Antimicrobial Stewardship (Section2)
Empiric vs. targeted therapy.
How to choose the right antimicrobial agent (AMA).
De-escalation Definition.
De-escalation strategies.
3.
How are antimicrobialsused?
Antimicrobials could be used as empirical therapy or pathogen-directed therapy or
prophylaxis.
Empirical therapy : is treatment for a possible or likely infection before laboratory
results become available, or when they are impossible to obtain. Empirical choices
may have to be made on the basis of microscopy, without the benefit of culture
and sensitivity data. This type of use is most common in low resource settings and
in community or outpatient care. However, it is strongly recommended that the
use of antibiotics is reviewed if and when laboratory data are available.
4.
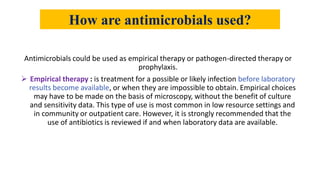
Pathogen-directed therapy:is antibiotic treatment guided by the results of
microbiological investigations, with choices determined by specific
sensitivity/resistance data.
Prophylaxis : is use of antibiotics to prevent infection. Generally used just prior to
surgery or other invasive procedures, it must target the microorganisms most likely
to cause infections following the procedure (e.g., colo-rectal surgery, prevention of
sub acute bacterial endocarditis, use in prolonged ruptured membranes prior to
delivery). It can also be applied to prevent infections in immunocompromised
patients (e.g., AIDS, cancer patients, transplants) and contacts of known infected
cases (e.g., meningococcal meningit is, TB). Prophylaxis must be used for the
shortest possible time and given when antibiotics are likely to be most effective.
5.
Choice of AnAntimicrobial
Before prescribing an AMA….
Assess patient condition
Is it an infection that can be treated? Is it bacterial?
Can it resolve on its own or with local measures only?
Then
Choose an appropriate AMA from a large number available depend on
some factors.
8.
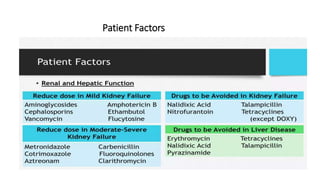
Patient Factors
Age
• Chloramphenicol͢͢͢͢͢͢͢͢͢ Gray Baby Syndrome
• Sulfonamides ͢͢͢ Kernicterus in neonates
• Tetracycline's ͢͢͢ Discoloration and deformed teeth in children
• Aminoglycosides ͢͢͢ Nerve toxicity in the elderly
Patient Factors
LocalFactors
• Presence of pus or secretions
• Presence of necrotic material or foreign body
• Hematomas
• Low pH at site of infections
• Penetration barriers at certain sites
11.
Patient Factors
DrugAllergy
History of previous intake of AMAs must be obtained before
administering any treatment to determine drug allergy
• Beta lactam drugs
• Sulfonamides } Frequently cause drug allergy
• Fluoroquinolones
12.
Patient Factors
ImpairedHost Defense
• Neutropenic Patients
• AIDS
• Impaired Cell-mediated Immunity
* Intensive cidal therapy is needed in those with impaired host defense
even then, complete eradication of organism may not occur
13.
Patient Factors
Pregnancy
• ALLAMAs SHOULD BE AVOIDED IN PREGNANCY DUE TO RISK TO THE FETUS
• Penicillins, many cephalosporins and erythromycin are said to be safe
Genetic Factors
• Primaquine
• Nitrofurantoin
• Sulfonamides } RISK OF CAUSING HAEMOLYSIS IN G-6-PD DEFIENCY
• Chloramphenicol
• Fluoroquinolones
Organism-Related Factors
AGood Guess can be Made from Clinical Features
• Tonsillitis
• Otitis Media
• Vaginitis
• Urethritis
* Gram stain smear of infected material suffices to make a choice
A Choice to be Based on Bacteriological Examination
• Meningitis
• Osteomyelitis
• UTI
• Wound infection
* But sensitivity testing may not always be possible
16.
Organism-Related Factors
a) Bacteriologicalservices not available
• Empirical therapy to be started with broad spectrum antibiotics
• Therapy is modified on the basis of clinical response
b) Bacteriological services available but treatment cannot be delayed
• Empirical therapy to be started
• AMA should be changed later in the light of bacteriological findings
c) Bacteriological services available and treatment can be delayed
Chronic UT
17.
