ANATOMY OF NOSE- FESS
PRESENTOR- Dr SMITHA D
MODERATOR-Dr ANIL REDDY
2.
CONTENTS
• Embryology
• Osteology
•Lateral wall of nose proper
Gross Anatomy
Blood supply
Nerve supply
Lymphatic Drainage
Transport of Secretion
• Surgical Anatomy
• Endoscopic Anatomy
3.
EMBRYOLOGY
• Facial developmenttakes place between 4 – 8 weeks of intra
uterine life
• Face develops from 5 facial swellings that surround the
Primitive mouth by the end of 4th
week
Central unpaired frontonasal process
Pair of maxillary process
Pair of mandibular process
4.
At 5th
week thickeningappear in fronto nasal process called
nasal placodes
At 6th
week nasal placode invaginates to form nasal pits
38- 40 days - Maxilloturbinal appear as swelling- Inferior
Turbinate
40- 43 days - Ethmoturbinals appear at junction of nasal
septum and nasal roof
Space btw MT & ET – Middle Meatus
6th
and 7th
week maxillary process increase in size to grow
medially
5.
Maxillary process fuseswith the lateral nasal process
The junction is marked by a groove called nasolacrimal/
naso-optic groove
By 7th
week groove invaginates into mesenchyme to form
nasolacrimal duct
6.
9th
& 10th
wk -6major furrows develops
60 Days – Nasoturbinal appear (ant to ET)- Agger Nasi
65 Days – 1st
Ethmoturbinal - uncinate process is identifiable
1st
&2nd
ET – Ethmoidal infundibulum
2nd
ET- Middle turbinate
3rd
ET – Superior turbinate
4th
& 5th
ET – Supreme turbinate
1st
Furrow (ascending)- Frontal recess
descending – Middle meatus & hiatus semilunaris
2nd
Furrow – Superior meatus
3rd
Furrow- Uppermost meatus
7.
• 65/70 days– pouch into floor of infundibulam- maxillar sinus
• 105 days – frontal recess cells develop medial to uncinate
• Fetal frontal recess cells- lateral to ant attachment of middle
turbinate, medial to uncinate
• frontal sinus opens medial to uncinate into middle meatus
• Ant aspect of infundibulam- Ant infundibular cells
Near roof of ethmoid
Most ant- may expand – frontal sinus
Frontal sinus opens into infundibulam (lat to UP)
Frontal bulla – ant ethmoidal cell, when frontal recess cells
form frontal sinus
Pneumatise agger nasi, uncinate, lacrimal bone
8.
• Suprabulbar cells– sup to bulla, infundibulam expands into 3 – 4
furrows.
Ethmoid bulla is pneumatised
supraorbital cells
One of the source for frontal sinus
source of concha bullosa
• lateral sinus forms following the development of ethmoidal bulla
• Infrabulbar cells- Infundibulaam expands inf to bulla
Inconstant space
Pnematise the bulla
invade ethmomaxillary plate -
Ethmomaxillary cells- Haller cells (post medial sup aspect of
maxilla)
9.
• 110 days– Ant end of sup meatus divide to Inf & Sup arm
Inf arm: two tracts of cell
1.Expand ant into lamella of middle turbinate as M/C
origin of concha bullosa
2.Expand laterally, space btw lat ethmoidal wall &
maxilla & ascending / orbital process of palate as M/C origin of
Haller cell
• Post ethmoidal cells
Origin from sup & supreme meatus
Supraorbital cells
Ant to frontal bone & post upto sphenoid
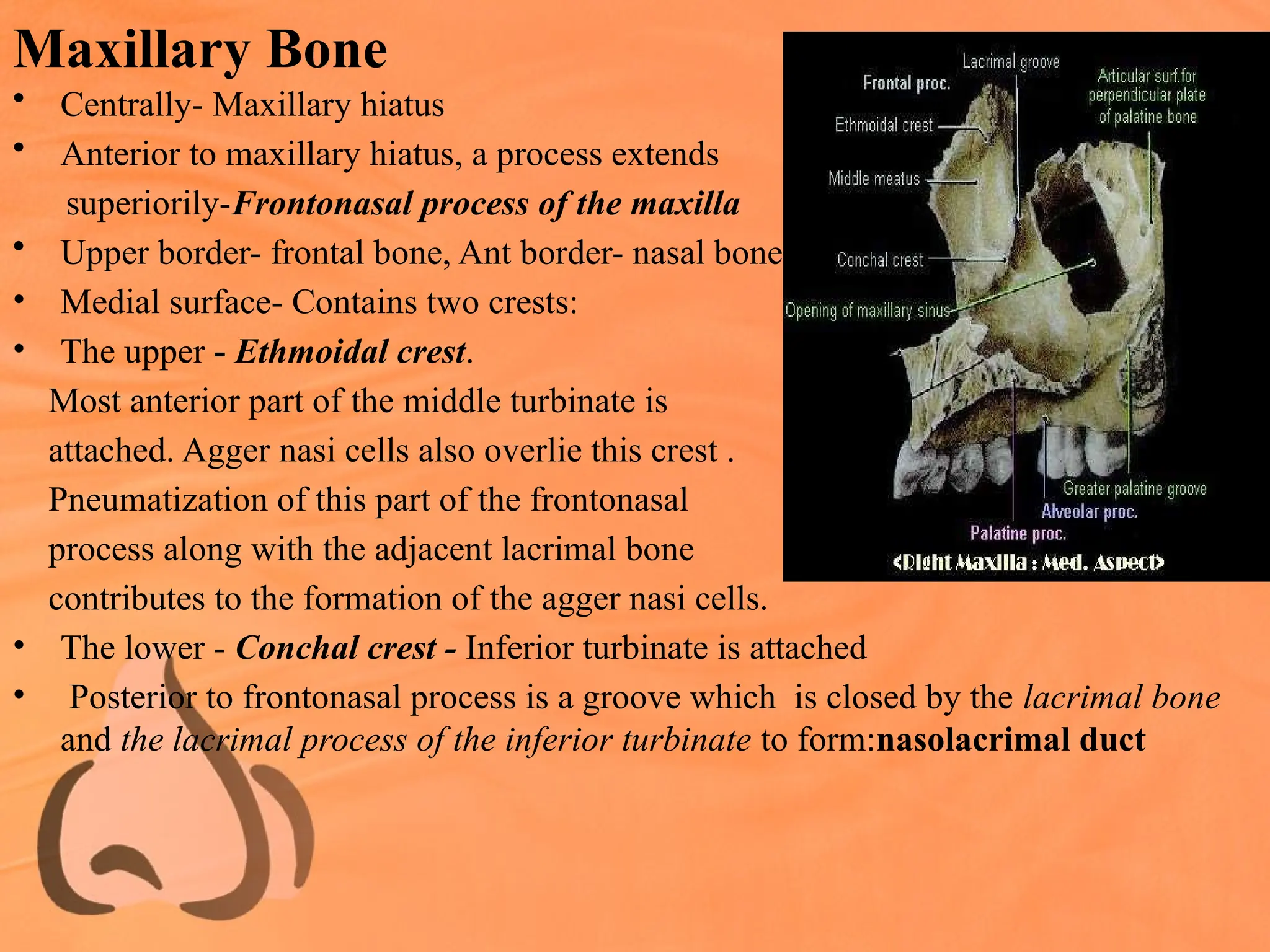
Maxillary Bone
• Centrally-Maxillary hiatus
• Anterior to maxillary hiatus, a process extends
superiorily-Frontonasal process of the maxilla
• Upper border- frontal bone, Ant border- nasal bone
• Medial surface- Contains two crests:
• The upper - Ethmoidal crest.
Most anterior part of the middle turbinate is
attached. Agger nasi cells also overlie this crest .
Pneumatization of this part of the frontonasal
process along with the adjacent lacrimal bone
contributes to the formation of the agger nasi cells.
• The lower - Conchal crest - Inferior turbinate is attached
• Posterior to frontonasal process is a groove which is closed by the lacrimal bone
and the lacrimal process of the inferior turbinate to form:nasolacrimal duct
12.
• Roughened areaposterior to the hiatus
at the junction of the medial and the
posterior wall of the maxilla:
maxillary tuberosity.
This area has an oblique groove
which when completed by the
perpendicular plate of the palatine
bone forms the canal for the greater
palatine vessels and nerve.
• roof of maxillary sinus- orbital surface
of the maxilla -marked by the
infraorbital canal - dehiscent to
expose its contents, namely, the
infraorbital vessels and nerve.
13.
Frontal Bone
• Center- Hiatus- cribriform plate
of ethmoid
• anterior and posterior ethmoidal
air cells on either side.
• Roof of air cells: skull base or
Ethmoidal fovea-higher level
• Laterally, lamina papyracea of ethmoid bone
• Junction of the suture lines between the lamina and the frontal bone, is the anterior
and posterior ethmoidal foramina transmitting their respective arteries.
• Lateral to the lamina papyracea- Orbit.
• Anteriorly and in the midline - Nasal spine. This spine articulates with the nasal
bones, which help in forming the anterior most portion of the lateral nasal wall
14.
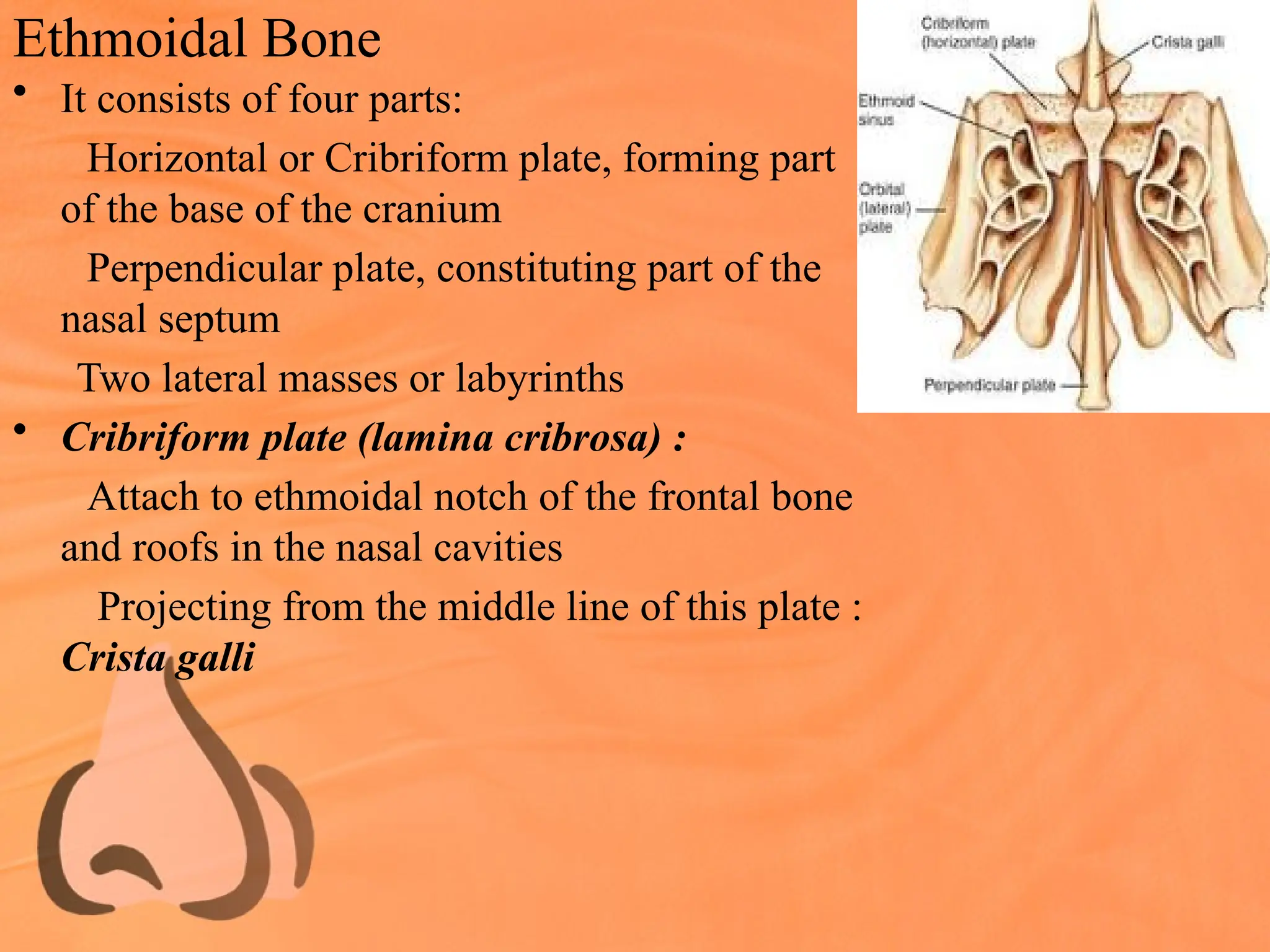
Ethmoidal Bone
• Itconsists of four parts:
Horizontal or Cribriform plate, forming part
of the base of the cranium
Perpendicular plate, constituting part of the
nasal septum
Two lateral masses or labyrinths
• Cribriform plate (lamina cribrosa) :
Attach to ethmoidal notch of the frontal bone
and roofs in the nasal cavities
Projecting from the middle line of this plate :
Crista galli
15.
