-
titis. Similar to the former CT, adding NS oil capsules to a
GFD for a period of 6 months was found to enhance the
efficacy of a GFD in the treatment of the disease [107]. Fur-
thermore, Mohtashami et al. reported that administration
of a honey-based formulation of NS oil (5 mL NS oil/day),
in comparison with a placebo, for 8 weeks could signifi-
cantly improve the symptoms, such as dyspepsia severity,
and decrease the rate of H. pylori infection in functional
dyspeptic patients [42].
3.15. Anti-toxicity effects
Leukemia is a tumoral growth of WBCs in the bone mar-
row and is caused by a malignant neoplasm of hemat-
opoietic stem cells. In ALL, which is the most common
childhood malignancy [108], increased numbers of lym-
phoblasts are present in the circulating blood and in differ-
ent tissues and organs [48]. A study by Hagag et al reported
that NS oil (80 mg/kg/day) administered for one week after
each methotrexate treatment could reduce hepatotoxicity
and improve the survival rate in ALL children undergoing
that treatment [108]. Table 3.
4. Discussion
This review article summarized different studies on the
clinical uses of NS and TQ in the prevention and the treat-
ment of different diseases. Results indicated that NS has
beneficial effects when used in the therapies for various
diseases, including cardiovascular, nervous system, skin,
infectious, reproductive system, respiratory system, skel-
etal system, and gastrointestinal diseases. Taken together,
the role of NS in the treatment of different diseases is dis-
cussed in the following sentences.
Dyslipidemia plays an important role in the genesis of
cardiovascular diseases (CVDs) [71], and hypercholeste-
rolemia is the most important risk factor for atheroscle-
rosis [72]. Lipid abnormalities are accountable for 56% of
patients with heart disease and 18% of those with an in-
farction; further, it is associated with one third of deaths
worldwide. In this article, we reviewed 19 clinical trials
that reported the ameliorative effect of NS on the lipid pro-
file. This finding shows that the use of NS supplements can
improve the lipid profile and prevent CVDs both in healthy
people and hyperlipidemic patients. The exact mecha-
nisms of the lipid-modifying effects of NS are not known,
but might be associated with the inhibition of intestinal
cholesterol absorption, decreased hepatic cholesterol syn-
thesis, and up-regulation of LDL receptors [74].
On the other hand, dyslipidemia is an important risk fac-
tor responsible for cardiovascular disease in patients with
diabetes [109], so alleviation/elimination of lipid abnor-
malities is important in the prevention of the complica-
tions of diabetes [79]. Thus, keeping the lipid profile of dia-
betic patients in the normal range can improve their health
status, and NS intake, in combination with anti-diabetics
and statins or fibrates, can help diabetic patients to control
both dyslipidemia and blood sugar. We also reported the
results of 13 clinical trials that presented data on the hy-
poglycemic effect of NS, 8 of which included patients with
insulin resistance. The results showed that the use of black
seed could decrease the HbA1c (5 studies) and the PPBG
(2 studies) levels significantly.
Obesity is typically associated with increased risk factors
of CVDs. Therefore, a therapeutic approach that aims to
control body weight and the metabolic profile might be ef-
fective in preventing CVDs [62]. The results of this review
demonstrate that the use of NS may have a weight-lose ef-
fect in obese men and women. Because of the lipid-mod-
ifying, hypoglycemic, and weight-lowering effects of black
seed, its use in the treatment of patients with metabolic
syndrome may be beneficial [21].
According to some studies reviewed, NS may be a useful
herb for improving sexual function because of its inhibito-
ry effect on prolactin [51] and excitatory effect on testoster-
one [33]. In addition, spermatogenesis can be stimulated
by NS [95]. Consequently, it presents a good option for use
in the treatment of infertile men. However, more studies
are needed due to the lack of an adequate number of stud-
ies proving this effect.
TQ has an antioxidant role, improves the body's defense
system, induces apoptosis, and controls the Akt pathway
[7]. Immune system modulation is one of the most impor-
tant properties of NS, and a number of studies have been
done in order to prove this significant effect. In this article,
we reviewed five studies that directly showed the immuno-
modulatory effect of NS [39, 44, 104, 106, 107]. In addition,
other investigations have demonstrated that NS may be an
optimum choice for treating patients with allergy-related
diseases, such as asthma, atopic eczema and allergic rhini-
tis [110].
Journal of Pharmacopuncture 2017;20(3):179-193](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-10-320.jpg)
![http://www.journal.ac 189
Moreover, the anti-nociceptive effect of NS has been
widely investigated in animal models, and a few studies
have evaluated that effect in humans. In this paper, the
anti-microbial activities of NS against bacteria, viruses,
and parasites have also been highlighted. The conclusion
is that it can be used in the treatment of infectious diseases
[111].
Theexistingdrugsforsomediseasesproduceadverseside
effects, do not lead to complete recovery, or are sometimes
expensive. Thus, herbal medicines, such as NS, can be use-
ful alternatives; however, before such herbal medicines are
used extensively, many RCTs should be conducted in or-
der to evaluate and confirm the effects of herbal medicines
[46, 48, 108]. One obvious example is sero-reversion in
HIV-infected patients. Highly active anti-retroviral therapy
does not cause sero-reversion in HIV-infected patients.
Onifade et al proved that NS contributes to sustained sero-
reversion in patients with HIV infection [91, 92].
Some authorities, despite achieving positive outcomes
for the features of NS, suggest further investigations with
larger samples and groups, diverse doses of NS, and longer
periods of study [42, 83-85, 93, 97-99]. After the beneficial
effects of NS have been confirmed, it can be used in treat-
ment protocols. In contrast, some authors have reached
results that conflict with the traditional beliefs about NS.
Actually, the evidence for the positive effects of NS in the
treatment of osteopenic postmenopausal women and
intractable epileptic children is conflicting [40, 82, 105].
Therefore, more studies should be planned in these situ-
ations.
5. Conclusion
In conclusion, the use of black seeds and their active
constituent TQ has been shown to have multiple useful
effects in the treatments of patients with several diseases,
such as inflammatory and auto-immune disorders, as well
as metabolic syndrome. In this study, we also reviewed
other advantages of NS, e.g., its antimicrobial properties,
anti-nociceptive and anti-epileptic impacts, etc. We found
that the side effects of this herbal medicine did not ap-
pear serious, so it can be applied in clinical trials because
most of its major effects have been shown to be beneficial.
Some properties of NS, such as its hypoglycemic, hypoli-
pidemic, and bronchodilatory properties, are sufficiently
understood so that NS can be used for subsequent phases
of clinical trials or for drug development. However, most
of the other effects and applications of NS require further
clinical and animal studies.
Acknowledgment
The authors thank Mashhad University of Medical Sci-
ences, Mashhad, Iran.
Conflict of interest
Ziaee T, Moharreri N, Hosseinzadeh H. Review of phar-
macological and toxicological effects of Nigella sativa
and its active constituents. J Med Plants. 2012;2(42):16-
42.
Darakhshan S, Bidmeshki Pour A, Hosseinzadeh Cola-
gar A, Sisakhtnezhad S. Thymoquinone and its thera-
peutic potentials. Pharmacol Res. 2015;95-96:138-58.
Ahmad A, Husain A, Mujeeb M, Khan SA, Najmi AK,
Siddique NA, et al. A review on therapeutic potential of
Nigella sativa: a miracle herb. Asian Pac J Trop Biomed.
2013;3(5):337-52.
Mollazadeh H, Hosseinzadeh H. The protective effect
of Nigella sativa against liver injury: a review. Iran J Ba-
sic Med Sci. 2014;17(12):958-66.
Shafiq H, Ahmad A, Masud T, Kaleem M. Cardio-pro-
tective and anti-cancer therapeutic potential of Nigella
sativa. Iran J Basic Med Sci. 2014;17(12):967-79.
Butt MS, Sultan MT. Nigella sativa: reduces the
risk of various maladies. Crit Rev Food Sci Nutr.
2010;50(7):654-65.
Khan MA, Chen HC, Tania M, Zhang DZ. Anticancer
activities of Nigella sativa (black cumin). Afr J Tradit
Complement Altern Med. 2011;8(5):226-32.
Banerjee S, Padhye S, Azmi A, Wang Z, Philip PA,
Kucuk O, et al. Review on molecular and therapeu-
tic potential of thymoquinone in cancer. Nutr Cancer.
2010;62(7):938-46.
Abukhader MM. Thymoquinone in the clinical treat-
ment of cancer: fact or fiction?. Pharmacogn Rev.
2013;7(14):117-20.
Forouzanfar F, Bazzaz BSF, Hosseinzadeh H. Black
cumin (Nigella sativa) and its constituent (thymoqui-
none): a review on antimicrobial effects. Iran J Basic
Med Sci. 2014;17(12):929-38.
Hosseinzadeh H, Fazly Bazzaz BS, Haghi MM. Anti-
bacterial activity of total extracts and essential oil of
Nigella sativa L. seeds in mice. Pharmacologyonline.
2007;2:429-35.
Amin B, Hosseinzadeh H. Black Cumin (Nigella sativa)
and its active constituent, thymoquinone: an overview
on the analgesic and anti-inflammatory effects. Planta
Med. 2015;82(1-2):8-16.
Amin B, Taheri MM, Hosseinzadeh H. Effects of intra-
peritoneal thymoquinone on chronic neuropathic pain
in rats. Planta Med. 2014;80(15):1269-77.
Ali BH, Blunden G. Pharmacological and toxico-
logical properties of Nigella sativa. Phytother Res.
2003;17(4):299-305.
Hosseinzadeh H, Eskandari M, Ziaee T. Antitussive ef-
fect of thymoquinone, a constituent of Nigella sativa
seeds, in guinea pigs. Pharmacologyonline. 2008;2:480-
4.
Salem ML. Immunomodulatory and therapeutic prop-
erties of the Nigella sativa L. seed. Int Immunopharma-
col. 2005;5(13-14):1749-70.
Hosseinzadeh H, Taiari S, Nassiri-Asl M. Effect of
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
The authors declare that there are no conflicts of interest.
References
Journal of Pharmacopuncture 2017;20(3):179-193](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-11-320.jpg)

![http://www.journal.ac 191
sus Nigella sativa for management of seasonal allergic
rhinitis: a single blind comparative clinical trial. Pak J
Med Sci. 2010;26(2):249-54.
Alsamarai AM, Abdulsatar M, Ahmed Alobaidi AH.
Evaluation of topical black seed oil in the treatment of
allergic rhinitis. Antiinflamm Antiallergy Agents Med
Chem. 2014;13(1):75-82.
Dogar MZUH, Adi H, Akhtar MS, Sheikh MA. Prelimi-
nary assessment of efficacy of Nigella sativa seeds in
acute lymphoblastic leukemia in local children. Phar-
macologyonline. 2009;2:769-77.
Arslan E, Sayin S, Demirbas S, Cakar M, Somak NG,
Yesilkaya S, et al. A case study report of acute renal fail-
ure associated with Nigella sativa in a diabetic patient.
J Integr Med. 2013;11(1):64-6.
Bamosa A. Nigella sativa is a safe herbal product. J In-
tegr Med. 2014;12(1):66.
Ibraheim ZZ. Effect of Nigella sativa seeds and total oil
on some blood parameters in female volunteers. Saudi
Pharm J. 2002;10:54-9.
Gelot P, Bara-Passot C, Gimenez-Arnau E, Bene-
ton N, Maillard H, Celerier P. [Bullous drug erup-
tion with Nigella sativa oil]. Ann Dermatol Venereol.
2012;139(4):287-91. French.
Al-Jenoobi FI, Al-Thukair AA, Abbas FA, Ansari MJ,
Alkharfy KM, Al-Mohizea AM, et al. Effect of black seed
on dextromethorphan O- and N-demethylation in hu-
man liver microsomes and healthy human subjects.
Drug Metab Lett. 2010;4(1):51-5.
Lonardo A, Ballestri S, Marchesini G, Angulo P, Loria
P. Nonalcoholic fatty liver disease: a precursor of the
metabolic syndrome. Dig Liver Dis. 2015;47(3):181-90.
Kim B, Feldman EL. Insulin resistance as a key link for
the increased risk of cognitive impairment in the meta-
bolic syndrome. Exp Mol Med. 2015;47:e149.
Najmi A, Haque SF, Naseeruddin M, Khan RA. Effect
of Nigella sativa oil on various clinical and biochemi-
cal parameters of metabolic syndrome. Int J Diabetes
Metab. 2008;16:85-7.
Amin F, Islam N, Anila N, Gilani AH. Clinical efficacy
of the co-administration of Turmeric and Black seeds
(Kalongi) in metabolic syndrome - a double blind ran-
domized controlled trial- TAK-MetS trial. Complement
Ther Med. 2015;23(2):165-74.
Latiff LA, Parhizkar S, Dollah MA, Tajuddin Syed Has-
san S. Alternative supplement for enhancement of re-
productive health and metabolic profile among peri-
menopausal women: a novel role of Nigella sativa. Iran
J Basic Med Sci. 2014;17(12):980-5.
Najmi A, Nasiruddin M, Khan RA, Haque SA. Thera-
peutic effect of Nigella sativa in patients of poor glyc-
emic control. Asian J Pharm Clin Res. 2012;5:224-8.
Lee MJ, Wu Y, Fried SK. Adipose tissue heterogeneity:
implication of depot differences in adipose tissue for
obesity complications. Mol Aspects Med. 2013;34(1):1-
11.
Namazi N, Mahdavi R, Alizadeh M, Farajnia S. Oxida-
tive stress responses to Nigella sativa oil concurrent
with a low-calorie diet in obese women: a randomized,
double-blind controlled clinical trial. Phytother Res.
2015;29(11):1722-8.
Mahdavi R, Namazi N, Alizadeh M, Farajnia S. Effects
of Nigella sativa oil with a low-calorie diet on cardi-
ometabolic risk factors in obese women: a randomized
controlled clinical trial. Food Funct. 2015;6(6):2041-8.
Ni WQ, Liu XL, Zhuo ZP, Yuan XL, Song JP, Chi HS, et
al. Serum lipids and associated factors of dyslipidemia
in the adult population in Shenzhen. Lipids Health Dis.
2015;14:71.
Moeen-ud-din H, Murad S, Fatima A. Placebo control-
led study on comparison of effects of Nigella sativa and
nicotinic acid along with low fat diet and physical ex-
ercise on LDL-cholesterol and HDL-cholesterol. Pak J
Med Health Sci. 2014;8:306-9.
Fatima A, Shad MN, Asrar A, Murad S. Effects of Nigella
sativa on HDL-c body weight. Pak J Med Health Sci.
2014;8(1):122-4.
Ibrahim RM, Hamdan NS, Mahmud R, Imam MU, Saini
SM, Rashid SN, et al. A randomised controlled trial on
hypolipidemic effects of Nigella Sativa seeds powder in
menopausal women. J Transl Med. 2014;12:82.
Ibrahim RM, Hamdan NS, Ismail M, Saini SM, Abd
Rashid SN, Abd Latiff L, et al. Protective effects of Ni-
gella sativa on metabolic syndrome in menopausal
women. Adv Pharm Bull. 2014;4(1):29-33.
