OBJECTIVES
At the endof this lecture, student will be able to:
Explain the mechanism of toxicity, toxicokinetics, clinical signs and symptoms,
investigations and management of benzodiazepine overdose
3.
Introduction
• A benzodiazepine(sometimes colloquially "benzo"; often abbreviated "BZD") is
a psychoactive drug.
• The first such drug, chlordiazepoxide (Librium), was discovered accidentally by Leo
Sternbach in 1955, and made available in 1960 by Hoffmann–La Roche, which has
also marketed the benzodiazepine diazepam (Valium) since 1963
4.
Introduction
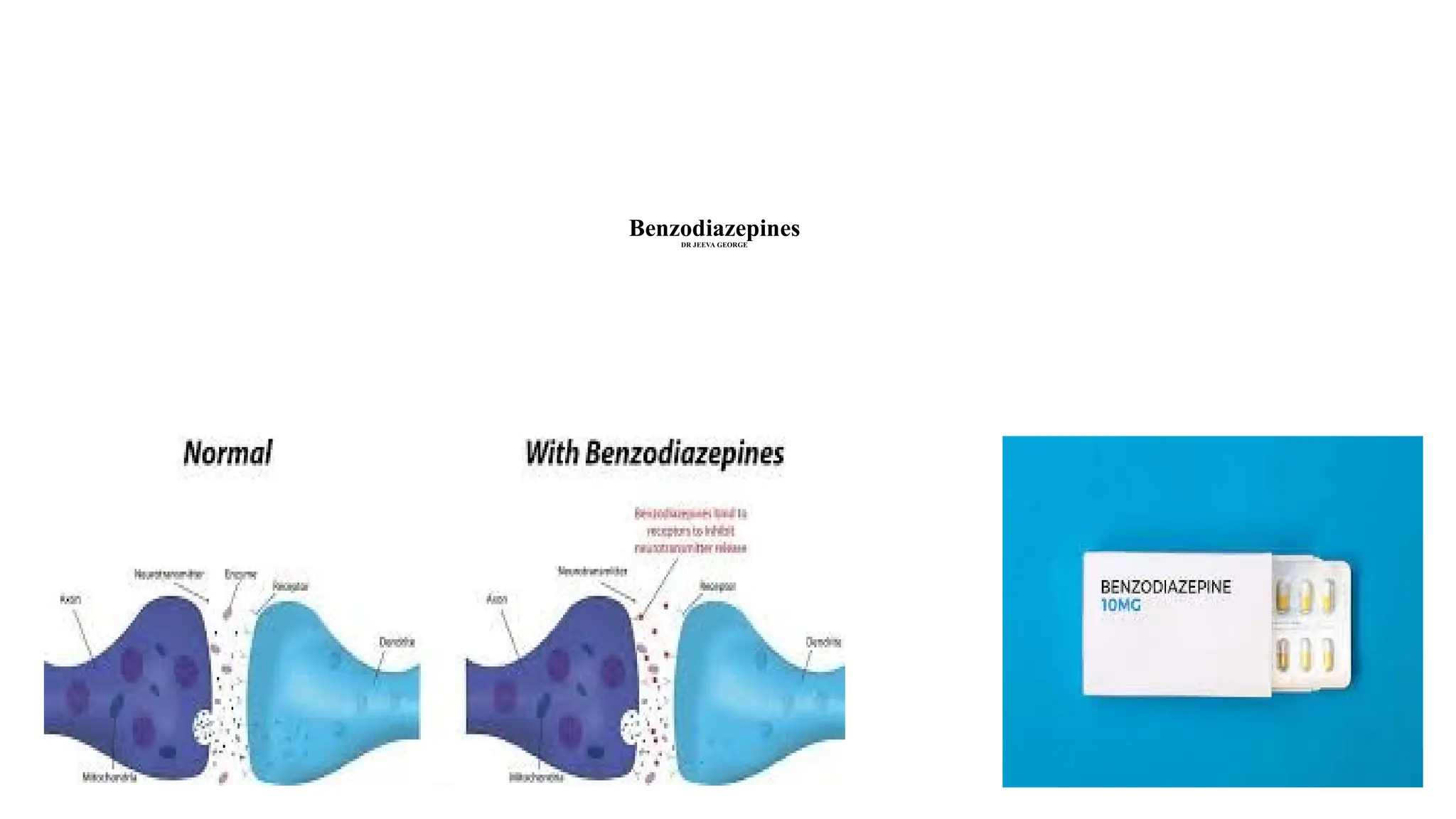
• Benzodiazepines enhancethe effect of the neurotransmitter gamma-aminobutyric
acid (GABA) at the GABAA receptor, resulting in sedative, hypnotic (sleep
inducing), anxiolytic (anti-anxiety), euphoric, anticonvulsant, and muscle
relaxant properties
• Wider therapeutic window and lower drug tolerance for abuse with the
benzodiazepines
5.
