Download to read offline
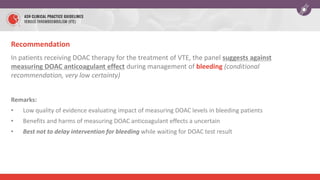
![Recommendation
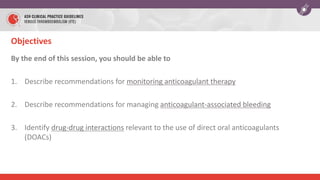
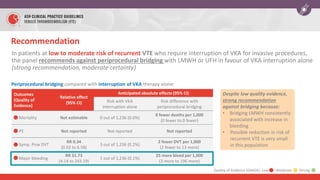
In patients with life-threatening bleeding during dabigatran treatment for VTE, the
panel suggests using idarucizumab in addition to cessation of dabigatran rather than no
idarucizumab (conditional recommendation, very low certainty)
Remarks:
• Compared with non-idarucizumab control group, patients receiving idarucizumab may have had less
worsening or recurrence of bleeding (RR 0.12 [95% CI, 0.03 to 0.43])
• In one cohort study, 6.3% of patients who received idarucizumab for uncontrolled bleeding developed
arterial or venous thrombosis within 90 days
CV Pollack NEJM 2017](https://image.slidesharecdn.com/ashteachingslidesetvteanticoagulationtherapypowerpointfinal71923-240503150343-839c49b2/85/ASH-Teaching-Slide-SetVTEAnticoagulationTherapyPowerpointFINAL71923-pptx-27-320.jpg)

This document outlines the 2018 American Society of Hematology guidelines for managing anticoagulation therapy, focusing on the optimal management of venous thromboembolism (VTE). It includes recommendations on dosing strategies, management of anticoagulant-associated bleeding, and considerations for patients undergoing procedures while on anticoagulants. Key takeaways emphasize adjusting doses based on actual body weight, avoiding certain bridging anticoagulants, and preferential use of 4-factor prothrombin complex concentrate for reversing vitamin K antagonists.


























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