• Cribriform plateshows a horizontal medial
lamella & oblique / vertical lateral lamella.
• Lateral lamella articulates with the frontal bone
forms - Ethmoid fovea
[medially by the lateral lamella of the
cribriform plate & laterally by the frontal bone]
• Frontal bone - ethmoid fovea - 0.5 mm thick
lateral lamella of the cribriform plate -0 .2 mm.
• The region where the anterior ethmoidal artery
pierces the dura medially is the thinnest area in
the base skull -0.05 mm thick.
16.
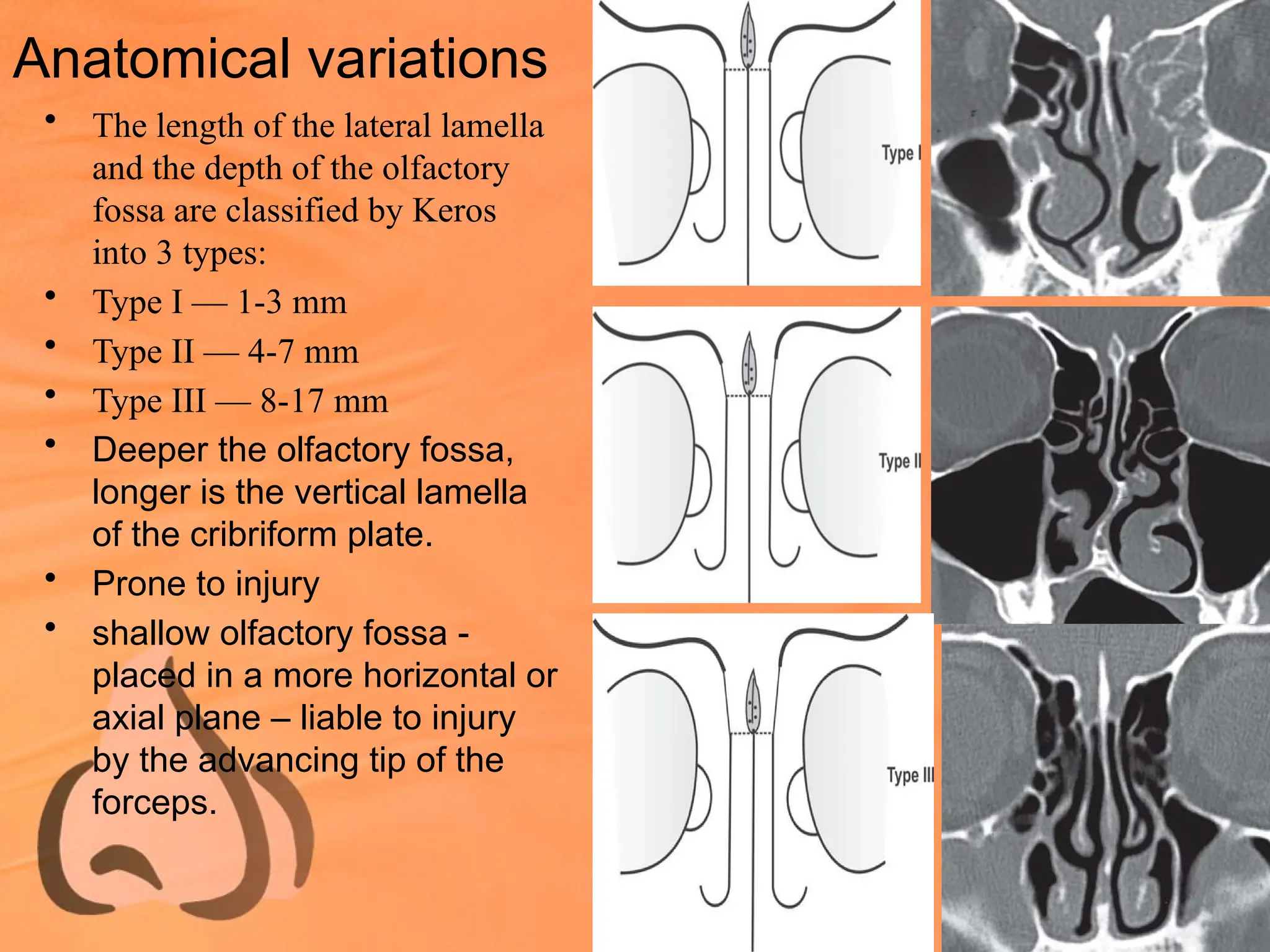
Anatomical variations
• Thelength of the lateral lamella
and the depth of the olfactory
fossa are classified by Keros
into 3 types:
• Type I — 1-3 mm
• Type II — 4-7 mm
• Type III — 8-17 mm
• Deeper the olfactory fossa,
longer is the vertical lamella
of the cribriform plate.
• Prone to injury
• shallow olfactory fossa -
placed in a more horizontal or
axial plane – liable to injury
by the advancing tip of the
forceps.
17.
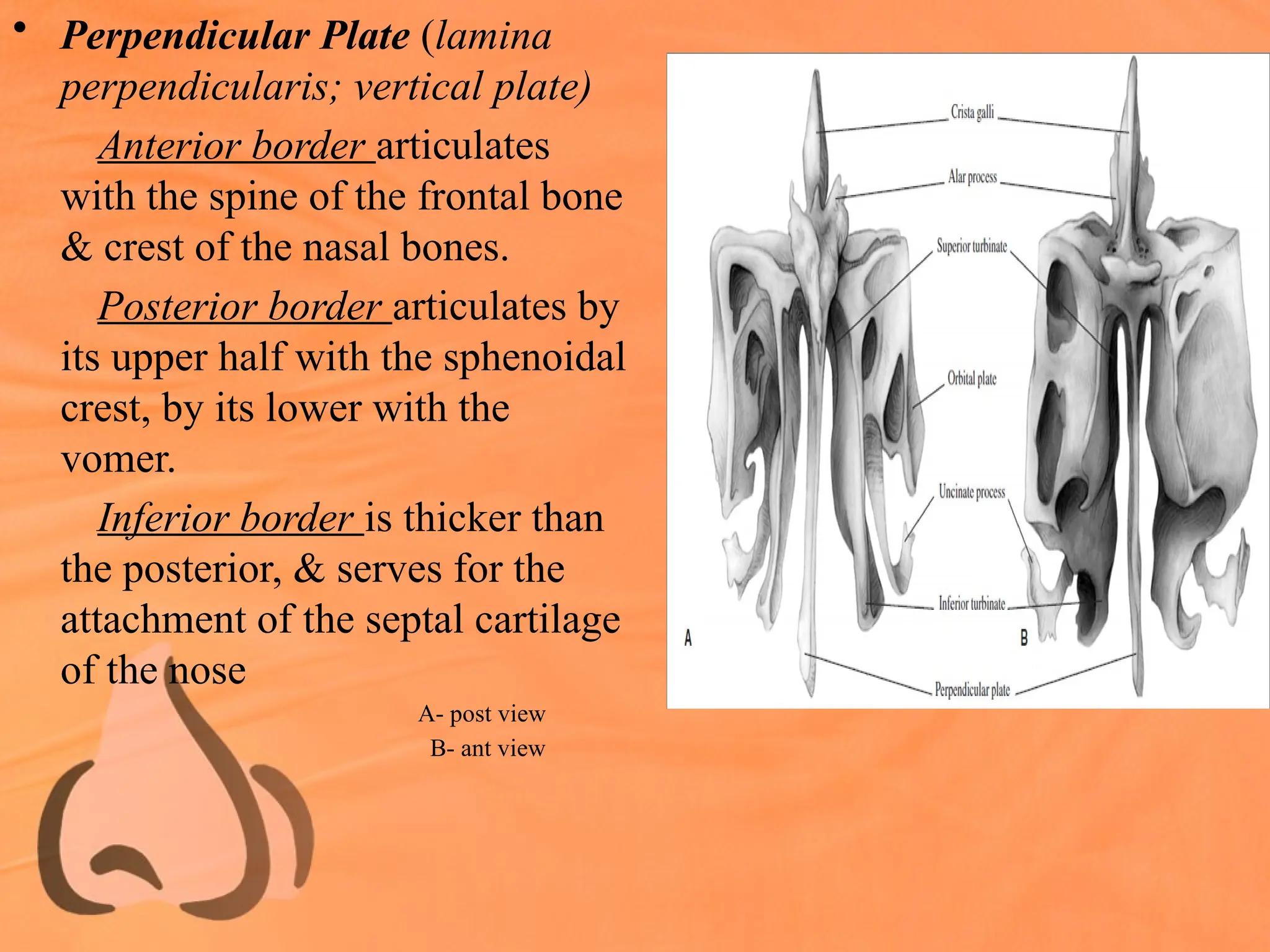
• Perpendicular Plate(lamina
perpendicularis; vertical plate)
Anterior border articulates
with the spine of the frontal bone
& crest of the nasal bones.
Posterior border articulates by
its upper half with the sphenoidal
crest, by its lower with the
vomer.
Inferior border is thicker than
the posterior, & serves for the
attachment of the septal cartilage
of the nose
A- post view
B- ant view
18.
