Download to read offline


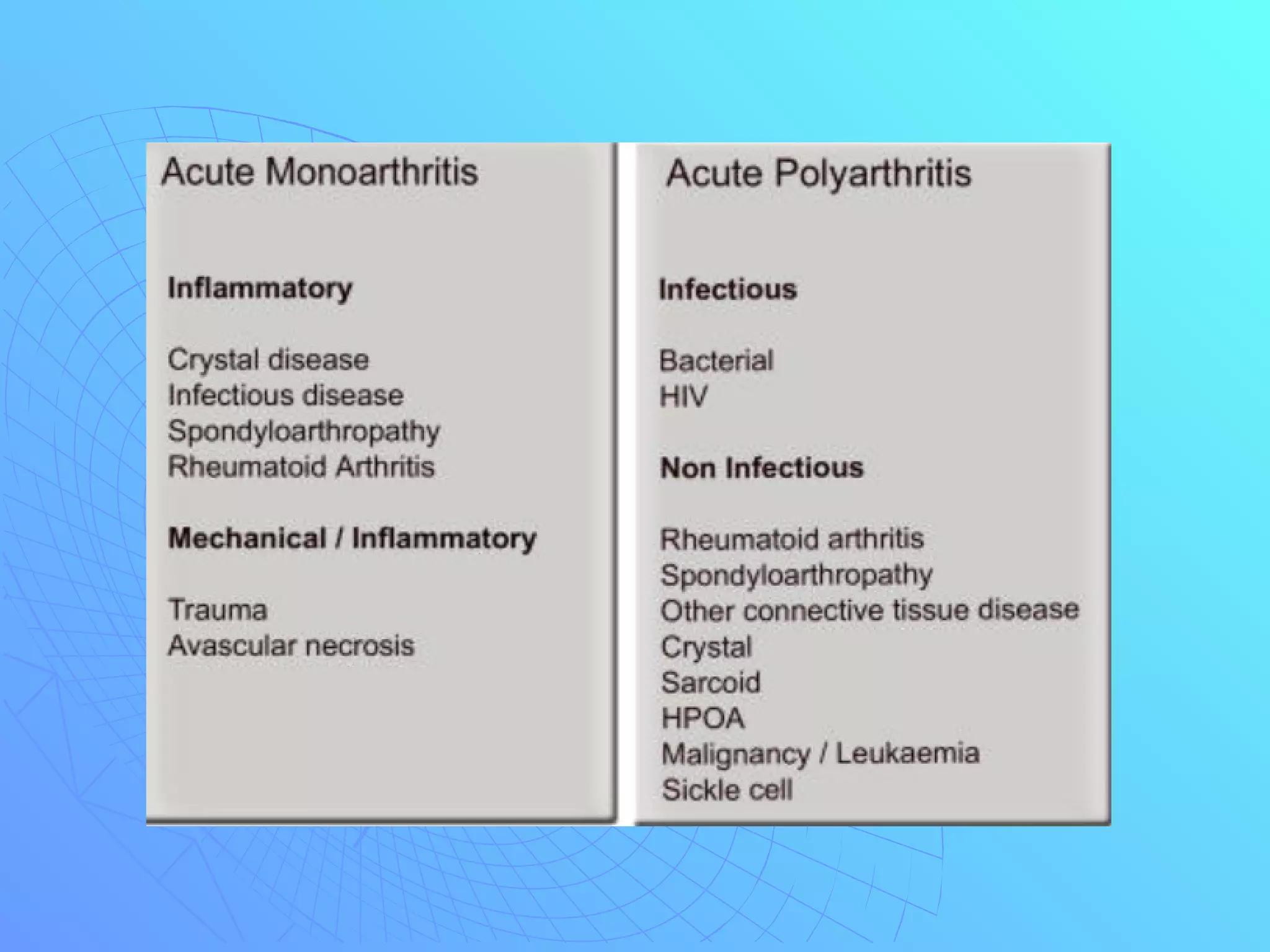











































This document discusses the approach to evaluating a rheumatologic patient, including common complaints, history taking, physical examination, and laboratory studies. It emphasizes obtaining a thorough history focused on joint issues, physical characteristics, and other illnesses. The physical exam should inspect all joints and systems potentially involved. Rheumatologic conditions are often diagnosed clinically, but laboratory tests like CBC, ESR, CRP, RF, ANA, and synovial fluid analysis can help identify conditions like rheumatoid arthritis. Proper evaluation relies on a detailed history, comprehensive physical exam, and selective use of lab tests.




























