Mathews MJ, Liebenberg L, Mathews EH. The mecha-
nism by which moderate alcohol consumption influ-
ences coronary heart disease. Nutr J. 2015;14:33.
Tasawar Z, Siraj Z, Ahmad N, Mushtaq H. The effects of
Nigella sativa (Kalonji) on lipid profile in patients with
stable coronary artery disease in Multan, Pakistan. Pak
J Nut. 2011;10:162-7.
Bamosa AO, Basil A, Sowayan AA, Sowayan SA. Effect
of oral ingestion of Nigella sativa seeds on some blood
parameters. Saudi Pharm J. 2007;2:126-9.
Ahmad Alobaidi AH. Effect of Nigella sativa and Al-
lium sativum coadminstered with simvastatin in dys-
lipidemia patients: a prospective, randomized, double-
blind trial. Antiinflamm Antiallergy Agents Med Chem.
2014;13(1):68-74.
Sabzghabaee AM, Dianatkhah M, Sarrafzadegan N,
Asgary S, Ghannadi A. Clinical evaluation of Nigella
sativa seeds for the treatment of hyperlipidemia: a ran-
domized, placebo controlled clinical trial. Med Arch.
2012;66(3):198-200.
Roufogalis B, Sekhon B. No statistically significant ef-
fects of powdered Nigella sativa (kalonji) seed on se-
rum lipid levels, blood sugar, blood pressure or body
weight in adults. Focus Altern Complement Ther.
2009;14(4):292-4.
Asgary S, Sahebkar A, Goli-malekabadi N. Ameliorative
effects of Nigella sativa on dyslipidemia. J Endocrinol
Invest. 2015;38(10):1039-46.
Sahebkar A, Beccuti G, Simental-Mendia LE, Nobili V,
Bo S. Nigella sativa (black seed) effects on plasma li-
pid concentrations in humans: a systematic review and
meta-analysis of randomized placebo-controlled trials.
Pharmacol Res. 2016;106:37-50.
Kaatabi H, Bamosa AO, Badar A, Al-Elq A, Abou-Ho-
zaifa B, Lebda F, et al. Nigella sativa improves glycemic
controlandamelioratesoxidativestressinpatientswith
type 2 diabetes mellitus: placebo controlled participant
62.
63.
64.
65.
66.
67.
68.
69.
70.
71.
72.
73.
74.
75.
76.
46.
47.
48.
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
Journal of Pharmacopuncture 2017;20(3):179-193](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-13-320.jpg)


![Hindawi Publishing Corporation
Evidence-Based Complementary and Alternative Medicine
Volume 2012, Article ID 696230, 6 pages
doi:10.1155/2012/696230
Review Article
Nigella sativa: A Potential Antiosteoporotic Agent
Ahmad Nazrun Shuid, Norazlina Mohamed,
Isa Naina Mohamed, Faizah Othman, Farihah Suhaimi, Elvy Suhana Mohd Ramli,
Norliza Muhammad, and Ima Nirwana Soelaiman
Department of Pharmacology, Faculty of Medicine, National University of Malaysia (UKM), Kuala Lumpur Campus,
Raja Muda Abdul Aziz Road, 50300 Kuala Lumpur, Malaysia
Correspondence should be addressed to Ima Nirwana Soelaiman, imasoel@medic.ukm.my
Received 2 April 2012; Revised 20 July 2012; Accepted 8 August 2012
Academic Editor: Srijit Das
Copyright © 2012 Ahmad Nazrun Shuid et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly
cited.
Nigella sativa seeds (NS) has been used traditionally for various illnesses. The most abundant and active component of NS is
thymoquinone (TQ). Animal studies have shown that NS and TQ may be used for the treatment of diabetes-induced osteoporosis
and for the promotion of fracture healing. The mechanism involved is unclear, but it was postulated that the antioxidative, and
anti-inflammatory activities may play some roles in the treatment of osteoporosis as this bone disease has been linked to oxidative
stress and inflammation. This paper highlights studies on the antiosteoporotic effects of NS and TQ, the mechanisms behind these
effects and their safety profiles. NS and TQ were shown to inhibit inflammatory cytokines such as interleukin-1 and 6 and the
transcription factor, nuclear factor κB. NS and TQ were found to be safe at the current dosage for supplementation in human with
precautions in children and pregnant women. Both NS and TQ have shown potential as antiosteoporotic agent but more animal
and clinical studies are required to further assess their antiosteoporotic efficacies.
1. Nigella sativa
Nigella sativa is a herbal plant which belongs to Ranuncu-
laceae family. It is also known as black cumin or habatus
sauda, and has a rich historical and religious background.
It is found in the southern region of Asia. It can grow
up to 30 cm and produces pale blue flowers. The fruit is
composed of follicles which contain the seeds, the most
valuable part of the plant. The seeds of Nigella sativa (NS),
which have a pungent bitter taste, are used in confectionery
and liquors. The seed is the source of the active ingredients
of this plant and has been used in Islamic medicine for its
healing powers [1]. Studies have revealed various therapeutic
values of NS such as anticancer, antioxidant, antibacterial,
antifungal, antiparasitic and antiasthmatic [2–7]. NS may
also inhibit renal calculi and improve poultry quality [8, 9].
NS contains 36–38% fixed oils, proteins, alkaloids, saponin,
and 0.4–2.5% essential oil [10]. High-performance liquid
chromatography (HPLC) analysis of NS essential oil revealed
that the main active ingredients were thymoquinone, dithy-
moquinone, thymohydroquinone, and thymol [11]. Among
the compounds identified, thymoquinone (TQ) is the most
abundant, which makes up 30–48% of the total compounds.
This quinine constituent is the most potent and pharmaco-
logically active compound in NS. There were several studies
showing that NS and TQ have beneficial effects on bone and
joint diseases.
2. Osteoporosis
The major bone disease is osteoporosis, a systemic skeletal
disease characterized by low bone mass and microarchitec-
tural deterioration of bone tissue, with a consequent increase
in bone fragility and susceptibility to fracture. According to
World Health Organization (WHO), osteoporosis is defined
as a bone mineral density that lays 2.5 standard deviations
or more below the average value for young healthy women.
In osteoporosis, bone loss occurs especially at the trabecular](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-16-320.jpg)
![2 Evidence-Based Complementary and Alternative Medicine
area when the balance of bone remodeling is tipped towards
bone resorption. The bone loss is associated with bone
biochemical marker changes such as reduction in osteocalcin
level, the marker for bone formation and elevation in cross-
link C-telopeptide, the marker for bone resorption. The
diagnosis of osteoporosis is made using dual emission X-
ray absorptiometry (DEXA) machine but more sophisticated
three-dimensional micro-computed tomography (micro-
CT) is making way for a better diagnosis.
This paper attempts to discuss the beneficial effects of NS
and TQ, its active compound, on osteoporosis and fracture
healing.
3. Postmenopausal Osteoporosis
The main cause of osteoporosis is menopause or estrogen-
deficiency. Several medicinal plants have been studied using
postmenopausal osteoporosis animal model such as soy,
blueberry, achyranthes bidentata, and labisia pumila [12–15].
To date, there is no study of NS or TQ on postmenopausal
osteoporosis animal model. There was a human study on
the effects of NS supplements on the bone markers of
postmenopausal women [16]. It was found that NS supple-
mentation for 3 months to these postmenopausal women
failed to cause any significant changes in the bone markers
levels. The authors concluded that NS was not recommended
for the treatment of postmenopausal osteoporosis. However,
there were several weaknesses in the study which may
account for the nonsignificant results. The sample size of
only 15 postmenopausal women was too small. The duration
of study should be longer to obtain bone markers readings at
several time points and to register any changes in the bone
mineral density. Noncompliant in taking NS oil was also a
problem due to the nonfavorable greasy taste. In the future, a
long term study with larger sample size should be planned.
NS in the form of capsules should be given to the study
participants to improve compliance. Before that, the effects
of NS should be tested in animal osteoporosis models. In
vitro studies are also required to determine the effects of NS
on osteoblasts and osteoclasts.
4. Diabetes-Induced Osteoporosis
Currently, NS has only been tested in animal osteoporosis
model of diabetes-induced osteoporosis. No study has been
conducted on other osteoporotic animal models. Osteoporo-
sis is now accepted as a major complication of patients
with diabetes mellitus. Diabetes could affect bone through
multiple mechanisms such as insulin deficiency, insulin resis-
tance, hyperglycemia, or atherosclerosis. However, the exact
mechanism responsible for osteopenia in diabetes is still
unknown [17]. Insulin and insulin-like growth factors (IGF-
1) may have some roles to play in the pathogenesis of
diabetic-induced bone loss due to their anabolic effects [18].
A study found that combined treatment of NS and
parathyroid hormone was more effective in reversing the
osteoporotic changes and improving the bone strength of
steptozocin-induced diabetic rats than either treatment alone
[19]. In another study using the same model, histological
assessments found that NS was able to ameliorate diabetic
changes of the bone [20]. These findings suggested that
NS has potential to be used for the treatment of diabetic
osteoporosis.
The mechanisms behind the bone protective effects of
NS against diabetes induced-osteoporosis are still unclear.
NS may have improved the bone metabolism by improving
the blood sugar levels. In certain parts of the world, NS
is frequently used as the traditional treatment of diabetes
[21]. Studies on streptozotocin-induced diabetic rats have
shown that NS may reduce hyperglycaemia, increase serum
insulin concentrations, and promote partial regeneration or
proliferation of pancreatic beta cells, causing an increase in
insulin secretion [22–25]. In other study, NS treatments of
diabetic rats have been shown to increase the area of insulin
immunoreactive beta-cells. These results have shown that NS
may be used as an effective antidiabetic therapy [19]. There
is a possibility that NS may have exerted its antiosteoporotic
effects in diabetes by improving the blood sugar profile, but
further studies are required to confirm this.
Besides that, previous literatures on NS and TQ have
highlighted two properties that may be responsible for their
antiosteoporotic effects, that is, antoxidative and antiinflam-
matory properties.
5. The Antioxidant Role of NS and
TQ against Osteoporosis
Osteoporotic patients were found to be under oxidative
stress as their lipid peroxidation levels were elevated and
antioxidant enzymes reduced [26, 27]. Most risk factors
for osteoporosis were associated with oxidative stress such
as hypertension [28], diabetes mellitus [29], and smoking
[30]. Exposure to oxidative stress would result in reduction
of bone-mineral density [31]. In bone studies, ferric nitril-
o-triacetate (FeNTA) was used to induce osteoporosis via
oxidative stress [32]. The ferric ions (Fe3+) in FeNTA gen-
erate reactive oxygen species through Fenton reaction [33],
which may damage bone cells by lipid peroxidation [34, 35].
They could also stimulate osteoclast formation and activity
[32, 34, 36], impair osteoblastic function [34, 36], and
decrease osteoblast recruitment and collagen synthesis [35].
Free radicals have also been shown to activate nuclear factor-
kappa B (NFκB) and raised the levels of bone-resorbing
cytokines, interleukin-1(IL-1), and interleukin-6 (IL-6) [32,
37].
Since it is apparent that oxidative stress may lead to
osteoporosis, antioxidants may play a role in protecting bone
against the damaging effects of free-radicals. Studies have
shown that potent anti-oxidants such as tocotrienol and
tocopherol, were able to protect bone against FeNTA (oxi-
dative-stress-) induced osteoporosis [32].
It is interesting to find that the most significant property
of TQ, the active compound of NS, is its antioxidative
activities. It has been reported that the freeradical scavenging
capability of TQ is as effective as superoxide dismutase [38].
It is most effective in scavenging superoxides, the reactive
oxygen species which plays an important role in the activa-
tion of osteoclasts [31]. Since TQ is a potent antioxidant,](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-17-320.jpg)
![Evidence-Based Complementary and Alternative Medicine 3
it is expected that it may be able to protect bone against
osteoporosis due to oxidative stress. In a cancer study, TQ
has been proven to suppress the FeNTA-induced oxidative
stress, hyperproliferative response and renal carcinogenesis
in rats [39]. In studies using rheumatoid arthritis model, TQ
was reported to reduce the serum levels of IL-1 and Tumour
Necrosis Factor-α [40, 41]. The bone turnover markers,
alkaline phosphatase and tartrate-resistant acid phosphatase
were also reduced, indicating stable bone formation and
resorption activities. The NFκB activation was also blocked
by TQ in time-dependent manner [41].
We suspect that the potent antioxidative properties of
NS or TQ may account for the antiosteoporotic effects. Fur-
thermore, the antiosteoporotic effects of tocotrienol, another
potent antioxidant, have been established in several studies
[32, 42].
6. Anti-Inflammatory Role of NS and TQ in
Protecting against Osteoporosis
Inflammation is mediated by two enzymes, cyclooxyge-
nase and lipoxygenase, which generates prostaglandins and
leukotrienes from arachidonic acid, respectively [43]. There-
fore, both prostaglandins and leukotrienes are the main
mediators of inflammation [44]. TQ was believed to exert
anti-inflammatory effects by inhibiting the synthesis of
prostaglandins and leukotrienes [45, 46]. It was found to
inhibit in a dose-dependent manner the cyclooxygenase and
lipoxygenase pathways of rat peritoneal leukocytes that were
stimulated with calcium ionophore A23187 [47].
The antiinflammatory activities of NS were investigated
in vitro, using the cyclooxygenase (COX) assay. TQ was
one of the compounds in NS that was able to inhibit the
COX activity at concentrations comparable to indomethacin,
a nonsteroidal antiinflammatory drug. Therefore, TQ con-
tributed significantly to the anti-inflammatory activities
of NS and has potential to be used as an alternative to
nonsteroidal antiinflammatory drugs [48]. Another possible
antiinflammatory mechanism of TQ might be suppression of
nitric oxide production by macrophages [49].
The anti-inflammatory activity of NS was also demon-
strated in studies using adjuvant-induced arthritis rat model.
Intraperitoneal injections of NS-inhibited carrageenan-
induced paw edema in a dose-dependent manner [50]. Sim-
ilar reduction of formalin-induced paw edema was also
observed with oral treatment of NS [51].
Osteoporosis is known to be caused by various endo-
crine, metabolic, and mechanical factors. Recently, plenty
of evidences had surfaced, linking inflammation to osteo-
porosis. This has led to the opinions that inflammation may
contribute to osteoporosis [52, 53]. Inflammatory conditions
such as ankylosing spondylitis, rheumatoid arthritis and
systemic lupus erythematosus were associated with higher
incidence of osteoporosis [54–57]. The level of C-reactive
protein, a marker of systemic inflammation was also found
to be negatively associated with bone mineral density [58].
The extend of osteoporosis is directly related to the degree
of inflammation, whereby systemic inflammation resulted
in general bone loss, while for local inflammation, bone
loss is restricted to the site of inflammation [52]. Elevations
of proinflammatory cytokines with aging, gouty arthritis,
rheumatoid arthritis and psoriatic arthritis may also con-
tribute to osteoporosis [59–62].
Periodontitis is defined as the inflammation and infec-
tion of the ligaments and bones that support the teeth. A
study has shown that the alveolar bone loss due to periodon-
titis was reduced by gastric feeding of TQ to rats. This was
accompanied by reduction in osteoclast number and raised
osteoblastic activity in TQ-treated rats [63]. The protective
effects of TQ on the alveolar bone were thought to be
contributed by it antioxidative and anti-inflammatory effects
(Figure 1).