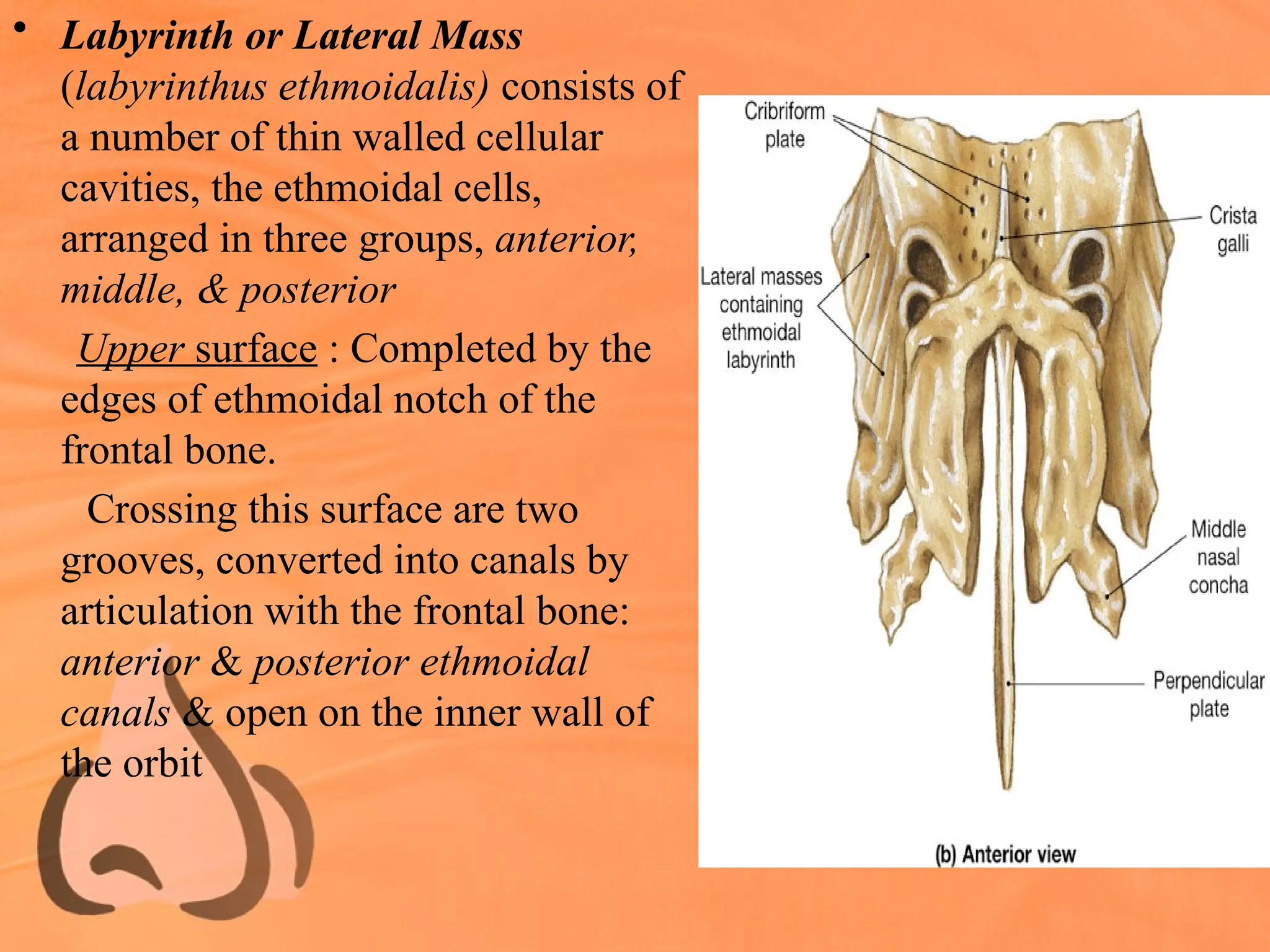
• Labyrinth orLateral Mass
(labyrinthus ethmoidalis) consists of
a number of thin walled cellular
cavities, the ethmoidal cells,
arranged in three groups, anterior,
middle, & posterior
Upper surface : Completed by the
edges of ethmoidal notch of the
frontal bone.
Crossing this surface are two
grooves, converted into canals by
articulation with the frontal bone:
anterior & posterior ethmoidal
canals & open on the inner wall of
the orbit
19.
Posterior surface :Presents large
irregular cellular cavities,
which are closed in by
articulation with the
sphenoidal concha and orbital
process of the palatine
Lateral surface : Formed of a
thin, smooth, oblong plate, the
lamina papyracea (os
planum), which covers middle
and posterior ethmoidal cells
C-sup view
D- inf view
20.
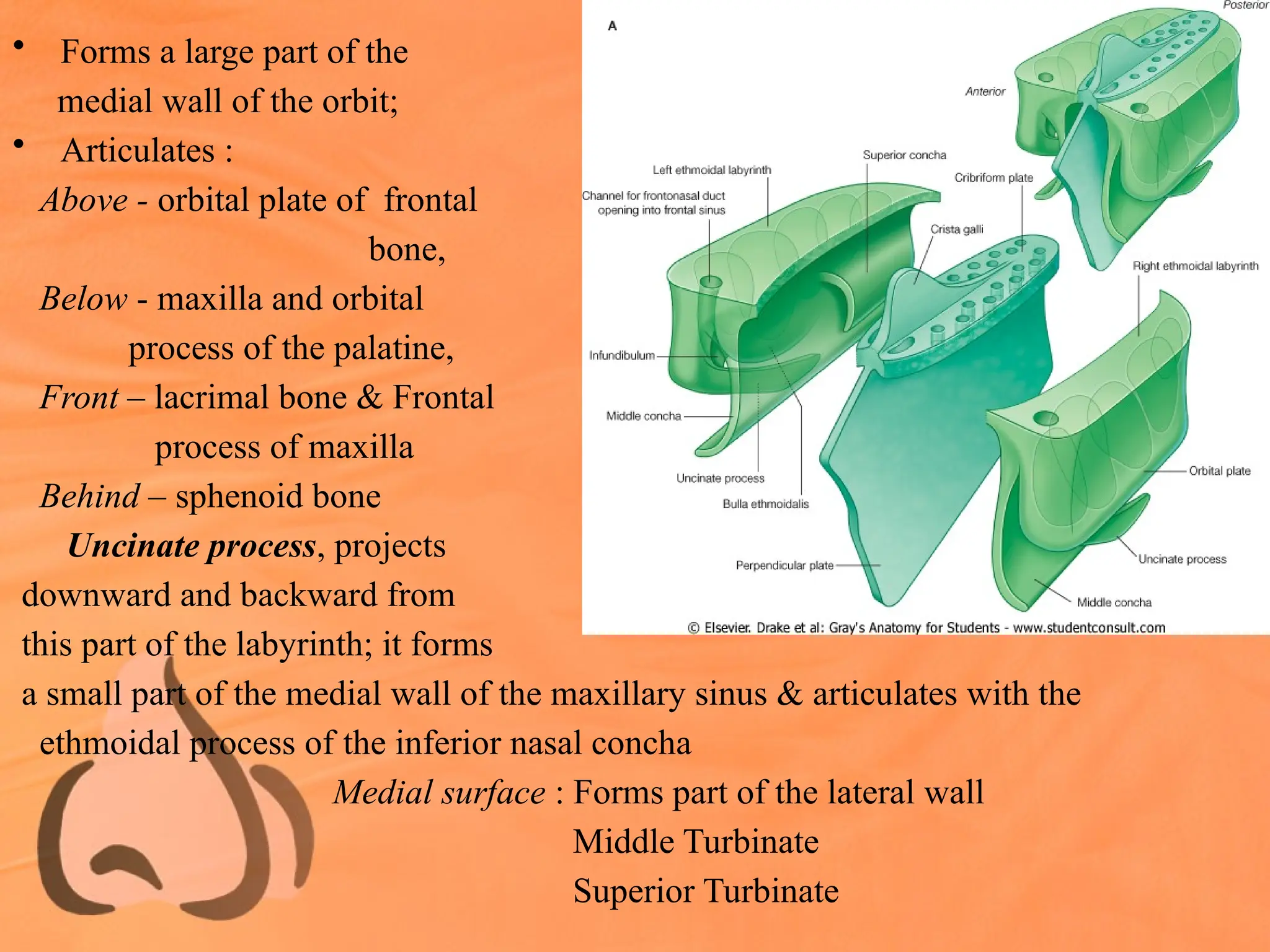
• Forms alarge part of the
medial wall of the orbit;
• Articulates :
Above - orbital plate of frontal
bone,
Below - maxilla and orbital
process of the palatine,
Front – lacrimal bone & Frontal
process of maxilla
Behind – sphenoid bone
Uncinate process, projects
downward and backward from
this part of the labyrinth; it forms
a small part of the medial wall of the maxillary sinus & articulates with the
ethmoidal process of the inferior nasal concha
Medial surface : Forms part of the lateral wall
Middle Turbinate
Superior Turbinate
21.
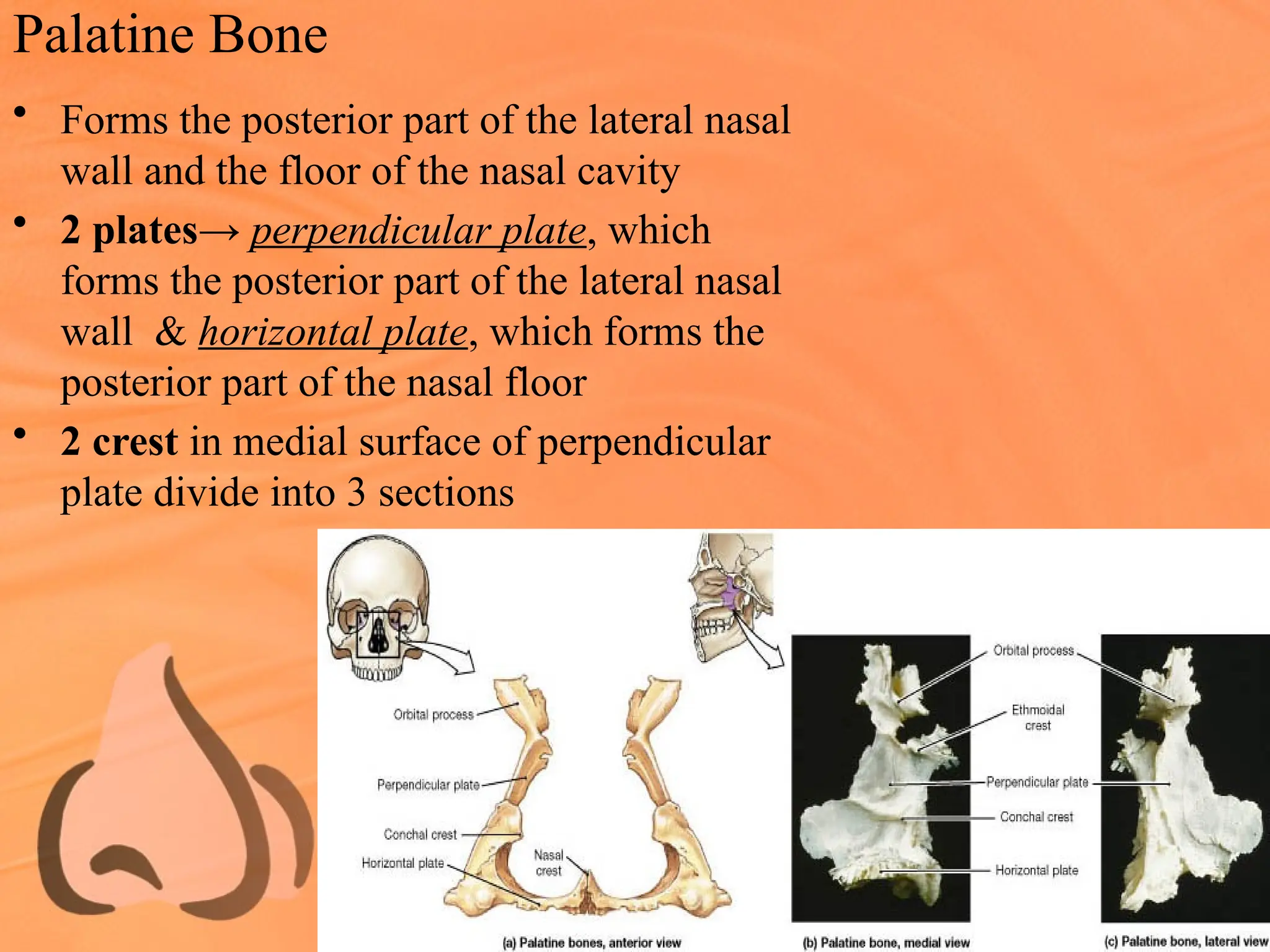
Palatine Bone
• Formsthe posterior part of the lateral nasal
wall and the floor of the nasal cavity
• 2 plates→ perpendicular plate, which
forms the posterior part of the lateral nasal
wall & horizontal plate, which forms the
posterior part of the nasal floor
• 2 crest in medial surface of perpendicular
plate divide into 3 sections
22.