Mechanism of actionof benzodiazepines
These compounds act by stimulating the GABAA receptors , thereby
opening up the chloride ion channel in the receptor complex,
resulting in the increased conduction of chloride ion across the nerve
cell membrane.
This lowers the potential difference between the interior and
exterior of the cell, blocking the ability of the cell to conduct nerve
impulses.
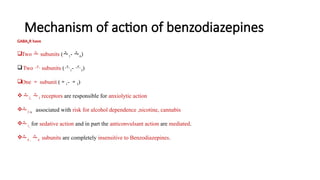
Mechanism of actionof benzodiazepines
GABAAR have
Two subunits (1- 6)
Two subunits (1- 3)
One subunit (1- 3)
2, 3 receptors are responsible for anxiolytic action
2 is associated with risk for alcohol dependence ,nicotine, cannabis
1, for sedative action and in part the anticonvulsant action are mediated.
4 , 6 subunits are completely insensitive to Benzodiazepines.
Uses
• Due tothe ability to calm the mind and body, benzodiazepines are often used to treat
anxiety, panic attacks, insomnia, agitation, muscle spasms, alcohol withdrawal and on
occasion, premedication for medical or dental procedures
• Anxiolytic : diazepam, lorazepam, oxazepam, alprazolam
• Sedative-hypnotic: flurazepam, nitrazepam, triazolam
• Anticonvulsant: Diazepam, clonazepam
• Muscle relaxant: Diazepam
11.
Risk assessment
• Isolatedbenzodiazepine overdose usually causes only mild sedation, irrespective of
the dose ingested, and can be easily managed with simple supportive care
• Alprazolam overdose is associated with greater degree of CNS depression and is
more likely to require intubation and ventilation
• Zolpidem and zopiclone (non-benzodiazepine sedative-hypnotics) rarely cause
severe CNS or respiratory depression when taken alone
12.
Risk assessment (contd)
•Co-ingestion of other CNS depressants (e.g. alcohol, opioids) increases the risk of
complications, prolonged length of stay and death
• The elderly and patients with cardiorespiratory co-morbidities may suffer greater
complications
• Children: Ingestion of one or two benzodiazepines usually manifests as mild sedation
and ataxia within 2 hours
13.
Benzodiazepine Side effects
•Relaxation
• Euphoria
• Sense of wellbeing
• Sedation
• Dizziness
• Impaired vision
• Decreased motor skills/ unsteadiness
• Dizziness
• The side effects of benzodiazepines are increased when paired with other drugs such as
barbiturates, alcohol, narcotics or tranquilizers
14.
Toxic Mechanism
• Benzodiazepinesact by enhancing gamma-amino butyric acid (GABA) mediated
neurotransmission. They bind to the GABAA receptor complex and increase the
frequency of chloride channel opening
• Zolpidem and zopiclone are non-benzodiazepine sedative-hypnotics that also act at
the GABAA receptor complex
15.
