The document discusses developments at the Aravind Eye Care System in 2009. Key points include:
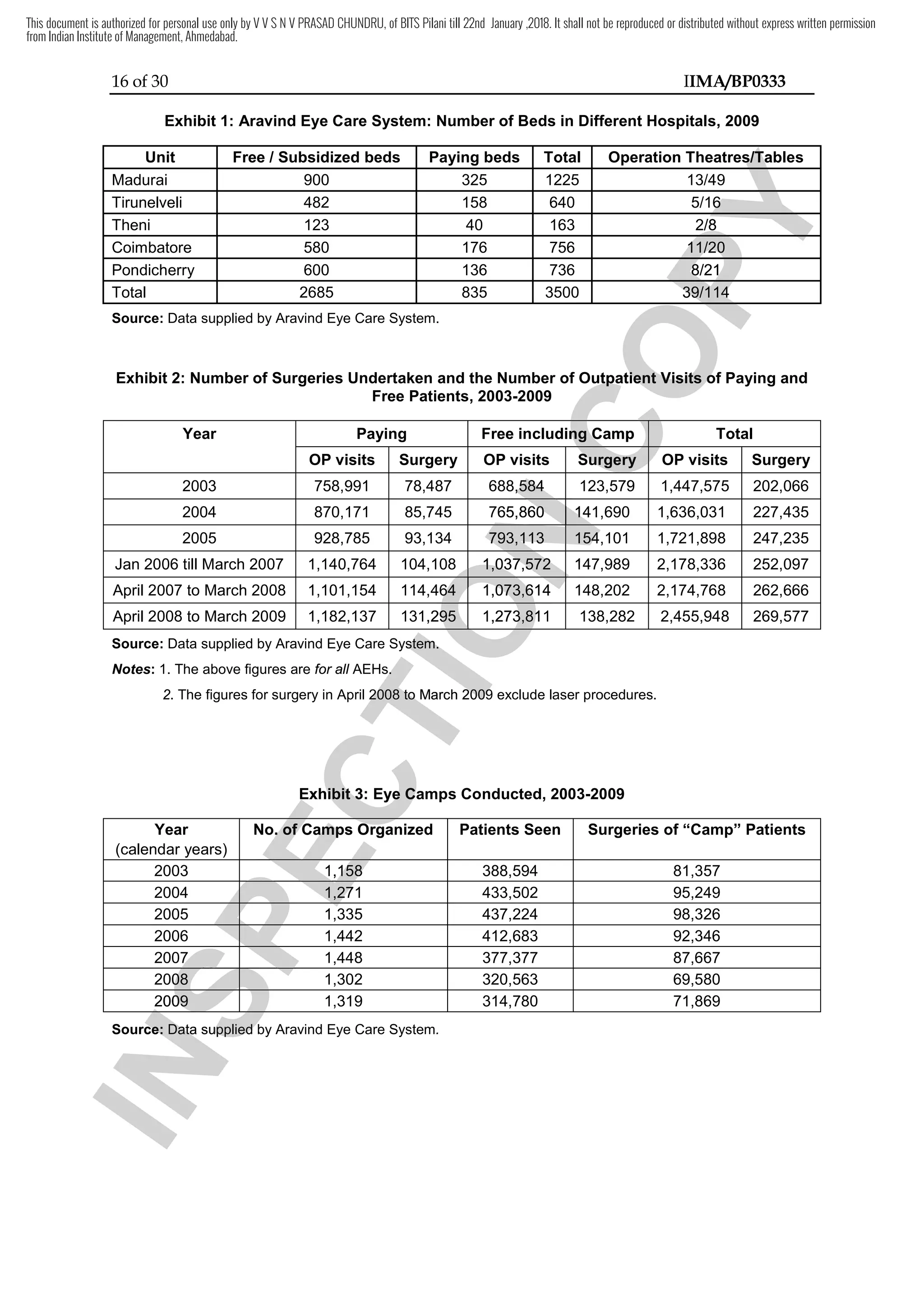
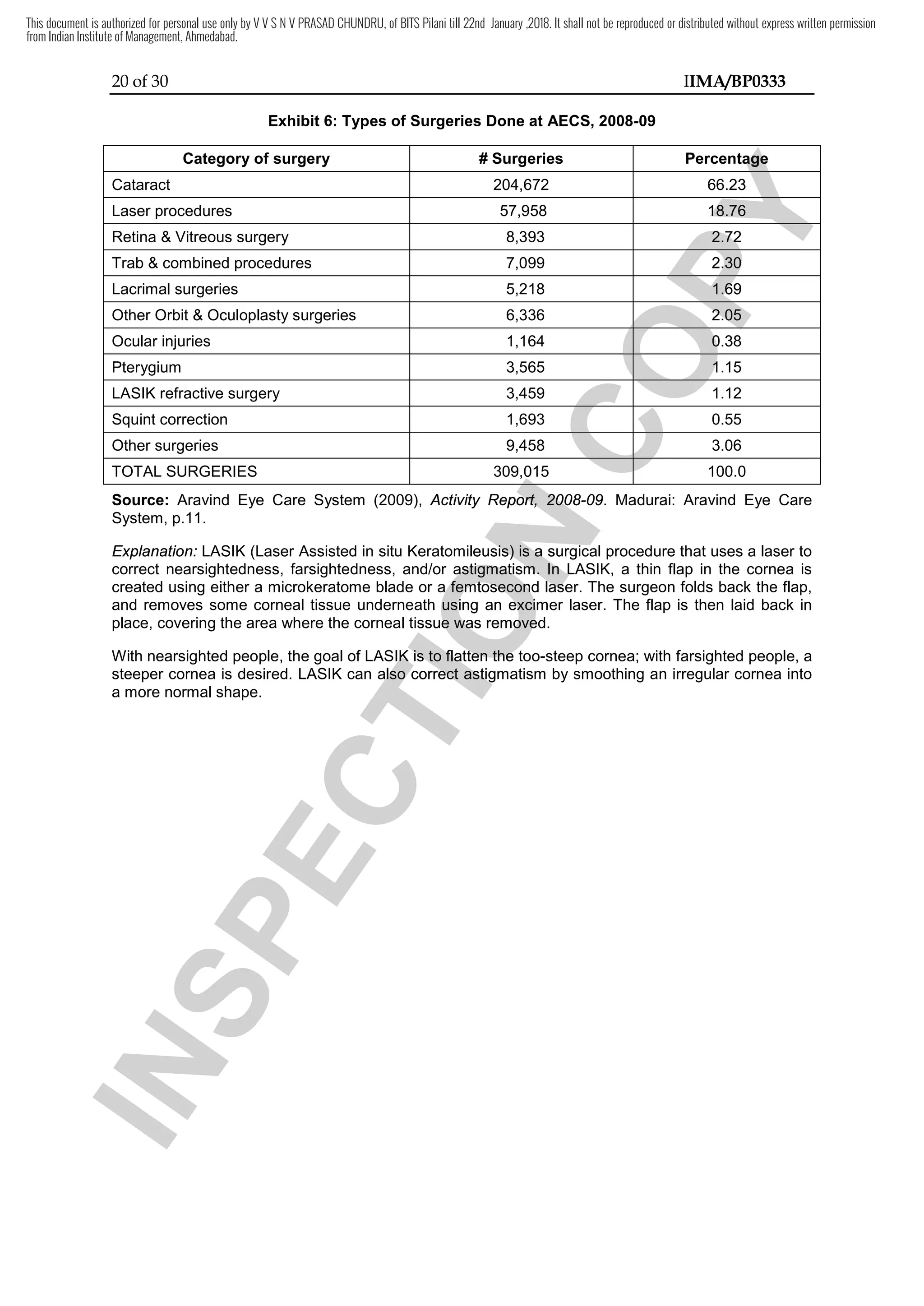
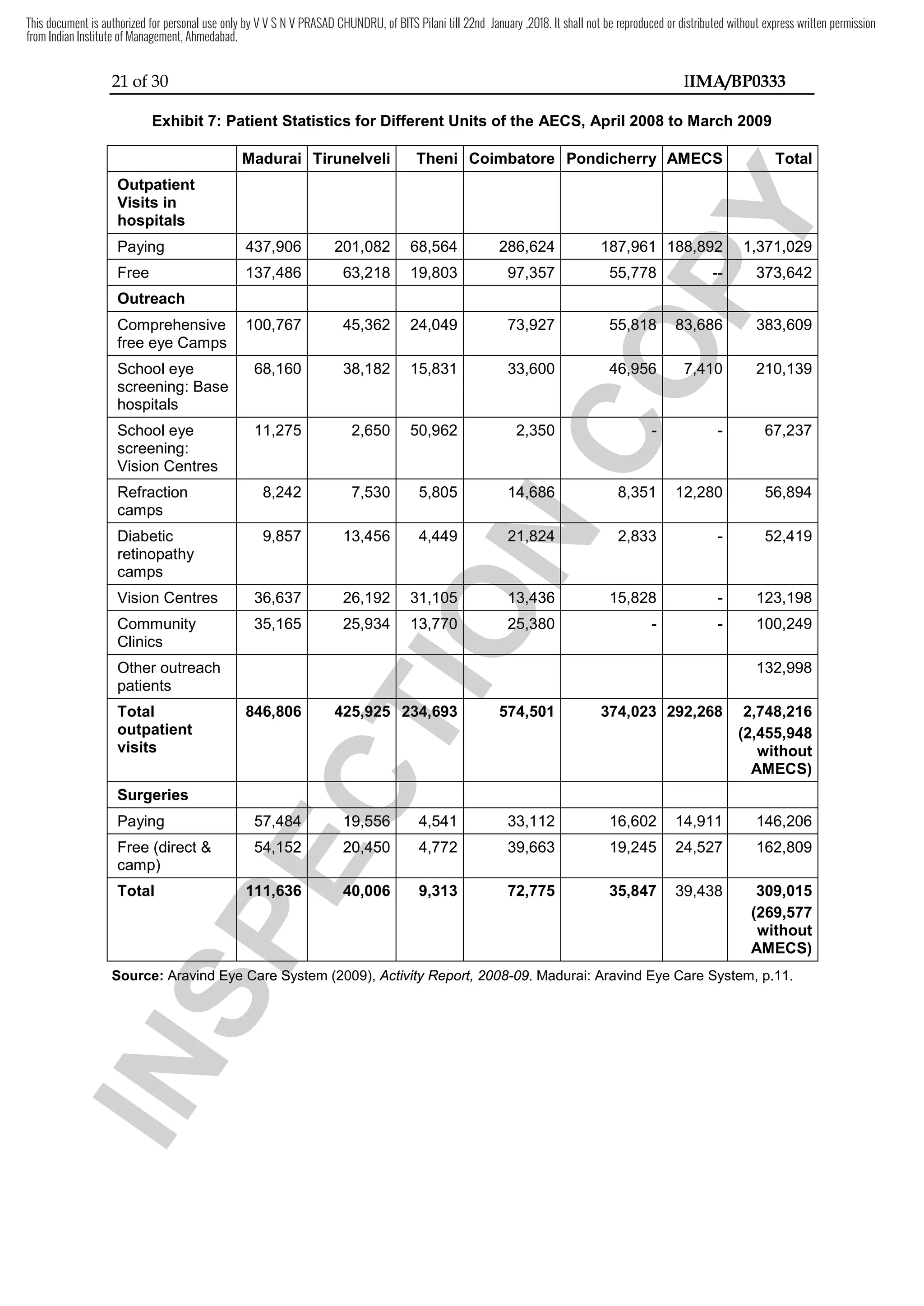
1) In 2008-2009, Aravind performed the highest number of surgeries in its history, including 162,809 free surgeries.