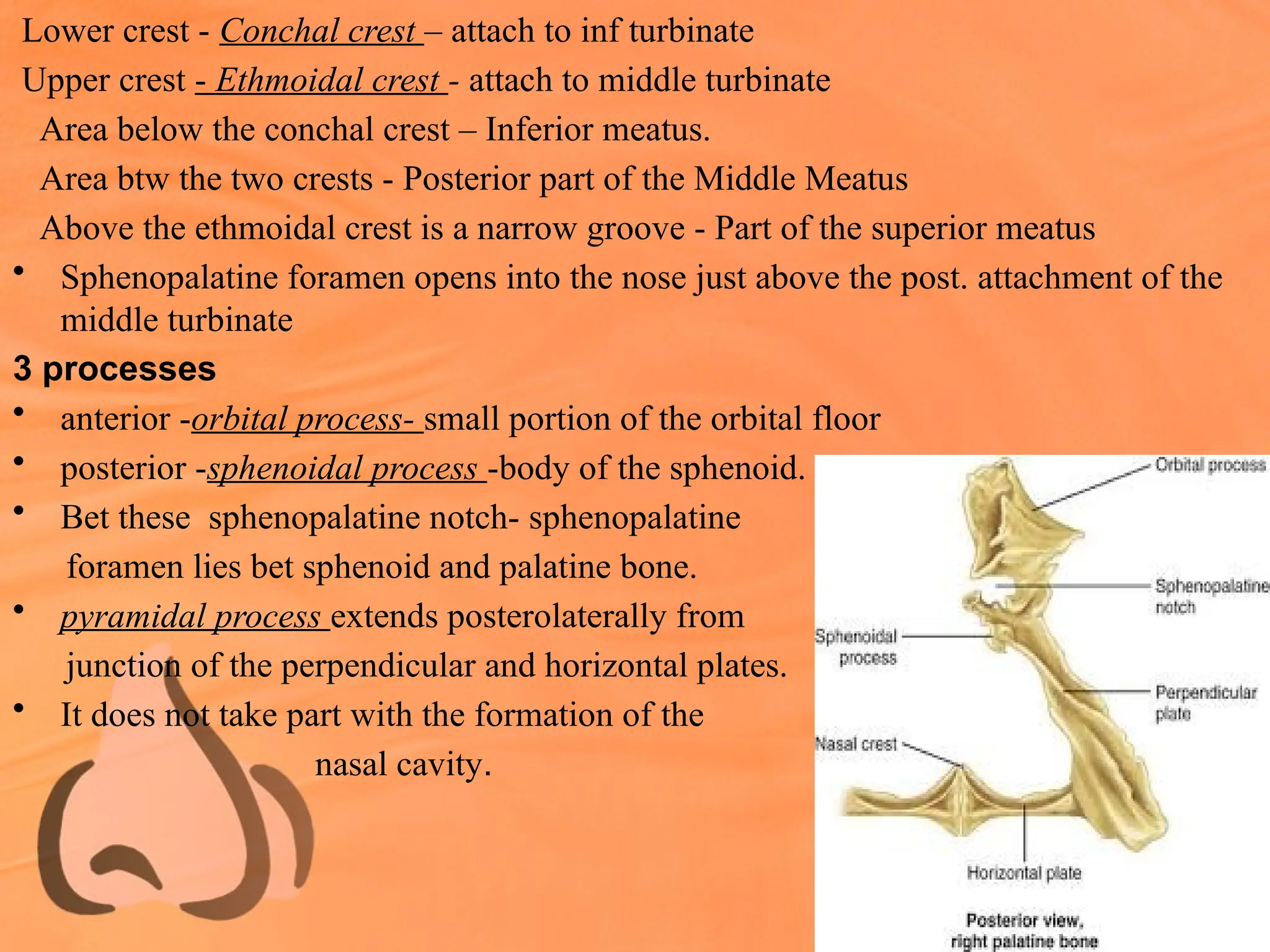
Lower crest -Conchal crest – attach to inf turbinate
Upper crest - Ethmoidal crest - attach to middle turbinate
Area below the conchal crest – Inferior meatus.
Area btw the two crests - Posterior part of the Middle Meatus
Above the ethmoidal crest is a narrow groove - Part of the superior meatus
• Sphenopalatine foramen opens into the nose just above the post. attachment of the
middle turbinate
3 processes
• anterior -orbital process- small portion of the orbital floor
• posterior -sphenoidal process -body of the sphenoid.
• Bet these sphenopalatine notch- sphenopalatine
foramen lies bet sphenoid and palatine bone.
• pyramidal process extends posterolaterally from
junction of the perpendicular and horizontal plates.
• It does not take part with the formation of the
nasal cavity.
23.
• Perpendicular plate
•Anterior border of the perpendicular plate has a prolongation - maxillary process -
articulates - maxillary process of inferior turbinate
• Posteriorly - medial pterygoid plates to form the lateral wall of the posterior
choana.
• Inferiorly - continuous with the horizontal plate.
• Superiorly- maxilla by its orbital process
and sphenoid by its sphenoidal process.
• Horizontal plate
• Anteriorly- horizontal process of the maxilla
to form the nasal floor.
• Posteriorly- free border, which is the
posterior end of the hard palate
24.
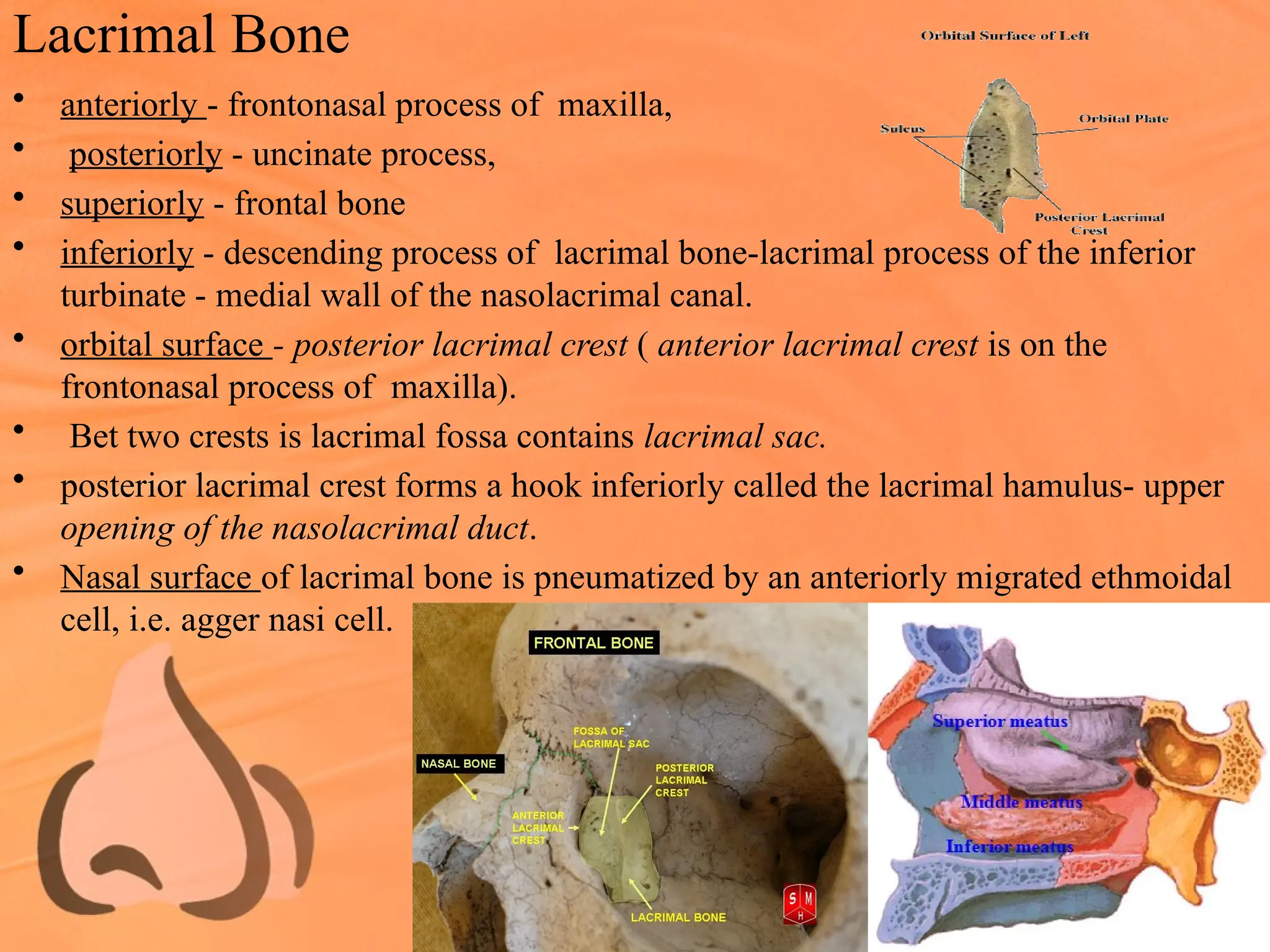
Lacrimal Bone
• anteriorly- frontonasal process of maxilla,
• posteriorly - uncinate process,
• superiorly - frontal bone
• inferiorly - descending process of lacrimal bone-lacrimal process of the inferior
turbinate - medial wall of the nasolacrimal canal.
• orbital surface - posterior lacrimal crest ( anterior lacrimal crest is on the
frontonasal process of maxilla).
• Bet two crests is lacrimal fossa contains lacrimal sac.
• posterior lacrimal crest forms a hook inferiorly called the lacrimal hamulus- upper
opening of the nasolacrimal duct.
• Nasal surface of lacrimal bone is pneumatized by an anteriorly migrated ethmoidal
cell, i.e. agger nasi cell.