7. Effects of NS or TQ on Bone Fracture Healing
To date, there is no study on the effects of NS or TQ on the
complication of osteoporosis, namely osteoporotic fracture.
There is however, an animal study on fracture healing of
nonosteoporotic bone, which resembled traumatic fracture
healing [64]. In this study, anatomical observations indicated
better healing pattern in rats with sustained delivery of TQ. It
was concluded that the sustained levels of TQ may enhance
bone fracture healing. More studies on fracture healing are
required before the effectiveness of NS or TQ in promoting
fracture healing can be concluded. In the most recent study,
TQ was found to accelerate bone formation and shorten
the retention period in rapid maxillary expansion procedure
[65].
8. Toxicity of NS
As in other herbal preparations, safety is one of the important
criteria before NS can be considered for medicinal use. In an
acute toxicity study of NS in mice, toxicity signs were first
noticed after 4 to 6 hours of NS extract administration. The
median lethal dose (LD50) was about 470 mg/kg body weight.
The toxic signs observed were decreased locomotor activity,
decreased sensitivity to touch, and jerking. After 10 hours of
administration, the mice exhibited tachypnoea, prostration,
and reduced food intake [51]. In other acute and chronic
toxicity studies in mice and rats, NS was found to have a wide
margin of safety at therapeutic doses. However, attention
should be paid to the rise in hematocrit and hemoglobin
levels and decrease in white blood cells and platelet counts
[66].
Sustained delivery of TQ for 30 days using Tri-Calcium
Phosphate Lysine (TCPL) capsule loaded with 0.02 grams of
TQ to adult male rats have shown little or no side effects
on the major vital and reproductive organs [64]. In an in
vitro study, TQ at the concentration of 0 to 10 μM was not
cytotoxic to isolated fibroblast-like synoviocytes [41].
The suitable dose for NS extract in human can be
extrapolated from animal studies based on the human
equivalent dose of no observed adverse effect level (NOAEL)
[67]. The human dose is approximately 0.6 mg/kg/day per
oral of TQ [41] or 0.05 mL/kg/day per oral of NS extract,
which was well received by postmenopausal women [16]. NS
extract should be used with precaution in pregnant ladies](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-18-320.jpg)
![4 Evidence-Based Complementary and Alternative Medicine
Increased bone
resorption
Osteoporosis
Free radicals
Osteoclast formation
and activation
Inflammation
Prostaglandins and
leucotrienes
Cyclooxygenase and
lipooxygenase enzymes
Nigella Sativa
or
thymoquinone
Catalyses the reaction
Arachidonic acid
Proposed antiosteoporotic
mechanism 1: neutralizes
the free radicals
Proposed antiosteoporotic
mechanism 2: inhibit these two
enzymes and inhibit inflammation
Activate
NFκB, IL-1, IL-6
Figure 1: The two pathways which may lead to osteoporosis are shown, that is, activation of osteclastic bone resorption activity by free
radicals and by inflammation. The inhibition of these two pathways by Nigella sativa or Thymoquinone, its active component, may account
for the mechanisms involved in prevention of osteoporosis.
and children due to its well-known hypoglycemic properties.
Diabetic patients should consult with their physicians before
taking NS [19, 68]. In children, it was recommended that
NS should be administered in weight-adapted doses and
given after meals [69]. NS at doses below 80 mg/kg was
considered safe in children as there were no adverse effects
being reported [70].
9. Conclusion
NS or TQ has shown potential as a safe and effective antios-
teoporotic agent. However, more studies on the effects of
NS or TQ using various animal osteoporotic models are
required. Once the antiosteoporotic effectiveness of NS or
TQ has been established, human studies can be carried out.
References
[1] W. G. Goreja, Black Seed: Natural Medical Remedy, Amazing
Herbs Press, New York, NY, USA, 2003.
[2] O. A. Badary and A. M. Gamal El-Din, “Inhibitory effects
of thymoquinone against 20-methylcholanthrene-induced
fibrosarcoma tumorigenesis,” Cancer Detection and Preven-
tion, vol. 25, no. 4, pp. 362–368, 2001.
[3] M. Burits and F. Bucar, “Antioxidant activity of Nigella sativa
essential oil,” Phytotherapy Research, vol. 14, no. 5, pp. 323–
328, 2000.
[4] N. M. Morsi, “Antimicrobial effect of crude extracts of Nigella
sativa on multiple antibiotics-resistant bacteria,” Acta Micro-
biologica Polonica, vol. 49, no. 1, pp. 63–74, 2000.
[5] S. H. M. Aljabre, M. A. Randhawa, N. Akhtar, O. M. Alakloby,
A. M. Alqurashi, and A. Aldossary, “Antidermatophyte activity
of ether extract of Nigella sativa and its active principle, thy-
moquinone,” Journal of Ethnopharmacology, vol. 101, no. 1–3,
pp. 116–119, 2005.
[6] M. A. Randhawa, O. M. Alaklobi, S. H. M. Ajabre et al., “Thy-
moquinone, an active principle of Nigella sativa, inhibited
Fusarium solani,” Pakistan Journal of Medical Research, vol. 44,
no. 1, pp. 1–3, 2005.
[7] M. H. Boskabady and B. Shirmohammadi, “Effect of Nigella
sativa on isolated guinea pig trachea,” Archives of Iranian
Medicine, vol. 5, no. 2, pp. 103–107, 2002.
[8] M. A. Hadjzadeh, A. Khoei, Z. Hadjzadeh, and M. Parizady,
“Ethanolic extract of Nigella sativa L seeds on ethylene glycol-
induced kidney calculi in rats,” Urology Journal, vol. 4, no. 2,
pp. 86–90, 2007.
[9] M. T. Islam, A. S. M. Selim, M. A. Sayed et al., “Nigella sativa
L. supplemented diet decreases egg cholesterol content and
suppresses harmful intestinal bacteria in laying hens,” Journal
of Animal and Feed Sciences, vol. 20, pp. 587–598, 2011.](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-19-320.jpg)
![Evidence-Based Complementary and Alternative Medicine 5
[10] B. H. Ali and G. Blunden, “Pharmacological and toxicological
properties of Nigella sativa,” Phytotherapy Research, vol. 17, no.
4, pp. 299–305, 2003.
[11] O. A. Ghosheh, A. A. Houdi, and P. A. Crooks, “High perfor-
mance liquid chromatographic analysis of the pharmacologi-
cally active quinones and related compounds in the oil of the
black seed (Nigella sativa L.),” Journal of Pharmaceutical and
Biomedical Analysis, vol. 19, no. 5, pp. 757–762, 1999.
[12] L. Devareddy, D. A. Khalil, B. J. Smith et al., “Soy moderately
improves microstructural properties without affecting bone
mass in an ovariectomized rat model of osteoporosis,” Bone,
vol. 38, no. 5, pp. 686–693, 2006.
[13] L. Devareddy, S. Hooshmand, J. K. Collins, E. A. Lucas, S. C.
Chai, and B. H. Arjmandi, “Blueberry prevents bone loss in
ovariectomized rat model of postmenopausal osteoporosis,”
Journal of Nutritional Biochemistry, vol. 19, no. 10, pp. 694–
699, 2008.
[14] C. C. He, R. R. Hui, Y. Tezuka, S. Kadota, and J. X. Li,
“Osteoprotective effect of extract from Achyranthes bidentata
in ovariectomized rats,” Journal of Ethnopharmacology, vol.
127, no. 2, pp. 229–234, 2010.
[15] A. N. Shuid, L. L. Ping, N. Muhammad, N. Mohamed, and I.
N. Soelaiman, “The effects of Labisia pumila var. alata on bone
markers and bone calcium in a rat model of post-menopausal
osteoporosis,” Journal of Ethnopharmacology, vol. 133, no. 2,
pp. 538–542, 2011.
[16] N. Valizadeh, H. R. Zakeri, A. Shafiee et al., “The effect
of Nigella sativa extract on biochemical bone markers in
osteopenic postmenopausal women,” Iranian Journal of Endo-
crinology Metabolism, vol. 10, no. 6, pp. 570–580, 2009.
[17] R. Okazaki, “Diabetes mellitus and bone metabolism,” Clinical
Calcium, vol. 21, no. 5, pp. 669–675, 2011.
[18] A. Pater and G. Odrowa̧ż-Sypniewska, “Alterations of bone
metabolism in children and adolescents with diabetes mellitus
type 1,” The Pediatric Endocrinology Diabetes and Metabolism,
vol. 17, no. 3, pp. 158–161, 2011.
[19] M. F. Altan, M. Kanter, S. Donmez, M. E. Kartal, and S.
Buyukbas, “Combination therapy of Nigella sativa and human
parathyroid hormone on bone mass, biomechanical behavior
and structure in streptozotocin-induced diabetic rats,” Acta
Histochemica, vol. 109, no. 4, pp. 304–314, 2007.
[20] A. M. Shady and H. Z. Nooh, “Effect of black seed (Nigella
sativa) on compact bone of streptozotocin induced diabetic
rats,” Egypt Journal of Histology, vol. 33, no. 1, pp. 168–177,
2010.
[21] A. Tahraoui, J. El-Hilaly, Z. H. Israili, and B. Lyoussi, “Ethno-
pharmacological survey of plants used in the traditional treat-
ment of hypertension and diabetes in south-eastern Morocco
(Errachidia province),” Journal of Ethnopharmacology, vol.
110, no. 1, pp. 105–117, 2007.
[22] M. Kanter, I. Meral, Z. Yener, H. Ozbek, and H. Demir,
“Partial regeneration/proliferation of the β-cells in the Islets
of Langerhans by Nigella sativa L. in streptozotocin-induced
diabetic rats,” Tohoku Journal of Experimental Medicine, vol.
201, no. 4, pp. 213–219, 2003.
[23] M. Kanter, O. Coskun, A. Korkmaz, and S. Oter, “Effects of
Nigella sativa on oxidative stress and β-cell damage in strep-
tozotocin-induced diabetic rats,” Anatomical Record—Part A,
vol. 279, no. 1, pp. 685–691, 2004.
[24] H. Rchid, H. Chevassus, R. Nmila et al., “Nigella sativa seed
extracts enhance glucose-induced insulin release from rat-
isolated Langerhans islets,” Fundamental and Clinical Pharma-
cology, vol. 18, no. 5, pp. 525–529, 2004.
[25] Z. A. Hawsawi, B. A. Ali, and A. O. Bamosa, “Effect of Nigella
sativa (black seed) and thymoquinone on blood glucose in
albino rats,” Annals of Saudi Medicine, vol. 21, no. 3-4, pp. 242–
244, 2001.
[26] A. N. Sontakke and R. S. Tare, “A duality in the roles of
reactive oxygen species with respect to bone metabolism,”
Clinica Chimica Acta, vol. 318, no. 1-2, pp. 145–148, 2002.
[27] D. Maggio, M. Barabani, M. Pierandrei et al., “Marked
decrease in plasma antioxidants in aged osteoporotic women:
results of a cross-sectional study,” Journal of Clinical Endo-
crinology and Metabolism, vol. 88, no. 4, pp. 1523–1527, 2003.
[28] F. P. Cappuccio, E. Meilahn, J. M. Zmuda, and J. A. Cauley,
“High blood pressure and bone-mineral loss in elderly white
women: a prospective study,” The Lancet, vol. 354, no. 9183,
pp. 971–975, 1999.
[29] J. O. Christensen and O. L. Svendsen, “Bone mineral in
pre- and postmenopausal women with insulin-dependent and
non-insulin-dependent diabetes mellitus,” Osteoporosis Inter-
national, vol. 10, no. 4, pp. 307–311, 1999.
[30] M. R. Law and A. K. Hackshaw, “A meta-analysis of cigarette
smoking, bone mineral density and risk of hip fracture:
recognition of a major effect,” British Medical Journal, vol. 315,
no. 7112, pp. 841–846, 1997.
[31] S. Basu, K. Michaëlsson, H. Olofsson, S. Johansson, and H.
Melhus, “Association between oxidative stress and bone min-
eral density,” Biochemical and Biophysical Research Communi-
cations, vol. 288, no. 1, pp. 275–279, 2001.
[32] N. S. Ahmad, B. A. K. Khalid, D. A. Luke, and S. I. Nir-
wana, “Tocotrienol offers better protection than tocopherol
from free radical-induced damage of rat bone,” Clinical and
Experimental Pharmacology and Physiology, vol. 32, no. 9, pp.
761–770, 2005.
[33] J. M. C. Gutteridge, D. A. Rowley, and B. Halliwell, “Super-
oxide-dependent formation of hydroxyl radicals and lipid
peroxidation in the presence of iron salts,” Biochemical Journal,
vol. 206, no. 3, pp. 605–609, 1982.
[34] Y. Ebina, S. Okada, S. Hamazaki, Y. Toda, and O. Midorikawa,
“Impairment of bone formation with aluminum and ferric
nitrilotriacetate complexes,” Calcified Tissue International, vol.
48, no. 1, pp. 28–36, 1991.
[35] K. Takeuchi, S. Okada, S. Yukihiro, and H. Inoue, “The
inhibitory effects of aluminum and iron on bone formation,
in vivo and in vitro study,” Pathophysiology, vol. 4, no. 2, pp.
97–104, 1997.
[36] I. R. Garrett, B. F. Boyce, R. O. C. Oreffo, L. Bonewald, J. Poser,
and G. R. Mundy, “Oxygen-derived free radicals stimulate
osteoclastic bone resorption in rodent bone in vitro and in
vivo,” Journal of Clinical Investigation, vol. 85, no. 3, pp. 632–
639, 1990.
[37] A. S. Baldwin, “Control of oncogenesis and cancer therapy
resistance by the transcription factor NF-κB,” Journal of Clini-
cal Investigation, vol. 107, no. 3, pp. 241–246, 2001.
[38] M. A. Nader, D. S. El-Agamy, and G. M. Suddek, “Protective
effects of propolis and thymoquinone on development of
atherosclerosis in cholesterol-fed rabbits,” Archives of Pharma-
cal Research, vol. 33, no. 4, pp. 637–643, 2010.
[39] N. Khan and S. Sultana, “Inhibition of two stage renal carcino-
genesis, oxidative damage and hyperproliterative response by
Nigella sativa,” European Journal of Cancer Prevention, vol. 14,
no. 2, pp. 159–168, 2005.
[40] I. Tekeoǧlu, A. Dogan, L. Ediz, M. Budancamanak, and
A. Demirel, “Effects of thymoquinone (volatile oil of black
cumin) on rheumatoid arthritis in rat models,” Phytotherapy
Research, vol. 21, no. 9, pp. 895–897, 2007.](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-20-320.jpg)
![6 Evidence-Based Complementary and Alternative Medicine
[41] F. Vaillancourt, P. Silva, Q. Shi, H. Fahmi, J. C. Fernandes,
and M. Benderdour, “Elucidation of molecular mechanisms
underlying the protective effects of thymoquinone against
rheumatoid arthritis,” Journal of Cellular Biochemistry, vol.
112, no. 1, pp. 107–117, 2011.