Minimum InhibitoryConcentration (MIC)
• The lowest concentration of an antibiotic which prevents visible growth
of a
• bacterium after 24 hours incubation in a microwell culture plate using
serial dilutions of the antibiotic
Minimum Bactericidal Concentration (MBC)
• The concentration of an antibiotic which kills 99.9% of the bacteria
determined by subculturing from tubes with no visible growth.
* A small difference between MIC and MBC indicates that an antibiotic
is cidal !
* MBC is not used to guide selection of therapy
18.
Post Antibiotic Effect(PAE)
• The lag period in growth resumption after an exposed organism is
placed in an antibiotic-free medium… time required to regain
logarithmic growth
• Lag period depends on the antibiotic and on the type of organism
• Drugs with a long PAE has been noted with fluoroquinolones,
aminoglycosides and rifampicin
19.
Drug Factors
Spectrumof Activity
• Definitive Therapy → Narrow spectrum drugs concerned with the
causative organism
• Empirical Therapy→ broad spectrum drugs used to cover all likely
pathogens
20.
Drug Factors
Typeof Activity
BACTERIOSTATIC OR BACTERICIDAL
• Most infections resolve faster with cidal rather than static
• Cidal drugs usually have a prolonged post-antibiotic effect preferred in
impaired host defence and life threatening infections
• With static drugs, bacteria may quickly start multiplying when drug level
falls below MIC→ relapse of infection
21.
Drug Factors
Relative Toxicity
•A LESS TOXIC ANTIBIOTIC IS ALWAYS PREFERRED … OBVIOUSLY!!!
• Beta lactam drugs over aminoglycosides
• Erythromycin over clindamycin
22.
Drug Factors
Routeof Administration
• Many AMAs can be given both orally or parenterally
• Few like aminoglycosides, Penicillin G, Vancomycin are given by
injection ONLY
• Oral antibiotics are preferred for less severe infections
• Parenteral antibiotics are preferred in more severe infections
23.
Drug Factors
Evidenceof Clinical Efficacy
• The value of various AMAs in therapy is based on comparative clinical
trials
• Optimum dosages and duration of treatment are determined based
on studies
• Reliable clinical trial data is the best guide for choice of an antibiotic!
Cost
• LESS EXPENSIVE DRUGS ARE PREFERRED …. AGAIN… OBVIOUSLY!!!
25.
Combined Use ofAntimicrobials
One is good, two should be better three should cure
• Frequently used
• Should only be administered when there is a specific purpose
• Objectives to use combinations:
1. To achieve synergism → Cotrimoxazole
2. To reduce severity or incidence of Side Effects → Streptomycin + Pen G in SABE
3. To prevent emergence of resistance → TB, Leprosy, HIV, H. pylori, Malaria
4. To broaden spectrum →treatment of mixed infections, severe infections, topical
26.
What is de-escalation?
•De-escalation is when we switch to a narrower-spectrum antibiotic to
target the causative pathogen(s) identified on culture.
Key Points: Switching to narrower spectrum antibiotics when
clinically indicated can prevent adverse reactions and reduce
antibiotic resistance.
27.
What is myrole in de-escalation?
• Every day, review all patients on broad-spectrum antibiotics in your
patient care area and identify those with positive cultures. Review
these patients using the 6-step process to determine whether a
narrower antibiotic would optimize therapy. If you feel a change in
therapy is needed, work with the prescribing provider and
recommend an alternate therapy. This process is designed for
patients with positive cultures only!
key Point: The goal of de-escalation is to determine whether a
narrower antibiotic would be more appropriate for each patient.
28.
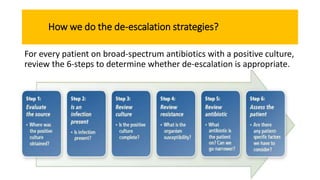
How we dothe de-escalation strategies?
For every patient on broad-spectrum antibiotics with a positive culture,
review the 6-steps to determine whether de-escalation is appropriate.
29.
Step 1 :Evaluate the source
• Where was the positive culture obtained? Positive cultures in sites
considered sterile need to be taken very seriously. For positive
cultures taken from non-sterile sites, use your clinical judgment to
determine whether the culture represents an infection or colonization
(step 2). Review the type, source, and status of the culture.