Anatomical variations ofGround Lamella(GL)
GL of MT, separates ant & post ethmoid cells, is not always in a coronal plane
• May bulge into ant ethmoids & have a convexity anteriorly
• May bulge into post ethmoids with a concavity anteriorly
• May show dehiscences or be partially deficient - infection can pass from ant to post
ethmoids.
• May itself be pneumatized & split into multiple septae
• Usually attaches to lamina papyracea, may, rarely, turn inferiorly in which case it
“misses” lamina papyracea & attaches to lateral wall of maxillary sinus
• Maxillary sinus is thus divided into two parts. The post part behaves like a post
ethmoidal cell in terms of drainage and involvement by disease
27.
LATERAL WALL OFNOSE
Gross Anatomy
• Anteriorly in the area of the nostril, the lateral nasal wall is lined by skin and has
hair : vestibule.
• Behind this is a plain structureless area lined by nasal mucosa: atrium.
• Atrium shows a bulge anterior to the middle turbinate formed by the underlying
Agger nasi cell.
• Very often a ridge can be discerned extending from the agger nasi cell to an apex
on the superior border of the inferior turbinate, this ridge overlies the nasolacrimal
duct
28.
• Behind theatrium are the three scrolls
of the inferior, middle & superior
turbinates, overlying the respective
meatii.
• Occasionally, supreme turbinate.
• Above the superior turbinate is the
sphenoethmoidal recess, which gets
its name from the fact that this area
forms a niche between the posterior
ethmoid cells and the sphenoid sinus.
29.
INFERIOR MEATUS
• lateralto the inferior turbinate.
• largest meatus, extending almost the entire length of
the nasal cavity.
• highest at the junction of the anterior and middle third.
• In adults,1.6 cm along the bony lateral wall
• Nasolacrimal duct – Hasner valve
• endoscopically identified by gentle massage of the
lacrimal sac at the medial canthus
30.
INFERIOR TURBINATE
• separatescroll-like bone
• Superior margin- maxilla anteriorly & palatine
bone posteriorly
• Inferior margin- free,overhanging its meatus
31.
3 PROCESS
• Lacrimal-arises anteriorly from its superior margin
• Articulates – descending process of lacrimal bone
• Forms canal for NLD
• Ethmoidal- arises from a little behind lacrimal process
from sup margin
• Articulates- uncinate process of ethmoid bone
• Maxillary- arises from sup border of inf turbinate &
curves laterally attaches maxilla
32.
AGGER NASI
• mostanterior part of ethmoid,
• most superior remnant of first ET/NT
• small prominence on lateral nasal wall
• just anterior to attachment of the MT
• groove may be seen where the Uncinate
process attaches to lateral wall.
• This is the junction of the uncinate process to
the lacrimal bone.
• .Ant. –frontal pr. Of maxilla
• Superiorly- FR/FS ,
• Anterolaterally –nasal bone
• Inferomedial-UP, Inferolaterally –lacrimal bone
33.
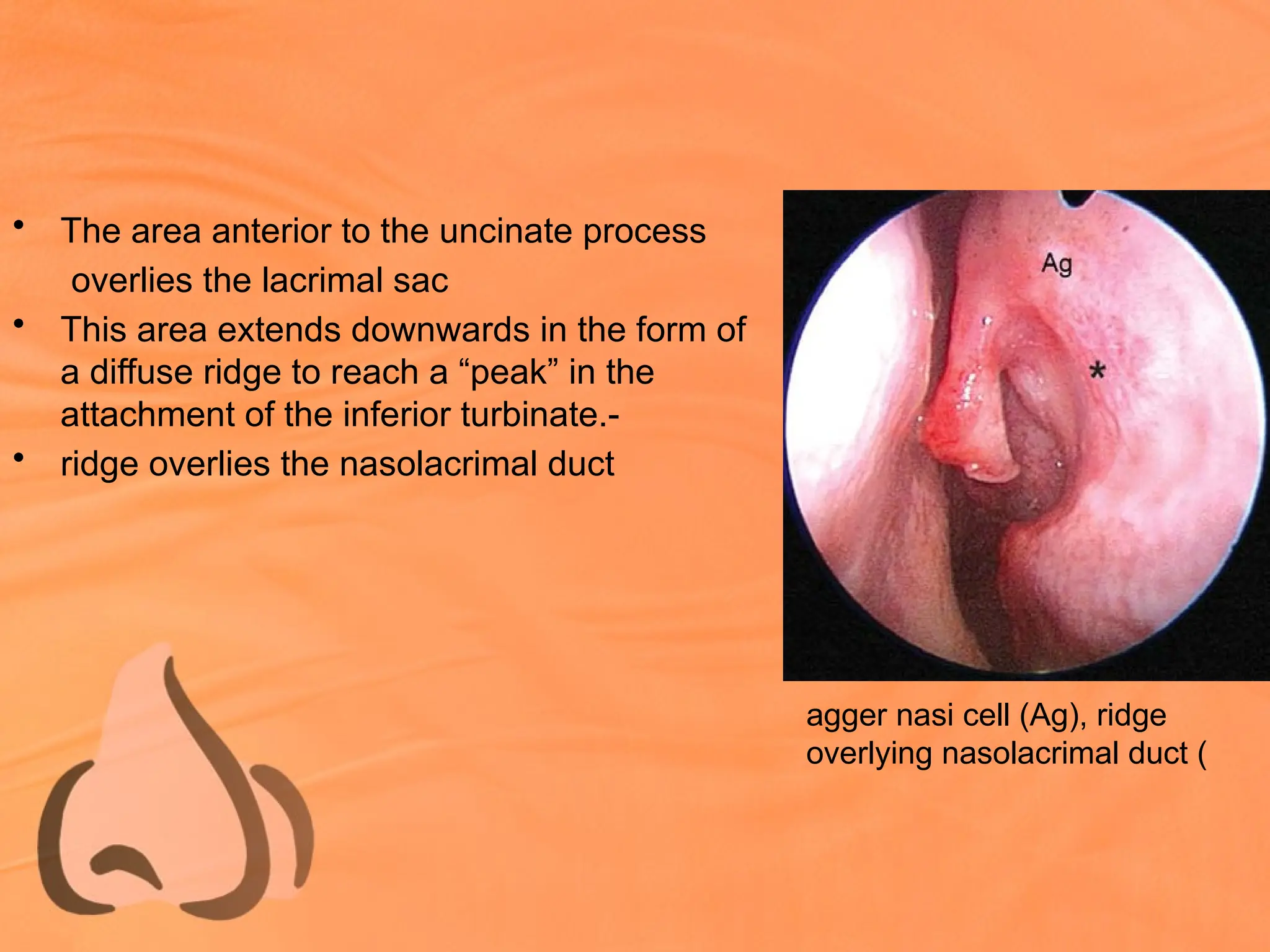
• The areaanterior to the uncinate process
overlies the lacrimal sac
• This area extends downwards in the form of
a diffuse ridge to reach a “peak” in the
attachment of the inferior turbinate.-
• ridge overlies the nasolacrimal duct
agger nasi cell (Ag), ridge
overlying nasolacrimal duct (
34.
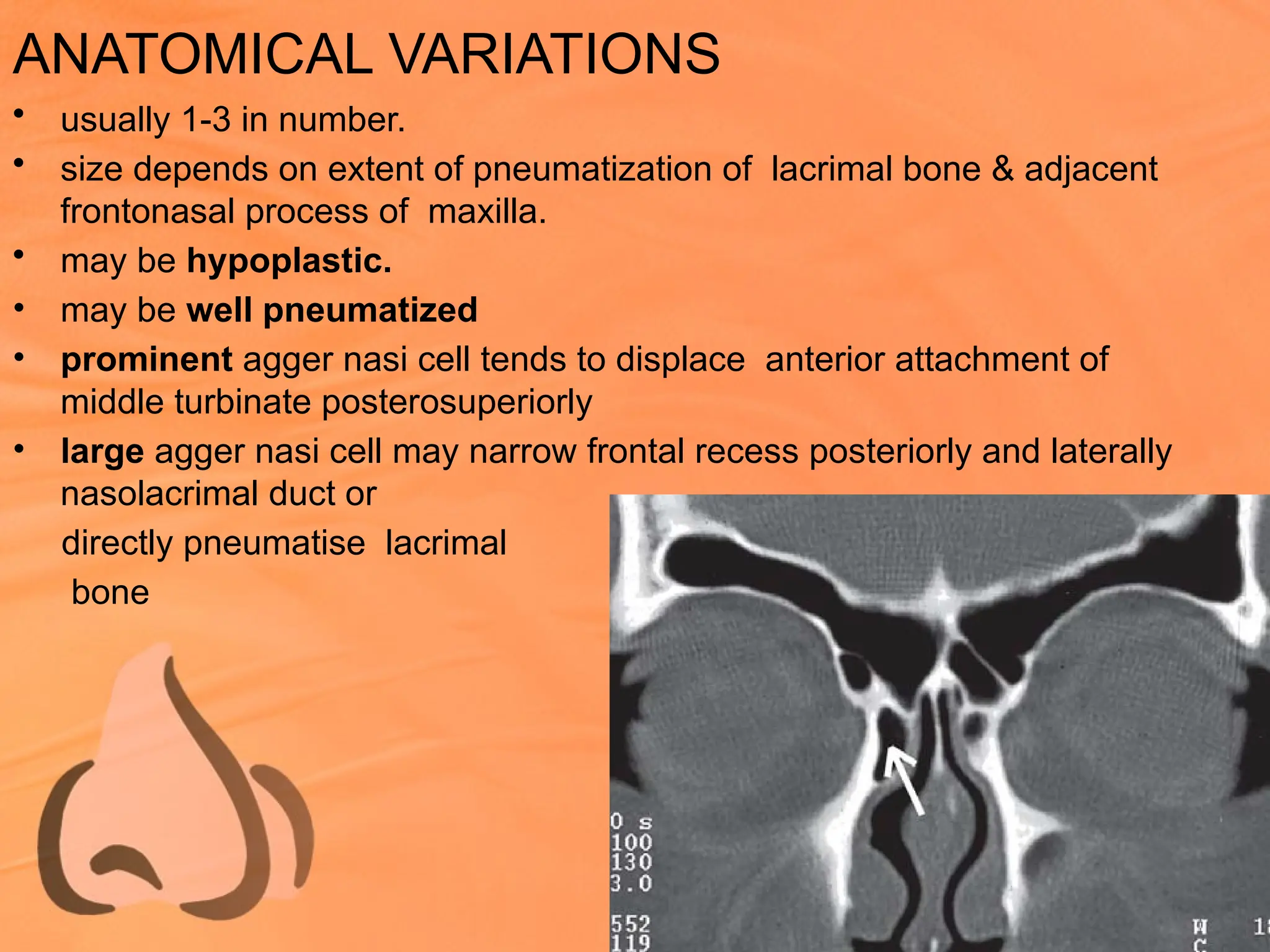
ANATOMICAL VARIATIONS
• usually1-3 in number.
• size depends on extent of pneumatization of lacrimal bone & adjacent
frontonasal process of maxilla.
• may be hypoplastic.
• may be well pneumatized
• prominent agger nasi cell tends to displace anterior attachment of
middle turbinate posterosuperiorly
• large agger nasi cell may narrow frontal recess posteriorly and laterally
nasolacrimal duct or
directly pneumatise lacrimal
bone
35.