[42] A. S. Nazrun, M. Norazlina, M. Norliza, and S. Ima Nirwana,
“Comparison of the effects of tocopherol and tocotrienol
on osteoporosis in animal models,” International Journal of
Pharmacology, vol. 6, no. 5, pp. 561–568, 2010.
[43] C. S. Williams, M. Mann, and R. N. DuBois, “The role of
cyclooxygenases in inflammation, cancer, and development,”
Oncogene, vol. 18, no. 55, pp. 7908–7916, 1999.
[44] J. van Ryn, G. Trummlitz, and M. Pairet, “COX-2 selectivity
and inflammatory processes,” Current Medicinal Chemistry,
vol. 7, no. 11, pp. 1145–1161, 2000.
[45] P. J. Houghton, R. Zarka, B. D. L. Heras, and J. R. S. Hoult,
“Fixed oil of Nigella sativa and derived thymoquinone inhibit
eicosanoid generation in leukocytes and membrane lipid
peroxidation,” Planta Medica, vol. 61, no. 1, pp. 33–36, 1995.
[46] A. Ghannadi, V. Hajhashemi, and H. Jafarabadi, “An investiga-
tion of the analgesic and anti-inflammatory effects of Nigella
sativa seed polyphenols,” Journal of Medicinal Food, vol. 8, no.
4, pp. 488–493, 2005.
[47] M. Mansour and S. Tornhamre, “Inhibition of 5-lipoxygenase
and leukotriene C4 synthase in human blood cells by
thymoquinone,” Journal of Enzyme Inhibition and Medicinal
Chemistry, vol. 19, no. 5, pp. 431–436, 2004.
[48] M. El-Dakhakhny, M. Barakat, M. Abd El-Halim, and S. M.
Aly, “Effects of Nigella sativa oil on gastric secretion and
ethanol induced ulcer in rats,” Journal of Ethnopharmacology,
vol. 72, no. 1-2, pp. 299–304, 2000.
[49] B. Suna, G. Asha, D. Ferhan et al., “Nigella sativa (black
seed) oil does not affect the T-helper 1 and T-helper 2
type cytokine production from splenic mononuclear cells in
allergen sensitized mice,” Journal of Ethnopharmacology, vol.
100, no. 3, pp. 295–298, 2005.
[50] M. S. Al-Ghamdi, “The anti-inflammatory, analgesic and
antipyretic activity of Nigella sativa,” Journal of Ethnopharma-
cology, vol. 76, no. 1, pp. 45–48, 2001.
[51] Y. Tanko, A. Mohammed, M. A. Okasha, A. Shuaibu, M. G.
Magaji, and A. H. Yaro, “Analgesic and anti-inflammatory
activities of ethanol seed extract of Nigella sativa (black
cumin) in mice and rats,” European Journal of Scientific
Research, vol. 18, no. 2, pp. 277–281, 2007.
[52] D. Mitra, D. M. Elvins, D. J. Speden, and A. J. Collins,
“The prevalence of vertebral fractures in mild ankylosing
spondylitis and their relationship to bone mineral density,”
Rheumatology, vol. 39, no. 1, pp. 85–89, 2000.
[53] A. J. Yun and P. Y. Lee, “Maldaptation of the link between
inflammation and bone turnover may be a key determinant of
osteoporosis,” Medical Hypotheses, vol. 63, no. 3, pp. 532–537,
2004.
[54] G. Hougeberg, M. C. Lodder, W. F. Lems et al., “Hand
cortical bone mass and its associations with radiographic joint
damage and fractures in 50–70 year old female patients with
rheumatoid arthritis: cross sectional Oslo-Truro-Amsterdam
(OSTRA) collaborative study,” Annals of the Rheumatic Dis-
eases, vol. 63, no. 10, pp. 1331–1334, 2004.
[55] I. E. M. Bultink, W. F. Lems, P. J. Kostense, B. A. C. Dijkmans,
and A. E. Voskuyl, “Prevalence of and risk factors for low
bone mineral density and vertebral fractures in patients with
systemic lupus erythematosus,” Arthritis and Rheumatism, vol.
52, no. 7, pp. 2044–2050, 2005.
[56] T. R. Mikuls, K. G. Saag, J. Curtis et al., “Prevalence of
osteoporosis and osteopenia among African Americans with
early rheumatoid arthritis: the impact of ethnic-specific
normative data,” Journal of the National Medical Association,
vol. 97, no. 8, pp. 1155–1160, 2005.
[57] C. Franceschi, M. Bonafè, S. Valensin et al., “Inflamm-aging.
An evolutionary perspective on immunosenescence,” Annals of
the New York Academy of Sciences, vol. 908, pp. 244–254, 2000.
[58] J. R. Arron and Y. Choi, “Bone versus immune system,” Nature,
vol. 408, no. 6812, pp. 535–536, 2000.
[59] K. Ishihara and T. Hirano, “IL-6 in autoimmune disease
and chronic inflammatory proliferative disease,” Cytokine and
Growth Factor Reviews, vol. 13, no. 4-5, pp. 357–368, 2002.
[60] J. K. Kiecolt-Glaser, K. J. Preacher, R. C. MacCallum, C.
Atkinson, W. B. Malarkey, and R. Glaser, “Chronic stress and
age-related increases in the proinflammatory cytokine IL-6,”
Proceedings of the National Academy of Sciences of the United
States of America, vol. 100, no. 15, pp. 9090–9095, 2003.
[61] A. R. Moschen, A. Kaser, B. Enrich et al., “The RANKL/OPG
system is activated in inflammatory bowel diseases and relates
to the state or bone loss,” Gut, vol. 54, no. 4, pp. 479–487, 2005.
[62] N. Saidenberg-Kermanac’h, M. Cohen-Solal, N. Bessis, M. C.
de Vernejoul, and M. C. Boissier, “Role for osteoprotegerin in
rheumatoid inflammation,” Joint Bone Spine, vol. 71, no. 1, pp.
9–13, 2004.
[63] H. Ozdemir, M. I. Kara, K. Erciyas et al., “Preventive effects of
thymoquinone in a rat periodontitis model: a morphometric
and histopathological study,” Journal of Periodontal Research,
vol. 47, no. 1, pp. 74–80, 2012.
[64] P. K. Kirui, J. Cameron, H. A. Benghuzzi et al., “Effects of
sustained delivery of thymoqiunone on bone healing of male
rats,” Biomedical Sciences Instrumentation, vol. 40, pp. 111–
116, 2004.
[65] I. M. Kara, K. Erciyas, A. B. Altan et al., “Thymoqionone accel-
erates new bone formation in the rapid maxillary expansion
procedure,” Archives of Oral Biology, vol. 57, no. 4, pp. 357–
363, 2012.
[66] A. Zaoui, Y. Cherrah, N. Mahassini, K. Alaoui, H. Amarouch,
and M. Hassar, “Acute and chronic toxicity of Nigella sativa
fixed oil,” Phytomedicine, vol. 9, no. 1, pp. 69–74, 2002.
[67] S. Reagan-Shaw, M. Nihal, and N. Ahmad, “Dose translation
from animal to human studies revisited,” The FASEB Journal,
vol. 22, no. 3, pp. 659–661, 2008.
[68] P. M. Le, A. Benhaddou-Andaloussi, A. Elimadi, A. Settaf,
Y. Cherrah, and P. S. Haddad, “The petroleum ether extract
of Nigella sativa exerts lipid-lowering and insulin-sensitizing
actions in the rat,” Journal of Ethnopharmacology, vol. 94, no.
2-3, pp. 251–259, 2004.
[69] M. S. Akhtar and S. Riffat, “Field trial of Saussurea lappa roots
against nematodes and Nigella sativa seeds against cestodes in
children,” Journal of the Pakistan Medical Association, vol. 41,
no. 8, pp. 185–187, 1991.
[70] U. Kalus, A. Pruss, J. Bystron et al., “Effect of Nigella sativa
(black seed) on subjective feeling in patients with allergic
diseases,” Phytotherapy Research, vol. 17, no. 10, pp. 1209–
1214, 2003.](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-21-320.jpg)
![RESEARCH ARTICLE Open Access
Nigella Sativa reverses osteoporosis in
ovariectomized rats
Ansam Aly Seif1,2
Abstract
Background: Osteoporosis poses a significant public health issue. It is a skeletal disorder characterized by
compromised bone strength that predisposes to increased risk of fracture. There is a direct relationship between
the lack of estrogen after menopause and the development of osteoporosis. About 33% of women over 50 will
experience bone fractures as a result of osteoporosis. Nigella Sativa (NS) has been shown to have beneficial effects
on bone and joint diseases. The present study was conducted to elucidate the protective effect of Nigella Sativa on
osteoporosis produced by ovariectomy in rats.
Methods: Female Wistar rats aged 12–14 months were divided into three groups: sham-operated control (SHAM),
ovariectomized (OVX), and ovariectomized supplemented with nigella sativa (OVX-NS) orally for 12 weeks; 4 weeks
before ovariectomy and 8 weeks after. After 12 weeks, plasma levels of calcium (Ca+2
), phosphorous (Pi), alkaline
phosphatase (ALP), amino terminal collagen type 1 telopeptide, malondialdehyde (MDA), nitrates, nitric oxide
surrogate, tumor necrosis factor-α (TNF-α), and interleukin-6 (IL-6) were measured. Histological examination of the
liver and the tibia was conducted. Histomorphometric analysis of the tibia was also performed.
Results: OVX rats showed significant decrease in plasma Ca+2
, accompanied by a significant increase in plasma
ALP, amino terminal collagen type 1 telopeptide, MDA, nitrates, TNF-α and IL-6. These changes were reversed by
NS supplementation in OVX-NS group to be near SHAM levels. Histological examination of the tibias revealed
discontinuous eroded bone trabeculae with widened bone marrow spaces in OVX rats accompanied by a
significant decrease in both cortical and trabecular bone thickness compared to Sham rats. These parameters were
markedly reversed in OVX-NS rats. Histological examination of the liver showed mononuclear cellular infiltration and
congestion of blood vessels at the portal area in OVX rats which were not found in OVX-NS rats.
Conclusion: Nigella sativa reverses osteoporosis in ovariectomized rats, which could be attributed to its high
content of unsaturated fatty acids as well as its antioxidant and anti-inflammatory properties.
Keywords: Osteoporosis, Nigella sativa, Ovariectomy, Rats
Background
The major bone disease is osteoporosis, a systemic skeletal
disease characterized by low bone mass and microarchi-
tectural deterioration of bone tissue, with a consequent in-
crease in bone fragility and susceptibility to fracture. The
main cause of osteoporosis is menopause or estrogen-
deficiency [1]. The increasing evidence of postmenopausal
osteoporosis and its related fractures have become global
health issues recently [2]. Although hormone replacement
therapy has been proven to be efficacious in preventing
bone loss, yet, it is not desirable to many women due to
its side effects [3].
The use of natural products as an alternative to conven-
tional treatment in healing and treatment of various di-
seases has been on the rise in the last few decades. Nigella
sativa, a natural herb which belongs to Ranunculaceae
family, has long been used as a natural medicine for treat-
ment of many acute, as well as, chronic conditions. It is
also known as black cumin or habatus sauda. The seed
is the source of the active ingredients of this plant [4].
Nigella sativa seed oils constitute a good alternative source
of essential fatty acids compared with common vegetable
Correspondence: ansamseif@yahoo.com
1
Physiology Department, Faculty of Medicine, Ain Shams University,
Abbassiya, Cairo, Egypt
2
Postal address: 12 Abdullah Abu Elseoud Street, Triumph, Heliopolis, Cairo,
Egypt
© 2014 Seif; licensee BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons
Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and
reproduction in any medium, provided the original work is properly cited.
Seif BMC Complementary and Alternative Medicine 2014, 14:22
http://www.biomedcentral.com/1472-6882/14/22](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-23-320.jpg)
![oils and could contribute to the overall dietary intake. On
the other hand, in terms of both quantity and quality,
these seeds are potentially attractive source of protein,
lipid and some common minerals that appear to have a
very positive effect on human health [5]. Nigella sativa
seed extracts and its oil have been exploited for their
various health benefits. Studies have revealed various
therapeutic values of NS such as anticancer, antioxidant,
antibacterial, antifungal, antiparasitic and antiasthmatic
[6]. Besides that, previous literatures on NS and thymo-
quinone (TQ), the main active ingredient of NS, have
shown that they have beneficial effects on bone and joint
diseases [6].
To our knowledge, there is no study of NS or TQ on
postmenopausal osteoporosis animal model. In view of
the aforementioned data, the present study aimed to test
the efficacy of NS in mitigating or prevention of post-
menopausal osteoporosis using the ovariectomized rat
model.
Methods
The present study was conducted in the Physiology
Department, Faculty of Medicine, Ain Shams University,
and approved by Faculty of Medicine Ain Shams Univer-
sity (FMASU), Research Ethics Committee (REC), Cairo,
Egypt, which conforms to the Guide for the Care and Use
of Laboratory Animals published by the US National Insti-
tutes of Health. This study was performed on 30 female
Wistar rats aged 12–14 months. Rats were maintained
under standard conditions of boarding. They were fed
standard laboratory chow with free access to water. Rats
were allocated into 3 groups: a) SHAM-operated control
(SHAM) rats (n = 10), b) Ovariectomized (OVX) rats
(n = 10), c) Nigella Sativa-supplemented Ovariectomized
(OVX-NS) rats (n = 10) which received a dose of 800 mg/kg
body weight of nigella sativa daily for 12 weeks, 4 weeks
before ovariectomy and continued for 8 weeks after the
operation. This dose was chosen because it corresponds
to the submaximal dose of thymoquinone (TQ), the active
ingredient of nigella sativa, producing hypotensive effect
in rats [7]. NS seeds (Bioextract (Pvt) Ltd, Sri Lanka,
www.bioextracts.lk) were provided in the form of 500 mg
capsules of grounded NS (powder). The powder was
added to distilled water at room temperature to prepare a
crude suspension of nigella sativa, a few minutes before
giving it to rats by oral gavage. An equivalent volume of
water was administered by the same route to the other
groups of rats.
Bilateral ovariectomy and sham operation were per-
formed under ether anaesthesia. A midline longitudinal
incision was made inferior to the rib cage. The ovaries
of rats in groups OVX and OVX-NS were exteriorized,
ligated and excised. The SHAM-operated control rats
had their dermal integuments, muscles and peritoneum
sectioned, without excision of the ovaries.
Experimental procedures
On the day of the experiments, overnight fasted rats
were weighed and injected intraperitoneally with he-
parin sodium, 1000 IU (B.Braun Melsungen AG.D-34209
Melsungen, Germany). One hour later, rats were anaesthe-
tized with thiopental sodium 40 mg/kg intraperitoneally
(Sandoz, GmbH, Kundl-Austria).
Biochemical analysis
Blood samples were collected from the abdominal aorta,
centrifuged, and then the plasma was subjected to the fol-
lowing assays: calcium (Ca+2
), phosphorous (Pi), alkaline
phosphatase (ALP), amino terminal collagen type 1 telo-
peptide (NTx), malondialdehyde (MDA), nitrates, tumor
necrosis factor-α (TNF-α), and interleukin-6 (IL-6). Tibia
and liver specimens were isolated and processed for histo-
logical examination.
