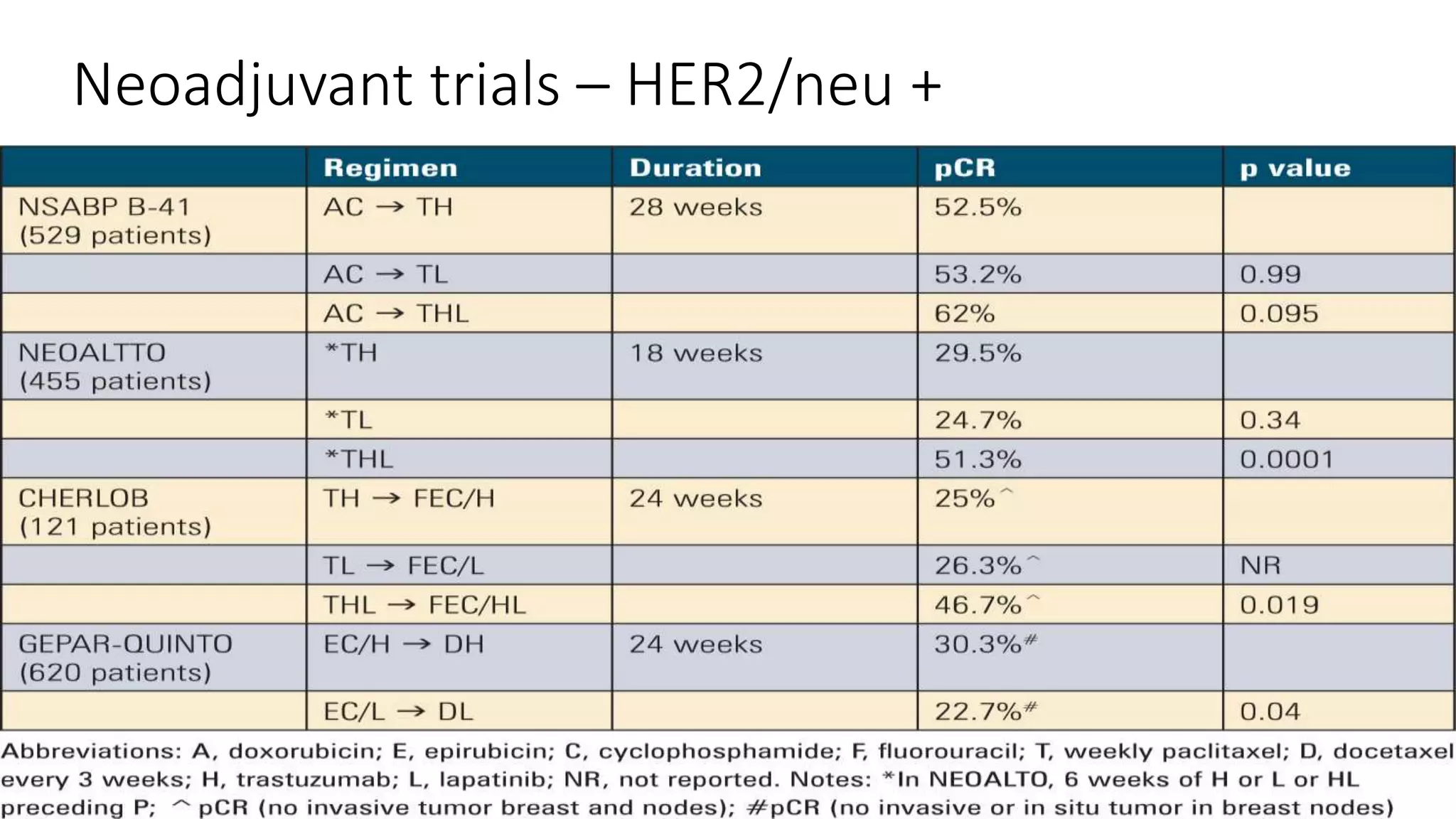
The document discusses neoadjuvant and adjuvant therapies for HER2-positive breast cancer. It summarizes several clinical trials evaluating combinations of trastuzumab, pertuzumab, docetaxel, and other chemotherapies in the neoadjuvant and adjuvant settings. Combinations including dual HER2 blockade with trastuzumab and pertuzumab were found to significantly improve pathological complete response rates compared to other regimens. Ongoing studies continue exploring new targeted agents and combinations to further improve outcomes for patients with high-risk HER2-positive breast cancer.