MIDDLE TURBINATE (MT)
•Origin- ethmoturbinal
• Convouted structure,dried leaf
• 3 PARTS
• Anterior 1/3rd
- sagittal (vertical) plane
• attachment-skull base – lateral edge of cribriform
• plate at junct of medial & lateral lamella &
• frontal nasal process of maxilla
• This arch like attachment of MT to
cribriform plate – Axilla of MT
• Olfactory fossa
36.
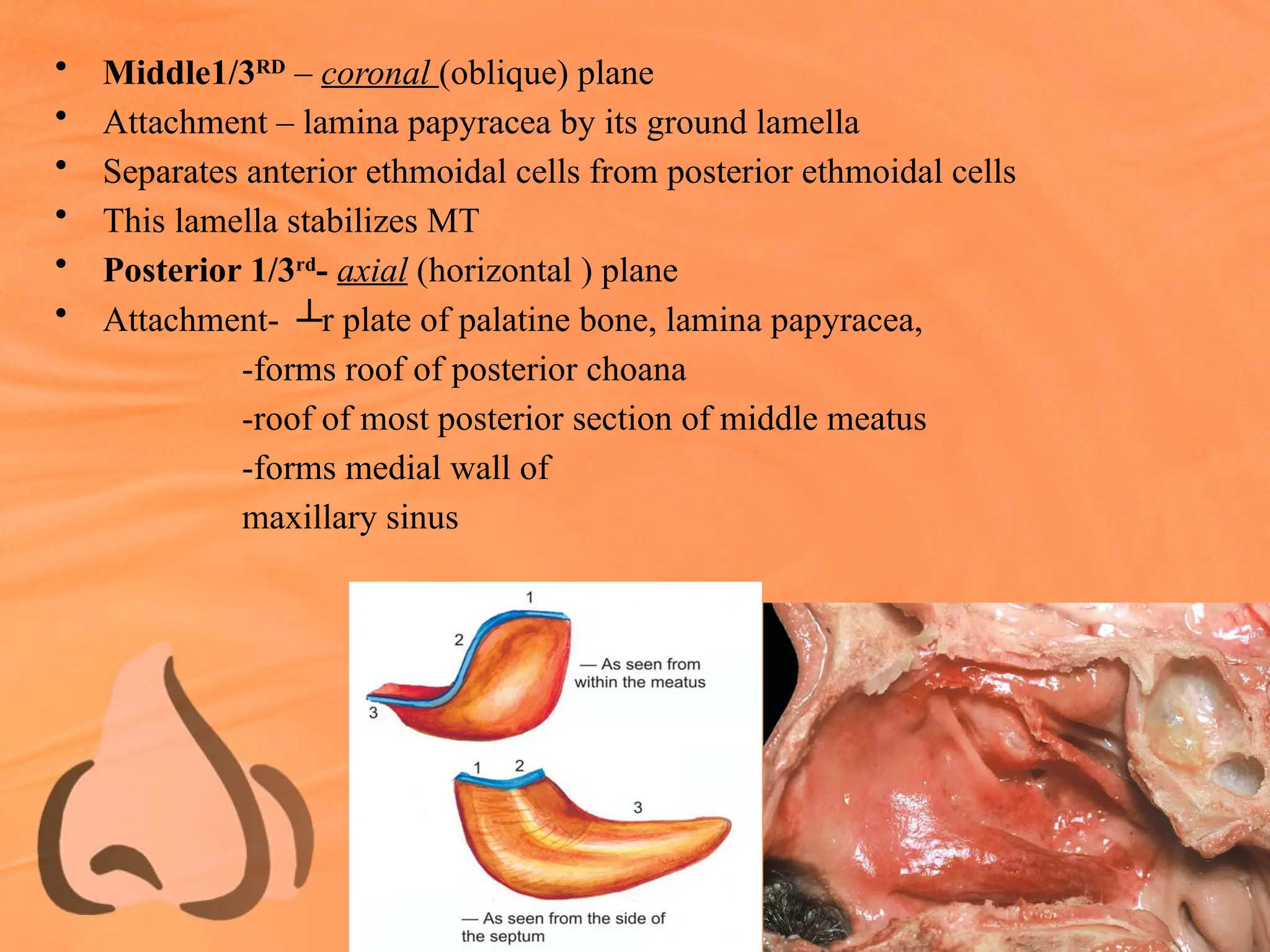
• Middle1/3RD
– coronal(oblique) plane
• Attachment – lamina papyracea by its ground lamella
• Separates anterior ethmoidal cells from posterior ethmoidal cells
• This lamella stabilizes MT
• Posterior 1/3rd
- axial (horizontal ) plane
• Attachment- ┴r plate of palatine bone, lamina papyracea,
-forms roof of posterior choana
-roof of most posterior section of middle meatus
-forms medial wall of
maxillary sinus
37.
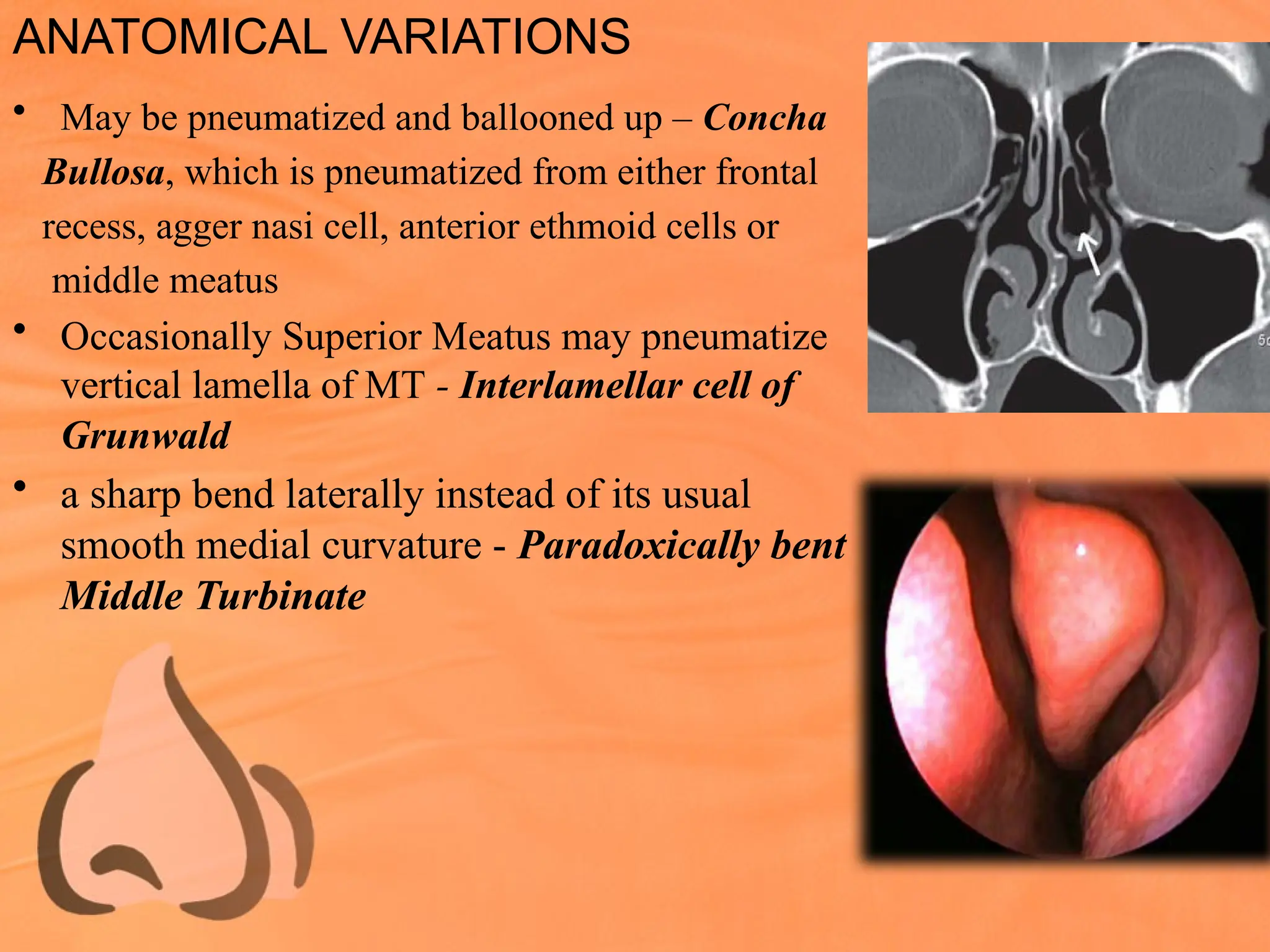
ANATOMICAL VARIATIONS
• Maybe pneumatized and ballooned up – Concha
Bullosa, which is pneumatized from either frontal
recess, agger nasi cell, anterior ethmoid cells or
middle meatus
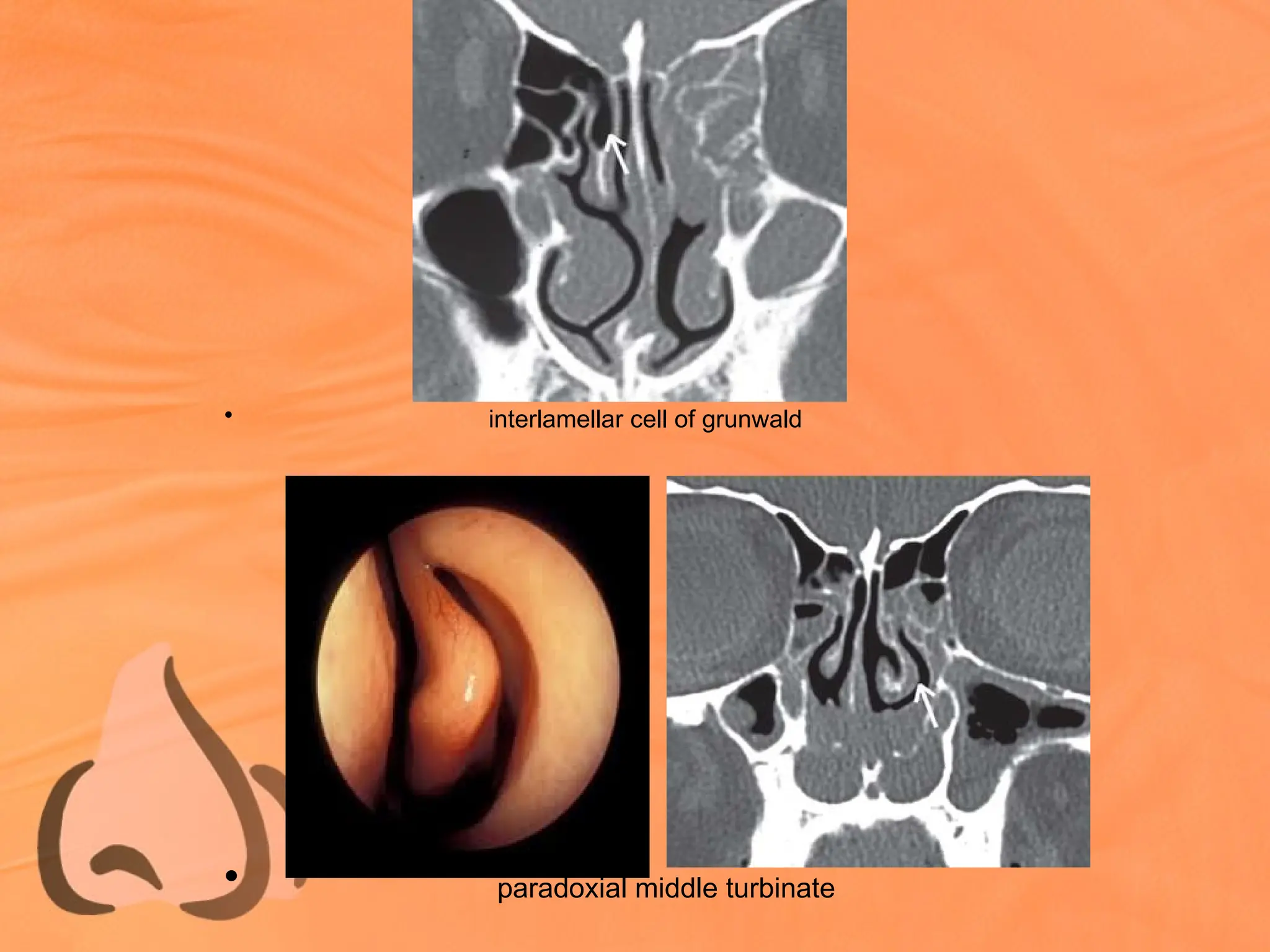
• Occasionally Superior Meatus may pneumatize
vertical lamella of MT - Interlamellar cell of
Grunwald
• a sharp bend laterally instead of its usual
smooth medial curvature - Paradoxically bent
Middle Turbinate
• Often bilateral& can block
infundibulum
• Normally curved MT may curl upon
itself to produce a concavity within it
- Turbinate Sinus
40.