Plasma Ca+2
, Pi
Plasma Ca+2
, Pi were measured using standard labora-
tory methods.
Plasma ALP
Plasma ALP was measured by a kinetic photometric test
using the Alkaline Phosphatase FS kit supplied by DiaSys
Diagnostic Systems GmbH (Germany) according to the
method described by Moss and Henderson [8]. Samples
were added to supplied regents (Diethanolamine pH 9.8 1.2
mol/L, Magnesium chloride 0.6 mmol/L, p-Nitrophenyl-
phosphate 50 mmol/L), incubated at 25°C for 1, 2 and 3
min and absorbance was read 400–420 nm. Calculations
were made from absorbance readings and ALP was
expressed as IU/L.
Plasma NTx
Plasma NTx was measured by a competitive inhibition en-
zyme immunoassay (EIA) method using the Osteomark
NTx plasma kit supplied by Ostex International, Inc.
(USA) according to the method described by Clemens
et al. [9]. Plasma controls, test samples, and calibrators
were added to the antigen-coated 96-well plate. Antibody
to the N-telopeptide cross-links that were conjugated to
horseradish peroxidase were then added to each well. The
wells were then washed to remove unbound material.
Buffered substrate/chromogen reagent was then added to
each well. The reaction was stopped by the addition of
stopping reagent (1N sulfuric acid), which resulted in a
color change from blue to yellow. The absorbance values
for the control, calibrators, and test samples were deter-
mined spectrophotometrically at 450 nm with a 650 nm
reference filter by using a microtiter plate reader. A
Seif BMC Complementary and Alternative Medicine 2014, 14:22 Page 2 of 8
http://www.biomedcentral.com/1472-6882/14/22](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-24-320.jpg)
![standard curve was constructed for each assay by plotting
absorbance versus concentration for each calibrator. The
antigen concentrations of the samples and control were
then read from the curve. Assay values were standardized
to an equivalent amount of bone collagen and are ex-
pressed in nanomoles bone collagen equivalents (nM
BCE/L) per liter.
Plasma MDA assay
Plasma MDA was determined according to the method
of Draper and Hadley [10], based on the reaction of
MDA with thiobarbituric acid (TBA). The reaction was
performed at 95°C for 15 minutes. The sample was
mixed with 2.5 volumes of 10% (w/v) trichloroacetic acid
to precipitate the protein. The precipitate was pelleted
by centrifugation and an aliquot of the supernatant was
allowed to react with an equal volume of 0.67% TBA in
a boiling water bath for 15 minutes. After cooling, the
absorbance was read at 532 nm.
Plasma nitrate assay
Plasma nitrate levels were measured according to the
method of Bories and Bories [11], using an enzymatic one
step methodology based on the reduction of nitrate by
nitrate reductase from Aspergillous species in the pres-
ence of β-NADPH and FAD. The concomitant oxidation
of the coenzyme β-NADPH was monitored by the de-
crease in the absorbance at 340 nm. FAD was used as a
supplementary electron carrier.
Plasma TNF-α assay
Plasma TNF-α was measured by the RayBio® Rat TNF-
alpha ELISA kit (RayBiotech, Inc., Norcross, Georgia,
USA). Standards and samples were pipetted into the wells
and TNF-alpha present in a sample was bound to the
wells by the immobilized antibody. The wells were washed
and biotinylated anti-Rat TNF-alpha antibody was added.
After washing away unbound biotinylated antibody, HRP
conjugated streptavidin was pipetted to the wells. The
wells were again washed, a TMB substrate solution was
added to the wells and color developed in proportion to
the amount of TNF-alpha bound. The Stop Solution
changes the color from blue to yellow, and the intensity of
the color was measured at 450 nm.
Plasma IL-6 assay
Plasma IL–6 was measured using using Rat IL-6 ELISA
kit (Immuno-Biological Laboratories, Inc.) (IBL-America).
Rat IL-6 specific-specific polyclonal antibodies were pre-
coated onto 96-well plates. The rat specific detection poly-
clonal antibodies were biotinylated. The test samples and
biotinylated detection antibodies were added to the wells
subsequently and then followed by washing with PBS or
TBS buffer. Avidin-Biotin-Peroxidase Complex was added
and unbound conjugates were washed away with PBS or
TBS buffer. HRP substrate TMB was used to visualize
HRP enzymatic reaction. TMB was catalyzed by HRP to
produce a blue color product that changed into yellow
after adding acidic stop solution. The density of yellow is
proportional to the rat IL-6 amount of sample captured in
plate.
Histological examination of bone
The tibias were dissected out, fixed in 10% buffered neu-
tral formaldehyde, and decalcified in EDTA solution for 2
weeks. Once decalcified, the specimens followed routine
histological processing and were embedded in paraffin.
Paraffin sections (5 μm thick) from the metaphysis of
tibias were deparaffinized and stained by haematoxylin
eosin (HE) for light microscopic examination [12].
Histological examination of the liver
Liver specimens were fixed in 10% buffered neutral pa-
raformaldehyde solution, processed and embedded in
paraffin. Thin paraffin sections (5 μm) were stained by
HE [12].
Morphometric analysis
The mean cortical bone thickness (CBT) and the mean
trabecular bone thickness (TBT) were measured in 5
fields/slide from 5 slides for each rat. The reading of each
rat was considered as one variable. Measurements were
done using the image analyzer (Leica Q 500 MC program)
in the Histology Department, Ain Shams University.
Statistical analysis
Statistical Package for social sciences (SPSS Inc., Chicago,
IL, USA) version 16 for windows was used for the statis-
tical evaluation of the results. All data were expressed as
mean ± SD. Statistical significance for data was deter-
mined using a one-way analysis of variance (ANOVA)
with post-hoc test, significance calculated by Tukey test to
find inter-group significance. The level of significance was
accepted as P 0.05.
Results
Biochemical parameters
The results of the present study show that plasma Ca+2
levels were significantly decreased in ovariectomized rats
compared to both SHAM and OVX-NS rats. NS sup-
plementation in OVX-NS group restored Ca+2
levels to be
insignificantly different from control SHAM rats, and sig-
nificantly higher compared to OVX rats. Plasma Pi levels
showed no significant changes between the 3 studied
groups. Plasma ALP levels were significantly increased in
ovariectomized rats compared to SHAM group. Although
ALP levels were decreased in OVX-NS compared to OVX
rats, these levels remained significantly higher compared
Seif BMC Complementary and Alternative Medicine 2014, 14:22 Page 3 of 8
http://www.biomedcentral.com/1472-6882/14/22](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-25-320.jpg)

![portal area shows normal branches of hepatic artery, por-
tal vein and bile duct (Figures 6 7). OVX rats showed
mononuclear cellular infiltration and congestion of blood
vessels at the portal area (Figure 8). In OVX-NS rats, there
was less congestion of blood vessels at the portal area
without mononuclear cellular infiltration (Figure 9).
Discussion
The present study highlights the anti-osteoporotic effects
of NS and the possible mechanisms behind these effects
using ovariectomized rats as a model of post- menopausal
osteoporosis. In the present study, ovariectomy in OVX
group resulted in significant hypocalcaemia. These results
are in agreement with Mattix-Kramer et al. [13], who
reported that ovariectomized rats had impaired Ca+2
ba-
lance that could have contributed to ovariectomy-induced
osteoporosis. Moreover, menopause is associated with im-
paired intestinal Ca+2
absorption that could be attributed
to reduced plasma 1,25 dihydroxyvitamin D levels, as well
as to the resistance of the gastrointestinal system to the
action of 1,25 dihydroxyvitamin D [14]. Estrogen has been
shown to modulate the end organ effect of 1,25 dihydro-
xyvitamin D on intestinal calcium absorption [15]. Fur-
thermore, menopause is associated with increased renal
excretion of calcium [16]. Estradiol increases renal tubular
Ca+2
reabsorption [17]. Our results show that NS supple-
mentation in OVX-NS was effective in preventing hypo-
calcemia caused by ovariectomy in OVX rats. Ali et al. [5]
reported that NS seed oils revealed higher degree of unsa-
turation and that the major unsaturated fatty acids were
linoleic acid followed by oleic acid. Oleic acid was found
to increase Ca+2
levels [18]. Oleic acid was also found to
help maintain bone health and prevent calcium loss by
promoting the absorption of nutrients in the body [19].
Martin-Bautista et al. [20], reported improvement of bone
formation biomarkers after 1-year consumption with milk
fortified with oleic acid and other fortifiers with a signifi-
cant increase in plasma calcium (4%), vitamin D (11%),
and osteocalcin (22%). Current evidence in animals also
suggests that linoleic acid may help decrease bone loss by
enhancing calcium absorption [21]. An average woman is
estimated to eat about 2 1/2 lbs of food a day, therefore
0.1–1% of her diet would amount to about 1.14–11.4 g of
linoleic acid a day. Given that dietary linoleic acid intakes
Figure 3 Proximal metaphysis of tibia of the OVX group
showing discontinuous network of bone trabaculae with
widening of bone marrow spaces (HE × 200).
Figure 4 Proximal metaphysis of tibia of the OVX group
showing erosion cavities in bone trabeculae (*) (HE × 1000).
Figure 5 Proximal metaphysis of tibia from OVX-NS group,
showing preserved bone architecture as compared to
ovariectomized (OVX) rat group (HE × 200).
Table 2 Cortical bone thickness (CBT) and trabecular bone
thickness (TBT) in SHAM-operated control (SHAM) rats,
ovariectomized (OVX) rats, and Nigella sativa-supplemented
ovariectomized (OVX-NS) rats
SHAM OVX OVX-NS
CBT (μm) 238.35 ± 5.41 197.10 ± 6.06a,b
236.75 ± 5.84
(n = 5) (n = 5) (n = 5)
TBT (μm) 98.86 ± 2.12 60.78 ± 3.14a,b
93.56 ± 2.70a
(n = 5) (n = 5) (n = 5)
n is the number of observations.
(a)
is the significance calculated by Tukey test, P 0.05 from SHAM-operated
control group.
(b)
is the significance calculated by Tukey test, P 0.05 from OVX-NS group.
Seif BMC Complementary and Alternative Medicine 2014, 14:22 Page 5 of 8
http://www.biomedcentral.com/1472-6882/14/22](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-27-320.jpg)
![in men and women are reported to not exceed 500 mg a
day [22], theoretically the health benefits attributed to
linoleic acid would not likely be observed by diet alone,
but would require supplementation. Moreover, Ali et al.,
[5], reported that NS seeds contain useful quantities of
calcium which makes them a natural source of calcium
supplementation for pregnant and lactating women as
well as for children and elderly people, which might par-
tially explain raised Ca+2
levels seen in OVX-NS rats.
In the current study, plasma ALP was significantly
increased in OVX rats compared to SHAM rats, indica-
ting increased osteoblastic activity with increased bone
formation. OVX rats also showed a significant increase in
plasma NTx levels compared to Sham rats indicating in-
creased bone resorption. Moreover, tibias of OVX rats
showed eroded cavities with widened bone marrow spaces
indicating increased bone resorption. The mean CBT and
TBT were both significantly decreased in OVX rats
compared to Sham rats. These results are in accordance
with Grassi et al. [23], who linked estrogen deficiency to
accelerated bone remodeling, where bone resorption out-
paced bone formation. NS supplementation in OVX-NS
rats lowered plasma ALP levels, albeit still significantly
higher compared to SHAM rats, indicating more stable
bone formation [6]. NS also lowered plasma NTx levels to
levels of control Sham rats, indicating decreased bone re-
sorption to normal control levels. The enhanced effects of
NS supplementation are assured by the elevation of the
mean CBT to control levels, as well as the elevation of the
mean TBT to be very near to control Sham rats, although
still significantly lower.
Besides that, previous literatures on NS and TQ have
highlighted two properties that might be responsible for
their antiosteoporotic effects, that is, antoxidative and
antiinflammatory properties [6]. Histological exami-
nation of liver specimens showed mononuclear cellular
Figure 6 Section in the liver of the SHAM group showing
classic parenchymal hepatic lobules with branching and
anastomosing cords of hepatocytes radiating from the central
vein and separated by blood sinusoids (HE × 200).
Figure 7 Section in the liver of SHAM group where the portal
area shows normal branches of hepatic artery, portal vein and
bile duct (HE × 200).
Figure 8 Section in the liver of OVX rats showing mononuclear
cellular infiltration and congestion of blood vessels at the
portal area (HE × 200).
Figure 9 Section in the liver of OVX-NS group showing less
congestion of blood vessels at the portal area without
mononuclear cellular infiltration (HE × 200).
Seif BMC Complementary and Alternative Medicine 2014, 14:22 Page 6 of 8
http://www.biomedcentral.com/1472-6882/14/22](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-28-320.jpg)
![infiltration and congested blood vessels in OVX-NS
rats. Recently, plenty of evidences had surfaced, linking
inflammation to osteoporosis. This has led to the opinions
that inflammation may contribute to osteoporosis [24].
Kireev et al. [25], reported that pro-inflammatory cyto-
kines TNF-alpha (TNF- α), IL-1beta and IL-6 measured in
liver homogenates were significantly increased and anti-
inflammatory IL-10 decreased during ageing and after
ovariectomy in rats. Moreover, Levels of lipid peroxides in
the liver homogenates as well as iNOS protein expression
and NO levels were increased in old rats as compared to
young animals; this effect was more evident in ovariecto-
mized animals. The authors also stated that administra-
tion of the different hormonal replacement therapies was
able to inhibit the induction of pro-inflammatory cyto-
kines and iNOS, decreased the levels of oxidative stress
markers and had therapeutic potential in the prevention
of liver injury. Moreover, Pighon et al. [26], showed that
exercise training in ovariectomized rats acted like estrogen
in properly regulating the expression of inflammatory bio-
markers in liver of OVX rats. TQ was believed to exert
anti-inflammatory effects by inhibiting the synthesis of
prostaglandins and leukotrienes which are the main me-
diators of inflammation [27]. The results of the present
study show significant elevation of plasma nitrates, NO
surrogate, in OVX rats compared to SHAM rats, which
was lowered to control levels by NS supplementation in
OVX-NS group. NO might have been produced by
macrophages as one of the inflammatory signs that were
corrected by NS supplementation. These results are in
agreement with Suna et al. [28], who stated that a possible
anti-inflammatory mechanism of TQ might be suppres-
sion of nitric oxide production by macrophages. Another
study has shown that the alveolar bone loss due to peri-
odontitis was reduced by gastric feeding of TQ to rats.
This was accompanied by reduction in osteoclast number
and raised osteoblastic activity in TQ-treated rats [29]. In
studies using rheumatoid arthritis model, TQ was
reported to reduce the serum levels of IL-1 and TNF-α,
[30]. The production of cytokines including TNF and
IL-17 can increase osteoclastogenesis and bone loss in
inflammatory liver conditions [31]. Bone protective effects
of estrogen might involve suppression of inflammatory
cytokines such as IL-1 and TNF-α, which in turn activate
inducible NO synthase (iNOS). iNOS is only expressed in
response to inflammatory stimuli, and NO derived from
this pathway potentiates cytokine and inflammatory-
induced bone loss [32]. This might be a possible ex-
planation for the detected significant increase in plasma
nitrates level in OVX rats in the present study. Further-
more, a previous study reported that IL-1 and TNF-α were
increased in healthy premenopausal women who under-
went ovariectomy and reached the highest levels 8 weeks
after ovariectomy, and these changes were associated with
indices of bone resorption [3]. In the present study, the
anti-inflammatory effects of NS were further assured by
the significant decrease in plasma TNF-α and plasma IL-6
levels in the OVX-NS group compared to the OVX group.