Toxicokinetics
• Benzodiazepines arerapidly absorbed orally. Most are highly protein bound and have
volumes of distribution that vary from 0.5 to 4 L/kg
• Benzodiazepines undergo hepatic metabolism
• Many have active metabolites. For example, diazepam is metabolized to N-
desmethyldiazepam, oxazepam and temazepam, and alprazolam is metabolized to 1-
and 4-hydroxyalprazolam
16.
Toxicokinetics
• Duration ofeffect following overdose depends on CNS tolerance and redistribution,
rather than rate of elimination
• Clinical features of intoxication are poorly correlated to serum benzodiazepine levels
17.
Clinical features
Acute poisoning
•Mild—Drowsiness, ataxia, weakness
• Moderate to Severe— Vertigo, slurred speech, nystagmus, partial ptosis (Falling of
upper eye lid), lethargy, coma
18.
Clinical features
• Onsetof symptoms occurs within 1–2 hours. Ataxia, lethargy, slurred speech and
drowsiness are followed by decreased responsiveness
• Apnoea is a complication of airway obstruction
• In very large ingestions hypothermia, bradycardia and hypotension may occur.
Resolution of CNS depression usually occurs within 12 hours
• More prolonged coma is common in the elderly
19.
Clinical features
• Shortacting benzodiazepines (midazolam and triazolam) and intermediate acting
(flunitrazepam) have a higher acute toxicity, as compared to diazepam,
lorazepam and nitrazepam
• Administration of benzodiazepines to a pregnant woman prior to delivery may
produce signs of poisoning in the neonate. A condition called “floppy infant
syndrome”, characterised by hypotonia (muscle weakness) that may last several
days, may occur following maternal diazepam use
20.
Clinical features
Chronic Poisoning
•Long-term use of benzodiazepines is associated with the development of
tolerance
• Abrupt cessation provokes a mild withdrawal reaction characterised by anxiety,
insomnia, head- ache, tremor, and paraesthesia, restlessness
21.
Management
Acute Poisoning
• Decontamination—Ipecac-inducedemesis is not recommended because of the potential for
CNS depression
• Stomach wash may be helpful if the patient is seen within 6 to 12 hours after the ingestion
• Endotracheal intubation is a prerequisite in comatose patients
• Activated charcoal adsorbs benzodiazepines and can be administered in the usual manner
22.
Management
• Establish clearairway
• Oxygen and assisted ventilation are often necessary
• IV fluids (Ringer’s lactate at a rate of 150 ml/hr for adults)
• If hypotension persists, administer dopamine or noradrenaline
• Forced diuresis and haemodialysis are ineffective
23.
Antidotes
• Flumazenil isa competitive benzodiazepine antagonist with a limited role in
benzodiazepine overdose. Its indications include:
• Management of airway and breathing when resources are not available to safely
intubate and ventilate the patient
• Diagnostic tool to avoid further investigation
• Reversal of conscious sedation
24.
Antidotes (contd)
• Flumazenilis a recently discovered pharmacologic antagonist of the CNS effects of
benzodiazepines
• It acts by binding CNS benzodiazepine receptors and competitively blocking
benzodiazepine activation of inhibitory GABA ergic synapses
• Most patients achieve complete reversal of benzodiazepine effect with a total slow IV
dose of just 1 mg
25.
Antidotes (contd)
• Flumazenilalso has the tendency to induce a withdrawal reaction in
benzodiazepine-dependant patients
• Flumazenil is contraindicated in mixed ingestions involving tricyclic
antidepressants and drugs which induce seizures, e.g. theophylline, chloroquine,
etc
26.
Management
Chronic poisoning
• Phenobarbitone-substitutiontechnique is recommended for benzodiazepine
withdrawal which employs propranolol for acute somatic symptoms, while
phenobarbitone is used for detoxification
• However the most frequently used method is the replacement of a short half-life
benzodiazepine (such as alprazolam) with a long half-life benzodiazepine (such as
clonazepam), before initiating a taper and final discontinuation