MIDDLE MEATUS
• Lateralto middle turbinate
• receives drainage from the anterior ethmoid, frontal and maxillary sinuses
• Drainage from frontal, maxilary & ant. ethmoidal sinuses
• In disarticulated bone large opening is seen in medial wall of maxillary bone,
maxillary hiatus, which is covered normally by adjacent bones making its
opening narrow
Inf: Maxillary process of Inferor Turbinate
Post: Perpendicular plate of Palatine bone
Anterosup: Descending process of Lacrimal bone
Sup: Uncinate process & Ethmoidal Bulla
• Left out hiatus is filled by: mucous memb of middle meatus & maxillary sinus
with intervening connective tissue- the membranous portion of lateral wall.
41.
• Membranous portion: lying ant or post to
uncinate process, constituting Ant & Post
Fontanelle
• Accessory ostia are found here
• Most frequantly in post fontanelle
Natural Os
• Alwayspresent
• Very difficult to see clinically
• Lies deep in infundibulum (immdtly
post. to NLD)
• Usually oval & tunnel like
• 3 dimension
• Always single
• Lies at the level of MT or upper border
IT
• Small in diameter 3mm to 10mm
• Inferiorly - inferior turbinate,
• superiorly1 to 2 mm -lamina papyracea
and orbit,
• posteriorly - posterior fontanelle,
• anteriorly 0.5 cm -nasolacrimal duct
Accessory Os
• Present about 4-5%
• Easily seen on endoscopy
• Lies in sagittal plane in fontanella
• Usually round & punched out.
• 2 dimension
• Could be multiple
• Lies anywhere in MM
• Could be large up to ½ to 1 cm
44.
• A windowis cut in the middle turbinate to
view the relationship of structures within the
middle meatus
• Most anteriorly is a curved ridge called the
uncinate process.
• Behind this is the well pneumatized and most
constant anterior ethmoidal cell, ethmoidal
bulla.
• These structures are separated by a semilunar
groove -hiatus semilunaris.
• The hiatus semilunaris is 2- dimensional and
leads into a 3-dimensional space called
infundibulum
45.
Osteomeatal Complex
• Commonchannel that links frontal sinus, ant & post ethmoidal sinuses
& maxillary sinus to middle meatus that allows airflow and
mucociliary drainage
• OMC- uncinate process
bulla ethmoidalis
hiatus semilunaris
infundibulum
maxillary ostium
46.
• Boundaries:
Medial- MiddleTurbinate
Lateral - lamina papyracea
Sup & post - basal lamella
Inf & Ant – open
• Space contains:
Agger nasi, nasofrontal recess,
infundibulam, bulla, ant
ethmoidal cells
47.
UNCINATE PROCESS
• Thinbent hook/sickle shaped structure
• Parts-vertical, horizontal & intermediate transitional part
• Runs in sagittal plane from anteriosuperior to posterioinferior
• Margins – Posterosup. - sharp, concave & lies parallel to ant. surface
of ethmoidal bulla.
• Posteroinf – lamina perpendicularis of palatine bone & ethmoidal
process of inf. turbinate.
• Anterior– convex, contact with bony lateral wall & can extent upto
lacrimal bone
• upper end of the uncinate process lies within the frontal recess.
48.
Anatomical variations
Upper endshows great variation
• UP attaches laterally to the lamina
papyracea-
• it’s upper end encloses within it a
blind recess called recessus
terminalis - commonest mode of
drainage of the frontal sinus is medial
to the uncinate process
• UP attach to the skull base.
• In this case the frontal sinus drains
into infundibulum and therefore
disease from the frontal sinus can
spread to the maxillary sinus and vice
versa
49.
• UP maybend medially to attach
to the middle turbinate
• UP may lie free within the
middle meatus and not attach to
any adjacent bony structure
50.
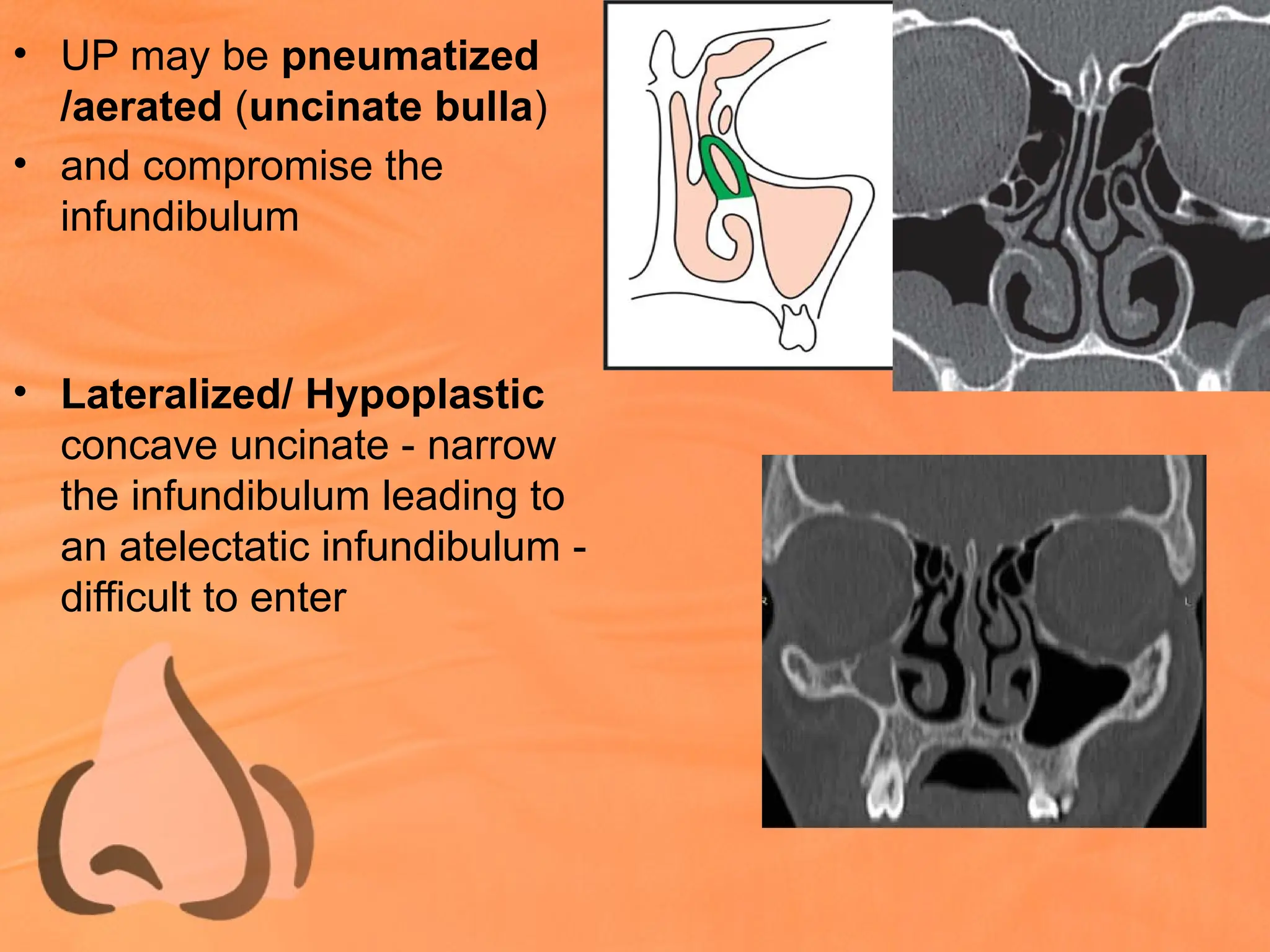
• UP maybe pneumatized
/aerated (uncinate bulla)
• and compromise the
infundibulum
• Lateralized/ Hypoplastic
concave uncinate - narrow
the infundibulum leading to
an atelectatic infundibulum -
difficult to enter
51.