Osteoporotic patients were found to be under oxida-
tive stress as their lipid peroxidation levels were elevated
and antioxidant enzymes reduced [33,34]. Most risk
factors for osteoporosis were associated with oxidative
stress such as hypertension [35], diabetes mellitus [36],
and smoking [37]. Reactive oxygen species could also
stimulate osteoclast formation and activity [38], impair
osteoblastic function [39], and decrease osteoblast re-
cruitment and collagen synthesis [40]. Exposure to oxi-
dative stress would result in reduction of bone-mineral
density [41]. Increased oxidative stress could be attri-
buted to the loss of the antioxidant effects of estrogen
[3]. Since it is apparent that oxidative stress may lead to
osteoporosis, antioxidants may play a role in protecting
bone against the damaging effects of free-radicals. It has
been reported that the free radical scavenging capability
of TQ is as effective as superoxide dismutase [41]. It is
most effective in scavenging superoxides, the reactive
oxygen species which plays an important role in the acti-
vation of osteoclasts [42]. The results of the present
study are in agreement with the previous data showing
that plasma MDA levels, an important measure of lipid
peroxidation, were significantly increased in OVX rats
compared to both SHAM and OVX-NS rats.
Conclusion
It can be concluded that NS has shown potential as a safe
and effective antiosteoporotic agent, which can be attri-
buted to its high content of unsaturated fatty acids as well
as its antioxidant and anti-inflammatory properties.
Competing interests
I declare that I have no competing interests.
Acknowledgements
Special gratitude goes to Dr. Safaa Shaker, assistant professor of histology,
Faculty of medicine, Ain Shams University for performing the histological
results of the present study.
Received: 16 May 2013 Accepted: 7 January 2014
Published: 14 January 2014
References
1. Shuid AN, Ping LL, Muhammad N, Mohamed N, Soelaiman IN: The effects
of Labisia pumila var.alata on bone markers and bone calcium in a rat
model of post-menopausal osteoporosis. J Ethnopharmacol 2011,
133(2):538–542.
2. Potu BK, Rao MS, Nampurath GK, Chamallamudi MR, Prasad K, Nayak SR,
Dharmavarapu PK, Kedage V, Bhat KM: Evidence-based assessment of
antiosteoporotic activity of petroleum-ether extract of Cissus quadrangularis
Linn: On ovariectomy-induced osteoporosis. Ups J Med Sci 2009,
114:140–148.
3. Das UN: Nitric oxide as the mediator of the antiosteoporotic actions of
estrogen, statins, and essential fatty acids. Exp Biol Med 2002, 227:88–93.
4. Goreja WG: Black Seed: Natural Medical Remedy. New York, NY, USA:
Amazing Herbs Press; 2003.
Seif BMC Complementary and Alternative Medicine 2014, 14:22 Page 7 of 8
http://www.biomedcentral.com/1472-6882/14/22](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-29-320.jpg)

![International Journal of Pharmacology Toxicology / 5(1), 2015, 53-61.
53 | P a g e
e - ISSN - 2249-7668
Print ISSN - 2249-7676
ANTI-ISCHEMIC PROPERTIES OF NIGELLA SATIVA AGAINST
CARDIAC AND NON-CARDIOVASCULAR ISCHEMIA
Ahmed A. A. Bader
Department of Pharmacology and Toxicology, Unaizah College of Pharmacy, Qassim University,
Al-Qassim 51452, Kingdom of Saudi Arabia.
ABSTRACT
Ischemic Cardiovascular Diseases (ICVD) may be broadly classified into ischemic coronary heart disease, renal
hypertension, ischemic cerebrovascular disease and peripheral vascular disease. The black seed, Nigella sativa (NS), a
member of the family of ranunculaceae, is commonly used as a natural food additive. NS and its active constituents have been
documented to exhibit antioxidant, hypotensive, calcium channel blockade and diuretic properties which may contribute to
reduce blood pressure and exerting anti-ischemic effects via reduction in sympatheic overactivity and oxidative stress;
suggesting a potential role of NS in the management of cardiovascular diseases as hypertension and ischemic coronary heart
diseases and other non-cardiovascular ischemia. This study aiming for exploring the anti-ischemic properties of NS that
protecting he heart and other vital organs against ischemia and decreasing incidence of myocardial infraction and ischemic-
reperfusion injuries on different body organs in experimental animal models and from clinical trials as found in ischemic heart
patients received NS. The results provide a clear evidence that both the NS oil and its active ingredients, in particular
thymoquinone (TQ), possessing reproducible anti-oxidant effects through enhancing the oxidant scavenger system against
several ischemic insults and suggesting that the regular use of NS seed is recommended for prevention of ischemic cardiac
and non-cardiovascular diseases.
Keywords: NS: Nigella sativa, TQ: thymoquinone, ICVD: Ischemic Cardiovascular Diseases, Anti-oxidant.
INTRODUCTION
Ischemic cardiovascular diseases (CVD) may be
broadly classified into ischemic coronary heart disease,
ischemic renal hypertension, ischemic cerebrovascular
disease and ischemic peripheral vascular disease, in which
the blood supplies to the heart, the brain and the peripheral
vasculature, respectively, are compromised [1]. Various of
vascular ischemia implicates oxygen-derived free radicals
(especially superoxide and hydroxyl radical) and high-
energy oxidants (such as peroxynitrite) are as mediators of
inflammation, shock, and ischemia/reperfusion injury [2].
The oxidantinjury can potentially occur during ischemia
and reperfusion due to an excess production of oxygen
free radicals, a decrease in antioxidant defenses, or both.
Because antioxidants function by removing the
toxicoxygen metabolites; they are generally highly
effective in reducing ischemia-reperfusion injury activity
[3].
MATERIALS AND METHODS
NS is one of the members of Ranunculaceae
family, commonly grows in the Middle East, Eastern
Europe and Eastern and Middle Asia. NS and its oil are
being used as food additives as well as natural remedies
for many ailments forover thousands of years. Many
active ingredients have been isolated from NS, including:
thymoquinone, thymo-hydroquinone, dithymoquinone,
thymol, carvacrol, nigellicine and alphahedrin. In addition,
many pharmacological effects of NS and its active
principles have been identified, such as immune
stimulation, anti-inflammatory, anti-cancer and anti-
microbial activity [4].
Corresponding Author:-Ahmed Abdul-Sabour Ahmed Bader Email:-ahmedpharma7@gmail.com
International Journal of
Pharmacology Toxicology
www.ijpt.org](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-32-320.jpg)
![International Journal of Pharmacology Toxicology / 5(1), 2015, 53-61.
54 | P a g e
NS as a natural remedy has been documented to
possess numerous therapeutic values, including diabetes,
tumors, hypercholesterolemia, hypertension,
inflammation, and gastrointestinal disorders [5-10]. This
study aiming for exploring the anti-ischemic properties of
NS and its constituents against oxidative stress and
ischemic reperfusion injury inducing vascular dysfunction
and in addition to outline the possible mechanisms of
actions underlying these beneficial effects that protecting
heart and other vital organs against ischemia and
decreasing incidence of myocardial infraction and
ischemic-reperfusion injuries on different body organs as
proved from experimental animal models and from
clinical trials in ischemic patients received NS.
Nigella sativa (NS)
The seed oil of NS was found to be rich in
polyphenols and tocopherols. The seeds contain 36–38%
fixed oils, 0.4–2.5% essential (volatile) oil, proteins,
alkaloids, and saponins [11-13]. Thymoquinone (TQ) is
the most pharmacologically active ingredient found
abundantly (30– 48%) in the black seeds, together with its
derivatives such as dithymoquinone, thymohydroquinone,
and thymol [14].
Antioxidant Property of NS
The seed oil of NS is well known for its strong
antioxidant properties [15]. Previous studies have
documented that pretreatment with TQ, the main active
constituents in seed oil, protected organs against oxidative
damage induced by a variety of free radical generating
agents, such as carbon tetrachloride and including the
alkylating agents, cisplatin, and the cardiotoxic anticancer
drug doxorubicin [16-17]. The free radical scavenging
effects of TQ, dithymoquinone, and thymol were tested
against several reactive oxygen species (ROS), and all the
tested compounds from NS exerted strong antioxidant
effects; thymol acted as singlet oxygen quencher, while
TQ and dithymoquinone showed superoxide dismutase
(SOD)-like activity [18].
Pathogenesis of Vascular ischemia
1. Role of Oxidative Stress in atherosclerosis and
vascular dysfunction. The most atherogenic type of plasma
lipids is LDLc component of total serum cholesterol; that
become oxidized by a process of low level oxidation when
bound to the LDL receptor, internalized, and transported
through the endothelium [19]. Oxidation of the serum
LDL may induce a decreased uptake of L-arginine that
may derange the eNOS, leading to over production of
super-oxide free radical ; that induce more vascular
damage due to defect in biosynthesis of NO[20].
Free radicals possess one or more unpaired
electrons in their outer electronic orbits. Free radicals and
ROS are formed continuously in normal physiological
process. ROS are highly reactive and unstable by nature;
hence, they can damage various cellular components
including lipid membranes [21]. Excessive production
leads to oxidative stress with an increase in the formation
of nitrogen-oxygen derivative free radicals as well as a
decrease in antioxidant capacity [22]. Oxidative stress
occurs when there is an imbalance between production of
ROS and antioxidant defence system in favour of the
former [23-24].
Lipid peroxides are derived from polyunsaturated
fatty acid (PUFA) oxidation and are capable to initiate
lipid peroxidation via free radicals chain reaction.
Molinaldehyde acid (MDA) is a major end product of
PUFA peroxidation and is often used as an indicator of
cell injury. Increase in the production of MDA may be due
to the formation of reactive oxidants. Lipid peroxidation
leads to structural changes of the lipid molecules, and the
changes are more severe as lipids are the main constituent
of biological membranes. Generally, lipid peroxides
carrying a risk factor for atherosclerotic complications
strongly producing vascular ischemia .
NO is synthesized predominantly in the vascular
endothelium. Endothelial nitric oxide synthase (eNOS) is
required for the synthesis of NO from amino acid L-
arginine. Reduced NO bioavailability, that is, a reduction
in NO production by free radicals or an increase in
deactivation of NO due to imbalance between antioxidant
and oxidant levels may be the mechanism underlying
endothelium dysfunction that producing vascular
ischemia. Generation of ROS such as superoxide anions
may cause vascular and cellular injury by oxidizing
membrane lipids, proteins, and nucleic acids. Furthermore,
superoxide anions may reduce NO bioavailability by
binding to the gaseous molecule and forming peroxynitrite
which itself is a free radical [25].
2. Evidences of Oxidative Stress Involved in
vascular dysfunction and ischemia. There is a growth
evidence suggesting that vascular dysfunction and
ischemia may be attributable to the increased production
of ROS [26-27]. Oxidative stress may play a vital role in
the development of vascular dysfunction and ischemia via
the following mechanisms: enhanced sequestration of NO
by ROS [28], formation of lipid peroxidation products
[29], and depletion of NOS cofactor (tetrahydrobiopterin)
[30] . Lastly, it may cause functional and structural
changes in vascular wall and blood vessel [31] . These
vascular alterations may be mediated by several ways,
including direct injury to endothelial and vascular smooth
muscle cells, effects on endothelial cell eicosanoid
metabolism, altered redox state, increases in intracellular
free calcium concentration, stimulation of inflammatory,
and growth signalling events [32-33]. Oxidative stress
promotes proliferation of vascular smooth muscle cells as
well as collagen deposition which cause thickening of
tunica media and narrowing of the vascular lumen, which
eventually leads to an increase in the total peripheral
resistance and vascular dysfunction and ischemia [34].](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-33-320.jpg)
![International Journal of Pharmacology Toxicology / 5(1), 2015, 53-61.
55 | P a g e
RESULTS AND DISCUSSION
Possible Pharmacological Actions of NS against
vascular ischemia. The therapeutic properties of NS have
been carried out by various previous experimental and
clinical trials. A wide spectrum of pharmacological
actions of NS have been explored which may include
antidiabetic, anticancer, immunomodulator, analgesic,
antimicrobial, anti-inflammatory, spasmolytic,
bronchodilator, hepato-protective, renal protective, gastro-
protective, antioxidant properties [47-52].
NS exerting pleiotropic vascular properties
effects including cardiac depressant effect, calcium
channels blocking property, and diuretic effect [53]. In
addition, NS was significantly ameliorating the
inflammatory changes in vital organs (liver, kidney and
lungs) and preventing multi-organ dysfunctions in aged
rats and recommending that the dietary supplement of NS
for elderly people can improve their prognosis on
exposure to sepsis [54]. Thymoquinone, the active
constituent of Nigella sativa seeds, is a pharmacologically
active quinone, which possesses several properties
including analgesic and anti-inflammatory actions [55]. It
has been reported that thymoquinone prevents oxidative
injury in various in vitro and in vivo studies in rats [56-
57]. It has been suggested that thymoquinone may act as
an antioxidant agent and prevents membrane lipid
peroxidation in tissues [58]. The mechanism of action is
still largely unknown. But, it seems these effects may be
related to inhibition of eicosanoid generation, namely
thromboxane B2 and leucotrienes B4 (by inhibiting
cyclooxygenase and 5-lipooxygenase, respectively), and
inhibition of membrane lipid peroxidation [59]. Moreover,
it has been demonstrated that NS can significantly prevent
hepatotoxicity [60]. Furthermore, the results obtained
some other experimental studies suggest that the NS seed
extract decreases cerebral ischemia reperfusion injury-
induced pathological stress in the rat model [36].
Although, the exact mechanism of action of anti-ischemic
activities is not clear; NS seed has a variety of anti-
ischemic activities including antioxidant [61, 62],anti-
eicosanoid [63], calcium channel blocker effects [64] and
a decreasing effect on intracellular calcium in mast cells
[65].
Myocardial infarction (MI) is a deleterious
enigma which is the principal cause of death in both
developed and developing countries as a result of
cardiovascular diseases, and has been the object of intense
investigation by clinicians and basic medical scientists
[66]. MI results from the prolonged myocardial ischemia
with necrosis of myocytes due to interruption of blood
supply to an area of heart [67]. The myocardial protective
effect of NS (black cumin) could be due to its protective
activity as result of the presence of phytoconstituents such
as thymoquinone, dithymoquinone, thymohydro-quinone,
thymol, carvacrol, tanethole and 4-terpineol [68].
Furthermore, the previous results indicated that
the prior administration of the black cumin attenuates
isoproterenol induced MI. The cardioprotective effect of
the black cumin is probably related to its ability to
strengthen the myocardial membrane by its membrane
stabilizing action, with a decrease in activity of Creatinine
Kinase-MB (CK-MB) isoenzyme in the serum; suggesting
a protective effect of NS against myocardial injury [37].