Key Point:
• Sterile sites: blood, CSF, bone, pleural fluid, synovial fluid, and
other deep surgical sites.
• Non-sterile sites: urine, skin, wounds, sputum, etc.
30.
Step 2: Isan infection present
• Is an infection present? The positive culture may represent any one of the
following:
• Infection: The presence of pathogenic microorganisms that invade a body
part or tissue to cause symptomatic disease.
• Colonizer: The presence of microorganisms in a non-sterile site that is not
causing infection. These are typically commensal organisms belonging to
normal flora and harmless to healthy people; sometimes they perform a vital
function (e.g., gut bacteria aid in digestion).
• Contaminant: The unintentional or accidental introduction of
microorganisms into a culture, either when the culture was obtained or in
the microbiology laboratory.
Key Point for step 2 : If the culture shows a colonizer or a contaminant is
present, suggest that the provider stop or adjust the patient’s
antimicrobials
31.
Step 3: Reviewculture
• Is the positive culture complete? Ask yourself:
• Is the culture finalized? Are other cultures pending?
• Are there other organisms on the Gram stain that didn’t grow?
• Does the infectious syndrome warrant broader therapy than the culture would
suggest? Do you need to cover more than just the positive culture? For example,
if the patient has an intra-abdominal abscess and the blood culture grows E coli,
anaerobic coverage is still required even though the culture didn’t grow
anaerobes.
• Does the patient have a comorbid infectious syndrome that warrants broader
therapy?
Key Point: If all cultures aren’t final, consider waiting on giving the provider a
recommendation for de-escalation
32.
Step 4: Reviewresistance
• What is the organism’s susceptibility profile?
• Always review the susceptibility profile to determine what antibiotics
will be active. If there is an antibiotic you would like to use that isn’t
listed on the culture, call your microbiology laboratory for more
information.
Key Point: Talk to the microbiological laboratory for more
information.
33.
Step 5: Reviewantibiotic
• What antibiotic is the patient on? Can we go any narrower? After you’ve assessed
the culture and susceptibility profile, ask yourself:
• Is there a narrower antibiotic that will better meet the needs of the patient?
• What exactly should I recommend?
Key Point: When you are ready to make a de-escalation recommendation, be
specific (e.g., include patient specific dosing).
34.
Step 6: Assessthe patient
• Are there any patient-specific factors we have to consider? Consider
the following patient-specific factors before making your
recommendation:
• Convenience (e.g., dosing interval, IV and PO, side effects, etc.)
• Allergies
• Drug-drug interaction
• IV or oral conversion
Key Point: Individualize your recommendation to the patient.
35.
Questions:
1-Empiric antimicrobial therapy:
a.Is given routinely before appropriate microbiological specimens have been
taken
b. Consists usually of a single antimicrobial drug that targets the most likely
pathogen
c. Usually includes several anti-infective drugs that cover the most likely
causative pathogens
d. Is continued even after the definitive cause of the infection is identified.
2-Targeted antimicrobial therapy:
a. Aims to match the antimicrobial given to the specific pathogen-causing
infection
b. Uses broad-spectrum antibiotics to cover all potential pathogens
c. Does not require the collection of appropriate microbiological specimens
d. Usually requires several different antimicrobials to be prescribed
36.
3-De-escalation of antimicrobialtherapy:
a. Means changing the patient’s prescription from a narrow to a broad-spectrum
antimicrobial
b. Is potentially harmful, even if the pathogen is sensitive to a narrow-spectrum
antimicrobial
c. Ensures effective therapy but reduces harmful effects of broad-spectrum
antimicrobials
d. Means that therapy should be stopped or discontinued.
• Mark (True/ False)
1-Minimum inhibitory concentration(MIC) The concentration of an
antibiotic which kills 99.9% of the bacteria determined by sub
culturing from tubes with no visible growth (T/F)
2-If all cultures aren’t final, Not consider waiting on giving the provider
a recommendation for de-escalation (T/F)









































![Hacking-Uncovered-How-People-Get-Hacked-and-How-to-Stay-Safe[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hacking-uncovered-how-people-get-hacked-and-how-to-stay-safe1-260130170011-4883a9c7-thumbnail.jpg?width=640&height=640&fit=bounds)