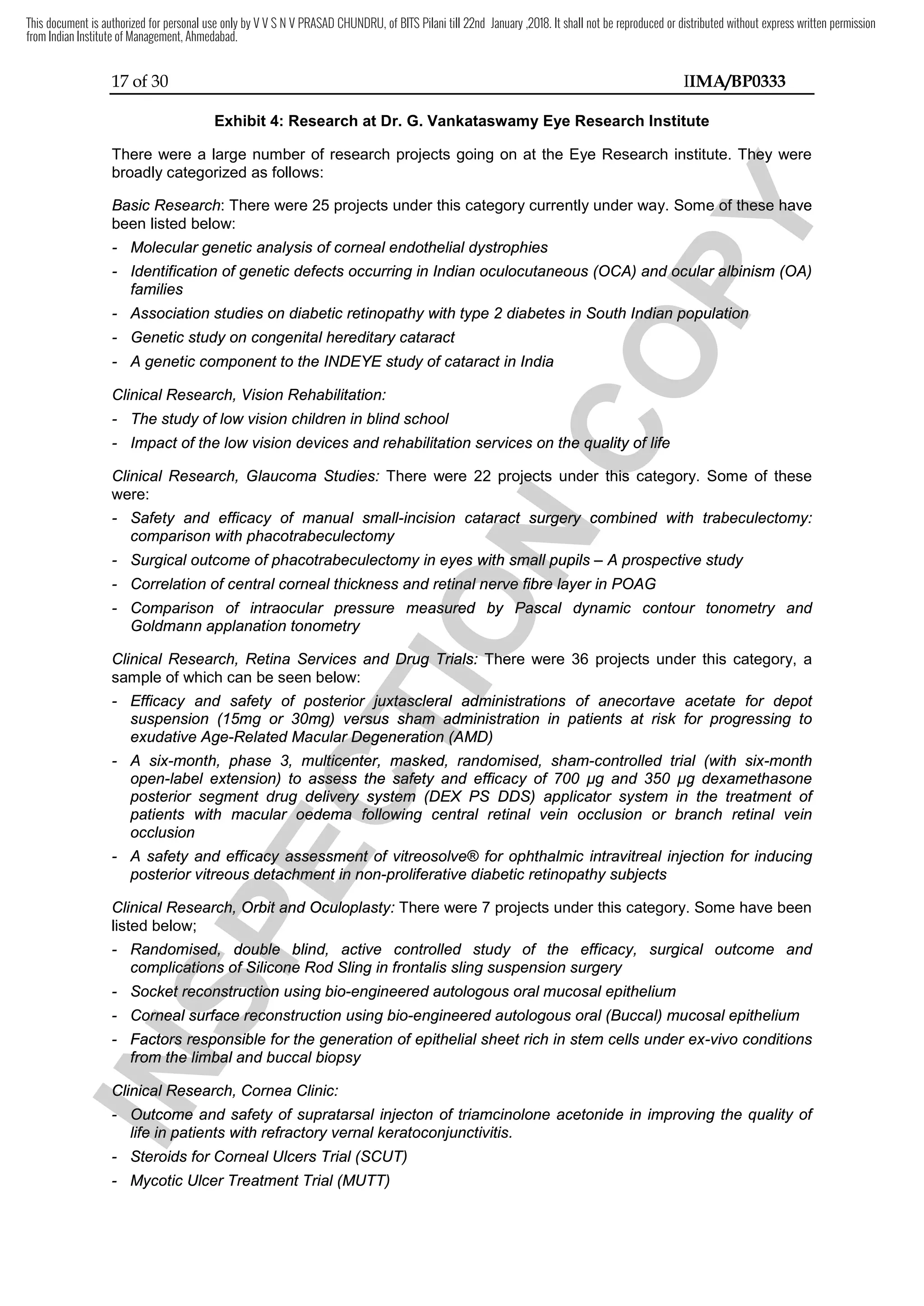
2) Since the author's previous visit in 2003, Aravind had expanded its facilities, set up new vision centers and clinics, and started a managed eye care initiative.
3) The document provides historical context on Aravind's founding in 1976 and growth under the leadership of its founder Dr. Venkataswamy, while noting the new challenges faced by its current CEO Dr. Namperumalsamy in maintaining high quality care.