Recently, it has been shown that NS oil had a
marked protective action against ischemia/ reperfusion-
induced gastric mucosal lesions, an effect that was
associated with suppression in the levels of lipid peroxide
(LPX) and lactate dehydrogenase (LDH) and an increase
in those of glutathione (GSH) and superoxide dismutase
(SOD) [69]. Ischemic stroke results from a transient or
permanent reduction in the cerebral blood flow, that is
restricted to the territory of a major brain artery [70].
Three major approaches of possible mechanisms had been
investigated to ameliorate ischemia-induced brain damage
by (i) interfering with the excitatory action of glutamate;
(ii) preventing intracellular accumulation of Calcium and
(iii) preventing the destructive actions of reactive oxygen
species [71]. Vascular ischemia can cause an increase in
the lipid peroxidation reaction and elevation in production
of free radicals, which contributes to a secondary damage
of the nervous tissues [72-73].
Diabetes is associated with marked increase in
ischemic heart disease [74]. The form of dyslipidemia, that
is most characteristic of the diabetes has increased
triglyceride and decreased HDL-Cholesterol level [75-76].
Atherosclerosis is a multifactorial progressive disease
characterized by inflammatory, athero-thrombotic and
fibroproliferative changes leading to macro and
microvascular complications with different clinical
sequelae particularly in diabetic persons [77].
Hypercholesterolemia is the major risk factor associated
with the increased incidence of atherosclerosis [78]. It had
been recorded that NS having a favorable impact on total
cholesterol, LDLc, triglycerides and fasting blood sugar,
that was observed in the intervention group with NS oil
capsules in comparison to the control group [39, 79].
There are various mechanisms were proposed for
the lowering of cholesterol by NS seed, the seed may
either inhibit de novo cholesterol synthesis or stimulate
bile acid excretion and both effects would lead to a
decrease in serum cholesterol [80]. The mechanism may
be due to stabilization of atherosclerotic plaques due to
anti-inflammatory effect of NS or its immunomodulatory
effect [81]. It was reported in a previous clinical study that
there was an effective reduction of serum cholesterol by
braka oil (Oil of NS) in hypercholesterolemic patients
[81]. Moreover, it was observed that the influence of
thymoquinoe on doxorubicin-induced hyperlipidemic
nephropathy in rats, that the rats treated with
thymoquinone (10mg/kg/day) for five days significantly
had lowered serum urea, triglycerides and total cholesterol](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-34-320.jpg)
![International Journal of Pharmacology Toxicology / 5(1), 2015, 53-61.
56 | P a g e
[82]. It has been observed that NS is very useful in
treatment of thrombosis due to their lipid reducing, blood
diluting and anti-oxidant property [44].
Oxygen free radicals, produced on reperfusion,
play a critical role in the vascular injury caused by
ischemia-reperfusion [83]. It has been shown that NS has
protective effect against ischemia reperfusion injury to
various organs [59, 69, 84]. Many studies have suggested
the beneficial antioxidant effects of antioxidant nutrients
such as NS, vitamin E, green tea extract, ginkgo biloba
extract, resveratrol and niacin for reducing or preventing
cerebral or muscle injury during ischemia-reperfusion [85,
86]. Furthermore, NS and thymoquinone possessing strong
antioxidant activity that had been shown to decrease
ischemia-reperfusion (I/R) injury in rat hippocampus [87]
or gastric mucosal tissues [69].
Table 1. Significant anti-ischemic effects of NS and its constituents against different cardio and non-cardiac vascular
ischemia in experimental and clinical trials
Reference Study model Constituents Laboratory Findings Conclusion and
Recommendations
[35] Experimental study of
renovascular ischemic
hypertension in rats
NS oil (i.p) 0.2
mL/kg
↓ SBP, tissue MDA, luminol,
and lucigenin CL
↑ tissue Na+ and K+-ATPase
and ↑ plasma NO
↓ plasma CK, LDH, and ADMA
NS seed oil could have a
therapeutic antihypertensive
effect against renovascular
hypertension in ischemic
hypertensive rat.
[36] Experimental study of
four-vessel occlusion
model in rats
NS aqueous (1 g /
kg) and Ethanolic
(1.6 g / kg) extracts
Significant reduction in
neuronal cell injuries
of rat hippocampus
NS seed extracts could have
a therapeutic protective
effects against cerebral
ischemia.
[37] Experimental study of
isoproterenol-induced
myocardial infarction
in rats
Black cumin (150
mg/kg body weight)
intragastrically for a
period of 15 days
Significant ↓ in serum AST,
ALT, LDH, CK, and tissue lipid
profile of TG, cholesterol, free
fatty acids in NS treated rat
groups
Pretreatment with black
cumin offered a protective
effects against isoproterenol
induced myocardial
infarction in rats.
[38] Experimental study of
L-NAME-induced
hypertension in rats
NS seed extract
(p.o) 400mg/kg
Significant ↓ in arterial BP,
SBP, DBP, and serum LDH; ↑
serum NO
Anti-ischemic effect could
be related to thee significant
decrease in blood lipids and
the increase in serum NO
[39] Experimental study of
Experimentally
induced
hypercholesterolemia
in rabbits
NS (5 g/kg/day) p.o NS showed a promising blood
lipid lowering effects when
compared to placebo and also
has a favourable significant
increase in serum HDL
NS recommended as a
dietary supplement for long
term use without toxic
effects for primary
prevention of
hypercholesterolemia and
atherosclerosis and also has
therapeutic potential actions
for ischemic patients with
coronary artery disease.
[40] Experimental study of
hepatic ischemia /
reperfusion injury in
rats
NS oil (0.2 mL/kg)
intraperitoneally,
before ischemia and
before reperfusion
Significant ↓ in serum AST,
ALT, and LDH in treated rats in
comparison with non-treated
rats
Suggested that NS oil
treatment can protect the rat
liver against ischemia-
reperfusion injury
[41] Experimental study of
ischemic / reperfusion
injury of skeletal
muscle in rats
The aqueous (1, 1.5
and 2 g/kg) and
ethanolic extracts
(1.6, 2.4 and 3.2
g/kg) of NS
Extracts of NS had suppressed
the increase of MDA levels in
the rat skeletal muscle and
therefore inhibiting lipid
peroxidation following
ischemia-reperfusion injury.
Concluded that NS extracts
having some protective
effects against skeletal
muscle tissue injury on
exposure to ischemia-
reperfusion and the anti-
ischemic effects could be
due to antioxidant properties
and free radical
scavengering of NS](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-35-320.jpg)
![International Journal of Pharmacology Toxicology / 5(1), 2015, 53-61.
57 | P a g e
[42] Experimental study of
adrenaline-induced
dyslipidemia and left
ventricular
hypertrophy in rats
Injection of NS with
different doses (0.5,
1 and1.5 mg/kg
body weight, BW)
NS showed significant anti-
dyslipidemic effects with
significantly increase in free
radical scavenging activity and
with attenuation of ischemic
cardiomyocyte damage
Suggested that NS having
antidyslipidemic,
antioxidative and
cardioprotectiving effects on
heart and NS might be used
as a therapeutic alternative
or as a combination with
drug in the treatment of
dyslipidemia that increase
risk of cardiac ischemia and
LVH.
[43] Clinical study on
patients with coronary
artery disease
NS seed oil capsules
with the dose (900
mg/ oral per day)
for 8 weeks.
Significant decreased in serum
levels of LDL, TG, VLDL and
total cholesterol after 8 weeks of
treatment, with significant
increase in serum HDL of
treated patients compared with
pre-treated group
NS seed oil can be usefull
in the treatment of mild
dyslipidemia due to its
potential
hypocholesterolemic and
hypolipidemic effects
[44] Clinical study on
patients with stable
coronary artery disease
NS seed powder
500 mg/daily orally
Significant decrease in serum
total cholesterol, LDL,VLDL,
TG after the treatment, with
significant increase in serum
HDL cholesterol after six
months of treatment
NS has ability to reduce
lipid profile which is a
major risk factor for
ischemic coronary artery
disease in cardiac patients.
[45] Clinical study on
patients with mild
hypertension
NS seed extract
100mg/kg and
200mg/kg, orally
per day
Significant ↓ SBP and DBP
(dose dependent)
↓ total and LDL cholesterol
NS seed extract could be
exerting antihypertensive
and hypolipidemic effects;
which may be beneficial for
ischemic hypertensive
diseases by decreasing
serum total cholesterol and
LDL cholesterol
[46] Clinical study on
patients with ischemic
heart disease
NS seeds in a dose
of 200 mg twice
daily; for 3 months
NS exerted beneficial reductive
effects on blood glucose levels
especially in diabetic patients,
with a significant increase in
serum HDL and a decrease in
serum TG after regular intake
of NS
NS could have beneficial
anti-ischemic effects on
patients with ischemic heart
disease after regular intake
for 3 months
Abbreviation
NS: Nigella sativa; L-NAME: L-NG-nitroarginine methyl ester; i.p: intraperitoneal; i.v: intravenous; p.o: per os; TQ:
thymoquinone; De-TQ: de-thymoquinonated; SBP: systolic blood pressure; DBP: diastolic blood pressure; MDA:
malondialdehyde; CL: chemiluminescence; CK: creatine kinase; LDH: lactate dehydrogenase; ADMA: asymmetric
dimethylarginine; NO: nitric oxide; GFR: glomerular filtration rate; GSH: glutathione; LDL: low-density lipoprotein; AST and
ALT ; aspartate and alanine transaminase; LDH; lactate dehydrogenase; CK; Creatine kinase; VLDL; very low density
lipoprotein ; LDL ; Low density lipoprotein; HDL ; high density lipoprotein; TG; triglycerides; NO; nitric oxide ; LVH; left
ventricular hypertrophy
CONCLUSION
The protective anti-ischemic effects of NS
against different vascular ischemia could be possibly
contributed to their multiple pleiotropic effects including
cardiac depressant and/ or calcium channel blockade
actions that are very helpful for decreasing myocardial
oxygen demands and for strengthening myocardial
membrane by its membrane stabilizing action in ischemic
patients, and in addition to this it could be attributed
largely to hypolipidemic and antioxidant properties of NS.
NS is a promising medicinal plant with many therapeutic
properties and this effect could be related to the presence
of active alkaloid components and/or other constituents.
Further studies should be carried out on human to confirm](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-36-320.jpg)











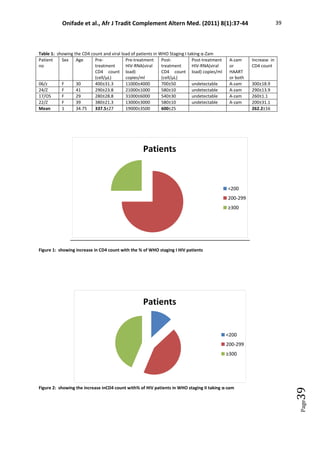
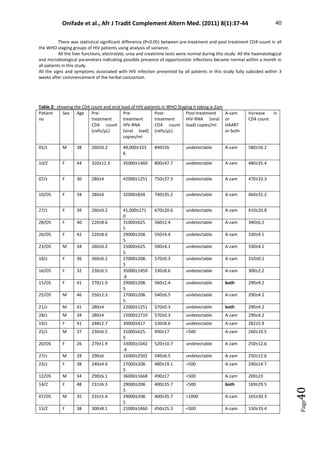





![Tualang honey ameliorates viral load, CD4 counts and improves
quality of life in asymptomatic human immunodeficiency virus
infected patients
Wan Nazirah Wan Yusuf a, *
, Wan Mohd Zahiruddin Wan Mohammad b
, Siew Hua Gan c
,
Mahiran Mustafa d
, Che Badariah Abd Aziz e
, Siti Amrah Sulaiman a
a
Pharmacology Department, School of Medical Sciences, Universiti Sains Malaysia, 16150, Kubang Kerian, Kelantan, Malaysia
b
Biostatistics Unit, School of Medical Sciences, Universiti Sains Malaysia, 16150, Kubang Kerian, Kelantan, Malaysia
c
School of Pharmacy, Building 2, Level 5, Room 40 (2-5-40), Monash University Malaysia, Jalan Lagoon Selatan, 47500, Bandar Sunway, Selangor Darul
Ehsan, Malaysia
d
Infectious Disease Unit, Department of Medicine, Raja Perempuan Zainab II Hospital, 15586, Kota Bharu, Kelantan, Malaysia
e
Physiology Department, School of Medical Sciences, Universiti Sains Malaysia, 16150, Kubang Kerian, Kelantan, Malaysia
a r t i c l e i n f o
Article history:
Received 2 January 2018
Received in revised form
17 May 2018
Accepted 17 May 2018
Available online xxx
Keywords:
Honey
Human immunodeficiency virus
Viral load
CD4 count
Quality of life
a b s t r a c t
This is the first study to report on the effects of honey in asymptomatic HIV positive subjects in
ameliorating CD4 count, viral load (VL) and quality of life (QOL). It is a randomized, controlled, open
labelled study, comparing the effects of Tualang honey (TH) administration for six months at three
different doses: 20 g (THL), 40 g (THI) or 60 g (THH) daily compared with control (no administered
treatment, THC). Only asymptomatic HIV positive subjects (n¼95) having CD4 count 250-600 cell/ml, not
on antiretrovirals were enrolled. Blood, (together with QOL questionnaires administration) were inves-
tigated at baseline, three and six months (CD4 cell count) while VL was determined only at baseline and
six months. Significant reductions in CD4 counts in THL and THC groups (p¼ 0.003 for both) were seen
with no significant reductions in the CD4 counts in THI and THH groups (p¼0.447 and 0.053 respec-
tively). There was improvement in VL in THC and THI (130% and 32% respectively) and reductions in THL
and THH (26% and 8% respectively). Within and between group analyses for VL indicated significant
differences between THL and THH compared to THC. In addition, significant improvement in QOL of
groups which received TH was noted. TH has the potential to improve the QOL (physical and psycho-
logical) and CD4 counts. There was a trend of lower VL in asymptomatic HIV subjects following TH
administration thus supporting the possible role of TH in boosting the immune system by improving CD4
counts, causing VL reductions in HIV positive subjects.
© 2018 Center for Food and Biomolecules, National Taiwan University. Production and hosting by Elsevier
Taiwan LLC. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/
licenses/by-nc-nd/4.0/).
1. Introduction
Human Immunodeficiency Virus (HIV) infection is reported to
be among the top ten leading cause of death in the productive
population in the world.1
Based on the UNAIDS Fact Sheet 2017,
there were 30.8e42.9 million people living with HIV (PLHIV) in
2016, affecting women (52%) and children (6%) with approximately
1.8 million people becoming newly infected with HIV yearly. In
Malaysia, the situation is also similar with an estimated 108,519
PLHIV cases reported and 3330 new HIV cases detected by the end
of 2015. Generally, PLHIV is predominant among Malaysian males
(89%) but over time, the pattern is progressively shifted towards
increasing infection rates in females with declining male to female
ratio [from 9.6 (in 2000) to 5.5 (in 2015)].2
HIV infection is a chronic disease whose progression to acquired
immune deficiency syndrome (AIDS) varies depending on the pa-
tient's state of immunity.3
The introduction of highly active anti-
retroviral therapy (HAART) in 1996 which reduces morbidity and
mortality, prolongs lives and improves quality of life (QOL) of
* Corresponding author.
E-mail address: wnazirah@usm.my (W.N. Wan Yusuf).
Peer review under responsibility of The Center for Food and Biomolecules,
National Taiwan University.
Contents lists available at ScienceDirect
Journal of Traditional and Complementary Medicine
journal homepage: http://www.elsevier.com/locate/jtcme
https://doi.org/10.1016/j.jtcme.2018.05.003
2225-4110/© 2018 Center for Food and Biomolecules, National Taiwan University. Production and hosting by Elsevier Taiwan LLC. This is an open access article under the CC
BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Journal of Traditional and Complementary Medicine xxx (2018) 1e8
Please cite this article in press as: Wan Yusuf WN, et al., Tualang honey ameliorates viral load, CD4 counts and improves quality of life in
asymptomatic human immunodeficiency virus infected patients, Journal of Traditional and Complementary Medicine (2018), https://doi.org/
10.1016/j.jtcme.2018.05.003](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-56-320.jpg)
![infected patients, has dramatically changed the development of
HIV-related disease. Nevertheless, to date, there is still no cure for
HIV and AIDS, both of which require life-long adherence since
treatment does not completely restore immune system integrity.
Currently, the use of HAART is reported to increase the survival rate
of PLHIV while its use is associated with reduced AIDS-defining
opportunistic infections as well as mortality which are directly
related to immune suppression.
In Malaysia, only selected PLHIV are administered with HAART.
Based on the Malaysian Guideline for HIV, many factors should be
considered before commencing patients on HAART including 1)
having CD4 counts 350 cells/mm, 2) patients' willingness to start
and adhere strictly to the treatment as well as during follow-up, 3)
available antiretroviral options, 4) underlying medical diseases
including cardiovascular diseases and diabetes mellitus, 5) the risk
of primary resistance and 6) individual factors which may hinder
adherence such as irregular working hours and lack of social sup-
port.4
The selection is done to ensure that patients on HAART are
compliant to the medications and to avoid the risk of developing
HIV resistant strains. Due to these reasons, only 28% of HIV patients
was reported to be on HAART in Malaysia in 2015.2
HIV infection increases oxidative stress which can result in
further oxidative damage.5
The extent of the damage is influenced
by both the amount of oxidative stress and the host defense
mechanisms both of which may be affected by the intake of dietary
and non-dietary antioxidants and the levels of antioxidant en-
zymes. The activity of the latter may in turn be dependent on the
intake of nutrients required for enzyme activity. In addition, low
plasma selenium concentration during HIV infection is associated
with low glutathione peroxidase activity.6
Significantly higher
oxidative stress and lower concentrations of major plasma anti-
oxidants such as ascorbic acid (vitamin C), alpha tocopherol
(vitamin E), beta-carotene (pro-vitamin A) and selenium have also
been reported in patients compared to seronegative patients.7
Low
levels of antioxidant may hasten disease progression due to
impaired defenses.8
Therefore, in order to boost the defense sys-
tem, many studies have been conducted on supplementation of
PLHIV with micronutrients including the use of selenium, b-caro-
tene9
as well as vitamins A10,11
and E.11
Additionally, due to gastrointestinal malabsorption, increased
metabolic demand, body redistribution, weight loss and muscle
wasting, PLHIV are reported to be more prone to suffering from
multi-nutrient deficiencies especially that of micronutrients.12
Therefore, some HIV patients have been reported to be deficient
in important micronutrients including thiamine, selenium, zinc and
vitamins A, B3, B6, B12, C, D and E.7,13
Moreover, oxidative stress has
been linked to a weakened antioxidant defense system7
thus
contributing to a decreased immunity, increased production of
reactive oxygen species (ROS) as well as a higher risk of disease
progression as well as mortality in PLHIV, indicating the need for
the use of micronutrients.
PLHIV are also at higher risk of developing non-AIDS conditions
such as accelerated aging,14
higher mortality, cardiovascular15
and
other inflammatory-related diseases16
despite having low VL and
high CD4 count17
since low levels of residual viral replication
contribute to residual immune activation and inflammation. Honey
may be a good supplement for HIV patients. It contains at least 181
substances which include vitamins, minerals, trace elements, pro-
teins, enzymes, amino acids and carbohydrates.18,19
Honey also
contains phenolic and flavonoids compounds19,20
which are
important antioxidants that can alleviate chronic inflammation and
stimulate immune cells.21
In addition, honey has antibacterial22
and anticancer properties.23
Interestingly, the oligosaccharides
present in honey has been reported to be rich in bifidobacteria and
lactobacilli both of which can act as prebiotics to alleviate
diarrhoea.24
Honey also shortens the duration of bacterial gastro-
enteritis attributed to its antibacterial properties.19
Besides being
rich in nutrients and antioxidants, honey provides energy where
one tablespoon of honey can supply 64 calories of energy.18
In
addition, honey has anti-inflammatory properties25
which can help
quench the inflammatory effects of residual immune activation and
inflammation. It is thus postulated that honey is an ideal supple-
ment for HIV patients who are at risk of malnutrition, infection and
cancers.
Due to its strong antioxidant, anti-inflammatory effects and the
ability to boost the immune system, it is hypothesized that honey
can improve the immunity of HIV patients, their CD4 counts hence
reducing VL in HIV-positive subjects. To our knowledge, the effects
of honey on immunocompromised patients especially in HIV pos-
itive subjects have not been investigated. Among the different types
of honey present in Malaysia, Tualang honey has been reported to
have a high antioxidant properties26
which may help to improve
the QOL of HIV patients. Thus, the objective of this study was to
investigate the effects of Tualang honey on CD4 counts, the VL and
the QOL in HIV positive subjects with a special focus on patients
who were not given anti-retroviral (treatment naïve) since these
group of individuals are also prone to opportunistic and other in-
flammatory reactions.
2. Materials and methods
2.1. Study subjects
The study was approved by the Ethical Committee of Universiti
Sains Malaysia (USMKK/PPP/JEPeM [198.3 (1)]) which complies
with the Declaration of Helsinki. Subjects were inmates from
Pengkalan Chepa Kota Bharu, Kelantan, Malaysia diagnosed to be
HIV positive with CD4 counts between 250 and 600 cells/ml and
were not on HAART. Written informed consents were signed prior
to enrollment. The enrolled subjects were mostly the unfortunate
ones who do not meet the criteria for HAART due to their poor
social support and difficulty to adhere to treatment and follow up.
2.2. Tualang honey
Tualang honey (AgroMas, Malaysia) was supplied by the Federal
Agriculture Marketing Authority (FAMA) of Malaysia. Honey was
collected by an authorized honey collector and was transported to
the laboratory at room temperature (30 C). It was evaporated to
achieve a 20% water content before being gamma irradiated at
20 Gy to ensure its sterility. It was individually packed in 20 g
sachet each to help standardize the amount administered to all
subjects.
2.3. Study design
This is a randomized, controlled, open-labeled study on the ef-
fects of Tualang honey administered at three different doses for six
months (Fig. 1). Inclusion criteria was PLHIV who were treatment
naïve with CD4 counts 250e600 cell/ml. Exclusion criteria include
AIDS defining illness,27
concurrent chronic diseases such as dia-
betes mellitus, tuberculosis, chronic renal failure and chronic liver
diseases. Demographic data and baseline investigations of CD4
count, VL and assessment of QOL were taken upon recruitment.
Using a block randomization method, the subjects were randomly
divided into four groups. Group THL was administered with honey
20 g daily (low dose), Group THI received 20 g of honey two times
daily (40 g/day, intermediate dose), Group THH received 20 g of
honey three times daily (40 g/day, high dose) while Group THC did
not receive any treatment and served as a control (an acceptable
W.N. Wan Yusuf et al. / Journal of Traditional and Complementary Medicine xxx (2018) 1e8
2
Please cite this article in press as: Wan Yusuf WN, et al., Tualang honey ameliorates viral load, CD4 counts and improves quality of life in
asymptomatic human immunodeficiency virus infected patients, Journal of Traditional and Complementary Medicine (2018), https://doi.org/
10.1016/j.jtcme.2018.05.003](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-57-320.jpg)

![repeated measurements (repeated measure ANOVA) was applied to
investigate the differences in log VL and CD4 counts between the
four groups. A two-sided p-value of less than 0.05 is considered as
statistically significant. There were no p-values for repeated mea-
sures ANOVA between group analyses, with regards to time. If the
mean of the group is outside the confidence interval range of the
compared group, then the difference is considered as statistically
significant.
3. Results
Ninety-five HIV-infected subjects were recruited where the
majority (72.6%) were previous intravenous drug users. Most sub-
jects were males (85.3%) and were unmarried (74.7%) (Table 1).
There was no significant difference in terms of the baseline data for
age, weight, CD4 counts and log VL among the honey-treated
groups as compared to the control indicating that the subjects
were homogenous. This was as expected since block randomization
was performed to ensure that the bias in subject selection is
minimized.
All groups had decreased CD4 absolute counts over the inves-
tigated period (Table 2). However, the reduction in the count was
significant only in groups THC (control group) and THL (low dose
group). Nevertheless, there was no significant difference in mean
CD4 count between all groups when repeated measures ANOVA
between group analysis were performed [F-stat (df) ¼ 0.245,3
p-
value ¼ 0.864].
There was an increase in VL in groups THC and THI (by 130% and
31% respectively) but reductions in groups THL and THH (by 25%
and 8% respectively) (Table 3). There were trends of VL increment in
control group and reduction in treatment group (Fig. 2). However,
the within group analysis were not statistically significant. When
between group analysis was conducted, significant differences
between groups THL and THH as compared to group THC were seen
at six months of treatment (Table 4).
As for the QOL, there were significant difference in the scores for
group THC (control group) in domains 1 (physical; p ¼ 0.045) and 2
(psychological; p ¼ 0.033) based on time (Table 4). There was a
significant difference in the mean score of domains 1 and 2 be-
tween the treatment groups and the control group at three and six
months (Table 5). Fig. 3 illustrates the reductions of the means score
for domains 1 and 2 where the control group had significant re-
ductions in the mean score as compared to the groups treated with
honey which showed improvement in the QOL score.
4. Discussion
To our knowledge, this is the first study to investigate on the
effect of Tualang honey administration on CD4 count and QOL of
HIV-positive subjects. The natural history of HIV infection in un-
treated patients is decreased in CD4 cell counts and an increased VL
where in the later stages, patients are more prone to opportunistic
infections. This phenomenon usually occurs within several years
once CD4 count is less than 200 cells/mm3.28
Nevertheless, the
production of new CD4 cells to counter the dead HIV-induced
lymphocyte cells requires time.
Our study indicated that there were reductions in the CD4
counts of all the treatment groups and the control specifically
groups A (low dose honey) and D (control), showed significant
reductions in CD4 counts. On the contrary, the reduction in CD4
counts were not significant in subjects treated with intermediate
and high doses of honey (groups B and C respectively). As discussed
earlier, even the CD4 counts of patients on antiretroviral therapies
with good VL suppression may not return to normalcy. In fact, there
were reports showing reduction of CD4 or failure of CD4 levels to
return to normalcy even among patients with good VL suppression
following treatment with antiretroviral therapies.29
This phenom-
enon may be due to persistent HIV infections which shorten the life
span of CD4 T-cells,30
causing functional dysregulation.31
Another
plausible explanation for the poor CD4 cell recovery especially in
subjects receiving intermediate and high doses of honey is
apoptosis32,33
secondary to chronic activation of uninfected cells
responding to HIV leading to activation-induced cell death.34
In
addition, reduction in CD4 has been reported to be lower among
naïve CD4 cell productions,34
subsequently leading to reduced
production of CD4 cells.
Our study on honey cannot be compared with that of an anti-
retroviral therapy since the mode of actions are different and
honey is given merely as a supplement, not for treatment. With its
good antioxidant and anti-inflammatory activities, honey con-
sumption is expected to boost the immunity which can help the
body combat infections naturally and are not intended for killing of
the HIV virus. The insignificant reduction in CD4 seen in groups
which received both intermediate and high doses of honey suggests
that the HIV subjects might have benefited from honey adminis-
tration since the decreased in CD4 counts seen was lower than that
Table 1
Baseline characteristics of the subjects.
Characteristics Groups Total F statistics (df) p-value
THL (n ¼ 26) (low dose) THI (n ¼ 24) (intermediate) THH (n ¼ 22) (high dose) THC (n ¼ 23) (control) freq (%)
Mean age (SD) 33.42 (7.65) 32.96 (4.86) 36.50 (7.78) 36.35 (7.29) 1.698 (3,91) 0.173a
Weight (kg) (SD) 56.35 (7.80) 58.75 (8.25) 54.89 (6.83) 58.28 (7.14) 1.287 (3,91) 0.284a
Mean BMI (SD) 21.47 (2.62) 22.22 (3.05) 20.80 (2.40) 22.71 (2.55) 2.159 (3,91) 0.099a
Mean CD4 (SD) 410.41 (104.16) 412.89 (99.84) 414.67 (99.55) 421.28 (82.33) 0.055 (3,91) 0.983a
Mean VL (SD) 74512.14 (149219.59) 61280.85 (91513.23) 64330.82 (57153.31) 79934.44 (95014.57) 0.159 (3,91) 0.924a
Sex
Male 22 (27.2) 20 (24.7) 19 (23.5) 20 (24.7) 81 (85.3) 0.985#
Female 4 (28.6) 4 (28.6) 3 (21.4) 3 (21.4) 14 (14.7)
Marital status
Married 6 (23.1) 5 (20.8) 5 (22.7) 5 (21.7) 21 (22.1) 0.979#
Single 19 (73.1) 19 (79.2) 16 (72.7) 17 (73.9) 71 (74.7)
Divorced or widow 1 (3.8) 0 (0.0) 1 (4.5) 1 (4.3) 3 (3.2)
Transmission
Sexual intercourse 5 (19.2) 10 (41.7) 6 (27.3) 3 (21.7) 24 (25.3) 0.422#
Needle sharing 20 (76.9) 14 (58.3) 16 (72.7) 19 (82.6) 69 (72.6)
Unknown 1 (3.8) 0 (0.0) 0 (0.0) 1 (4.3) 2 (2.2)
a
A one-way ANOVA was applied to compare the means of each group.# A Pearson Chi Square test was applied to compare the means of each group. Normality and ho-
mogeneity of variances assumptions are met for both statistics. SD: Standard deviation, Freq: frequency, BMI: body mass index.
W.N. Wan Yusuf et al. / Journal of Traditional and Complementary Medicine xxx (2018) 1e8
4
Please cite this article in press as: Wan Yusuf WN, et al., Tualang honey ameliorates viral load, CD4 counts and improves quality of life in
asymptomatic human immunodeficiency virus infected patients, Journal of Traditional and Complementary Medicine (2018), https://doi.org/
10.1016/j.jtcme.2018.05.003](https://image.slidesharecdn.com/blackseedoil-casestudy-220915093635-2c05f883/85/Black-Seed-Oil-Case-Study-pdf-59-320.jpg)