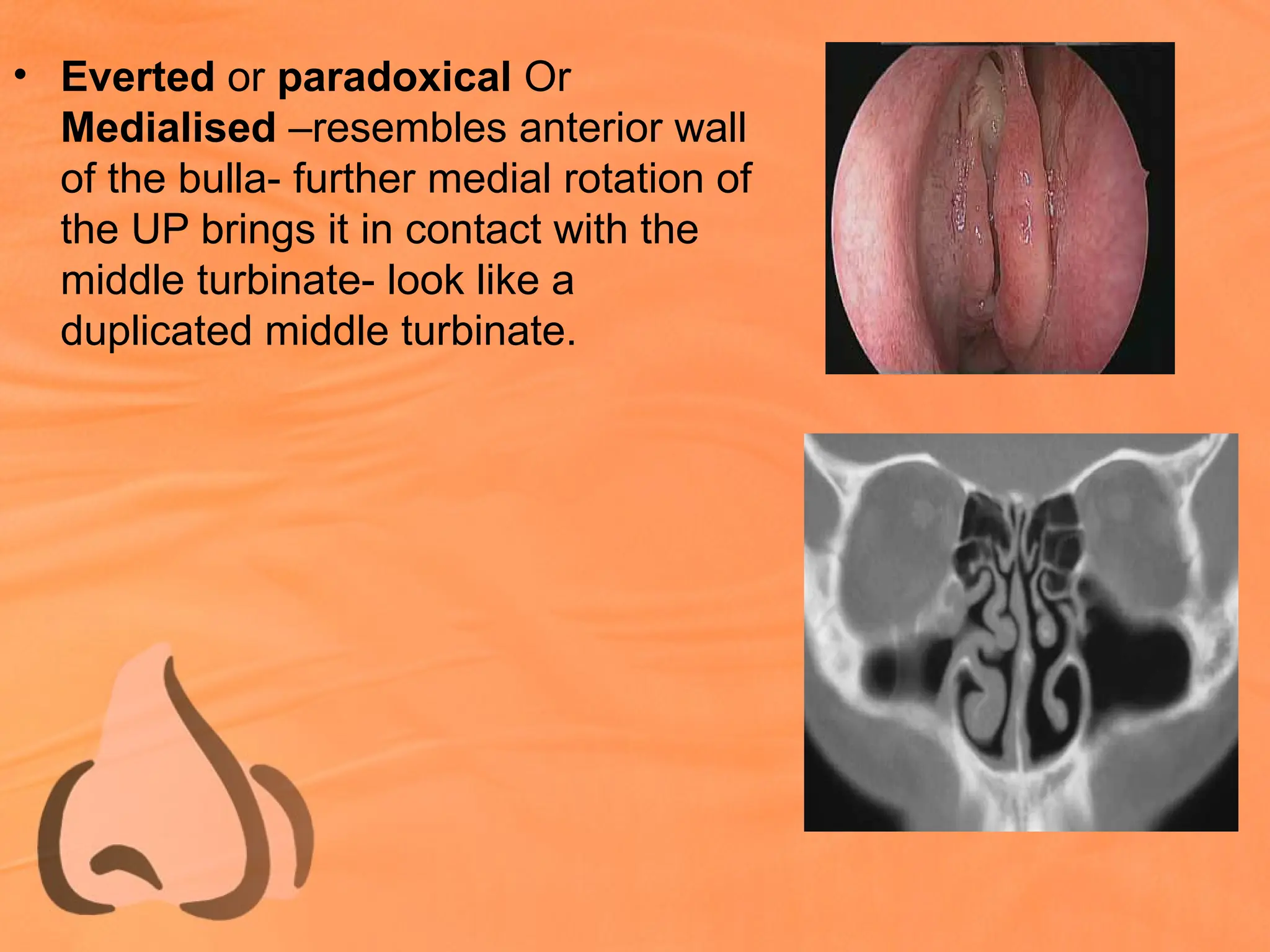
• Everted orparadoxical Or
Medialised –resembles anterior wall
of the bulla- further medial rotation of
the UP brings it in contact with the
middle turbinate- look like a
duplicated middle turbinate.
52.
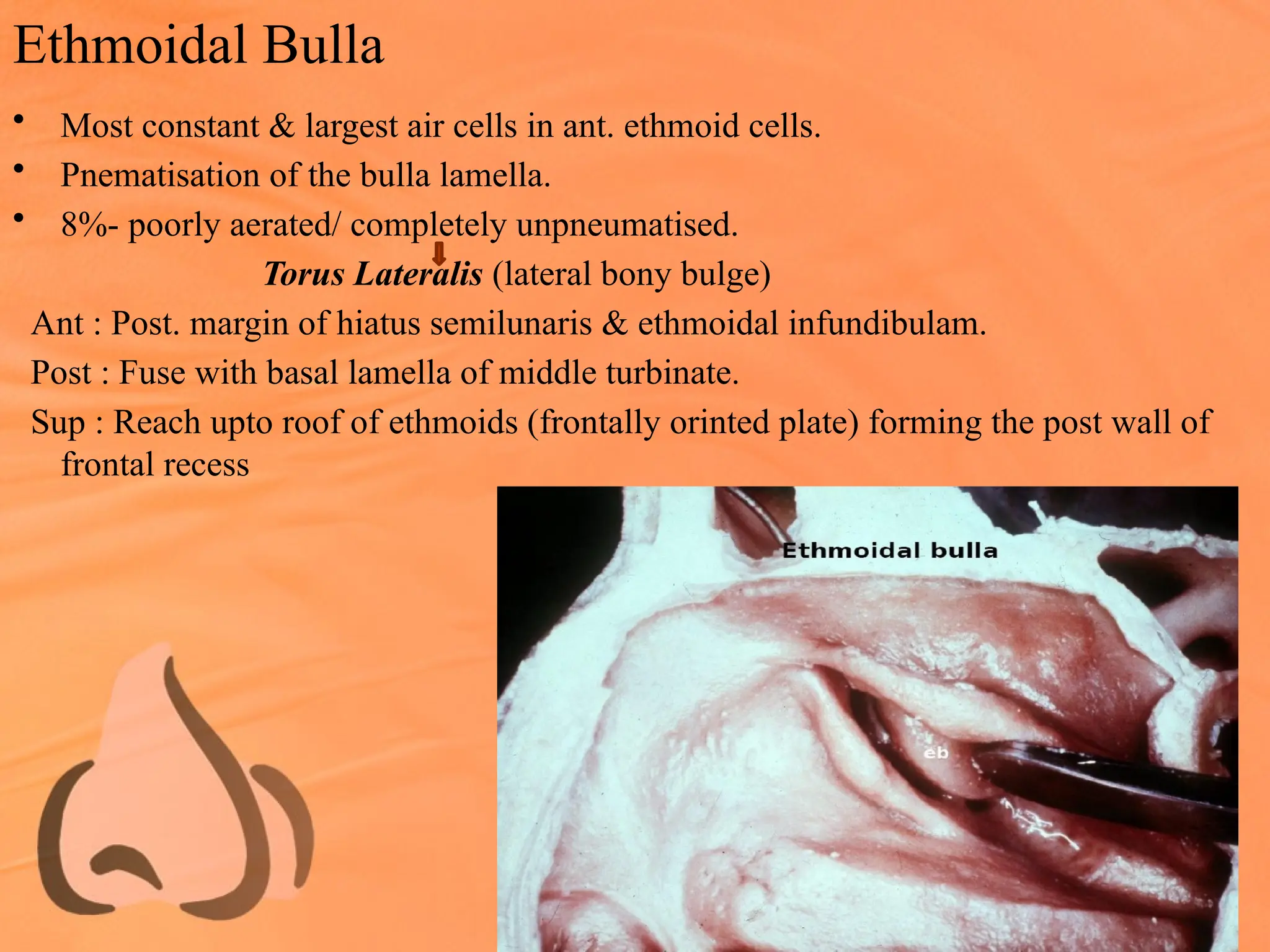
Ethmoidal Bulla
• Mostconstant & largest air cells in ant. ethmoid cells.
• Pnematisation of the bulla lamella.
• 8%- poorly aerated/ completely unpneumatised.
Torus Lateralis (lateral bony bulge)
Ant : Post. margin of hiatus semilunaris & ethmoidal infundibulam.
Post : Fuse with basal lamella of middle turbinate.
Sup : Reach upto roof of ethmoids (frontally orinted plate) forming the post wall of
frontal recess
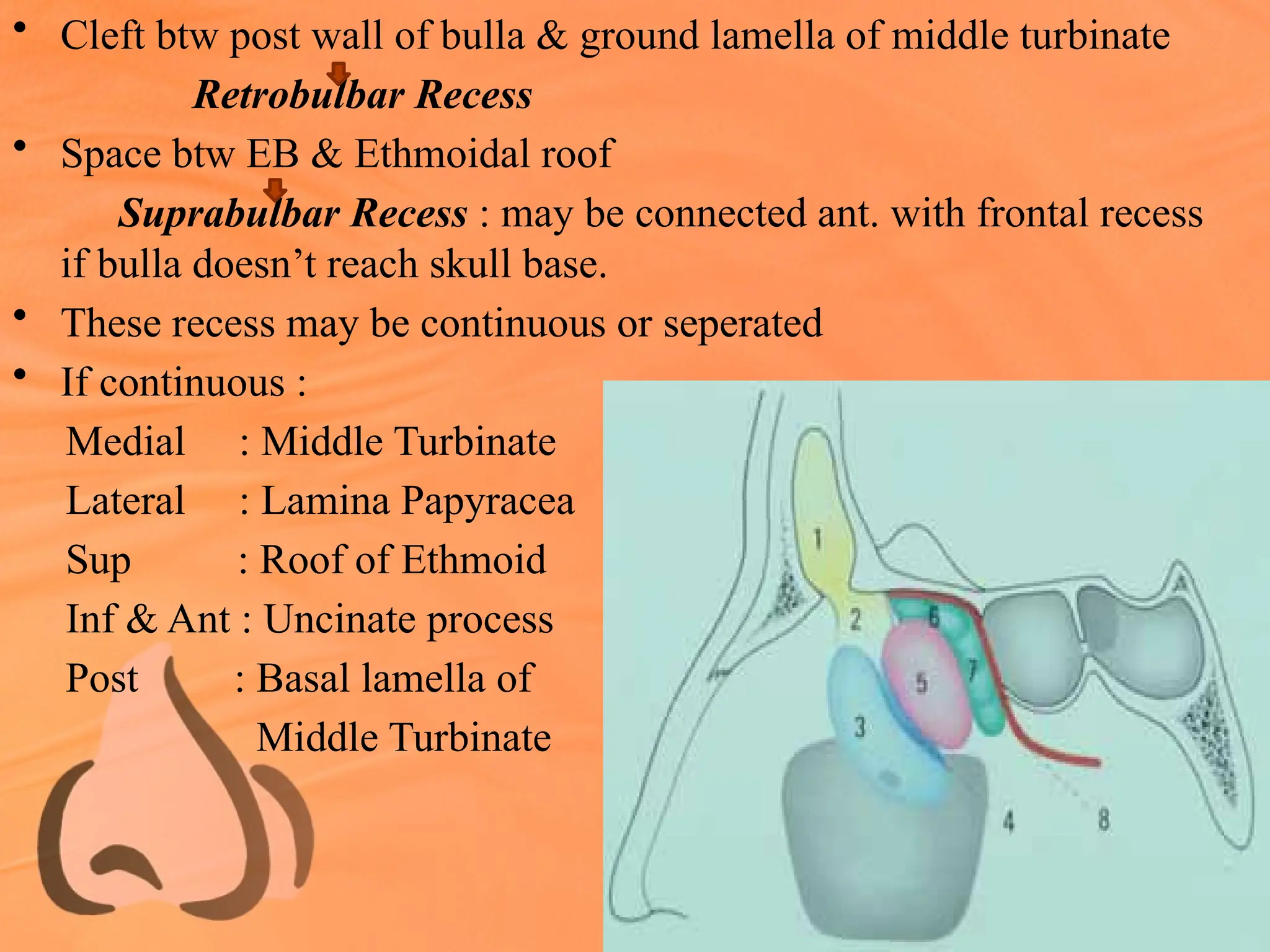
• Cleft btwpost wall of bulla & ground lamella of middle turbinate
Retrobulbar Recess
• Space btw EB & Ethmoidal roof
Suprabulbar Recess : may be connected ant. with frontal recess
if bulla doesn’t reach skull base.
• These recess may be continuous or seperated
• If continuous :
Medial : Middle Turbinate
Lateral : Lamina Papyracea
Sup : Roof of Ethmoid
Inf & Ant : Uncinate process
Post : Basal lamella of
Middle Turbinate
55.
Suprabulbar Recess
If theethmoidal bulla do not reach the ethmoidal roof
Btw the superior aspect of the bulla and the ethmoidal roof
Air containing space,
Boundaries
Inf: Roof of the ethmoidal bulla,
Medial: Middle turbinate,
Lateral: Lamina papyracea
Superiorly: Roof of the ethmoid.
Laterally it may give rise to an air-containing
cleft extending above the orbit – supraorbital recess
Suprabullar recess may open into frontal recess
56.
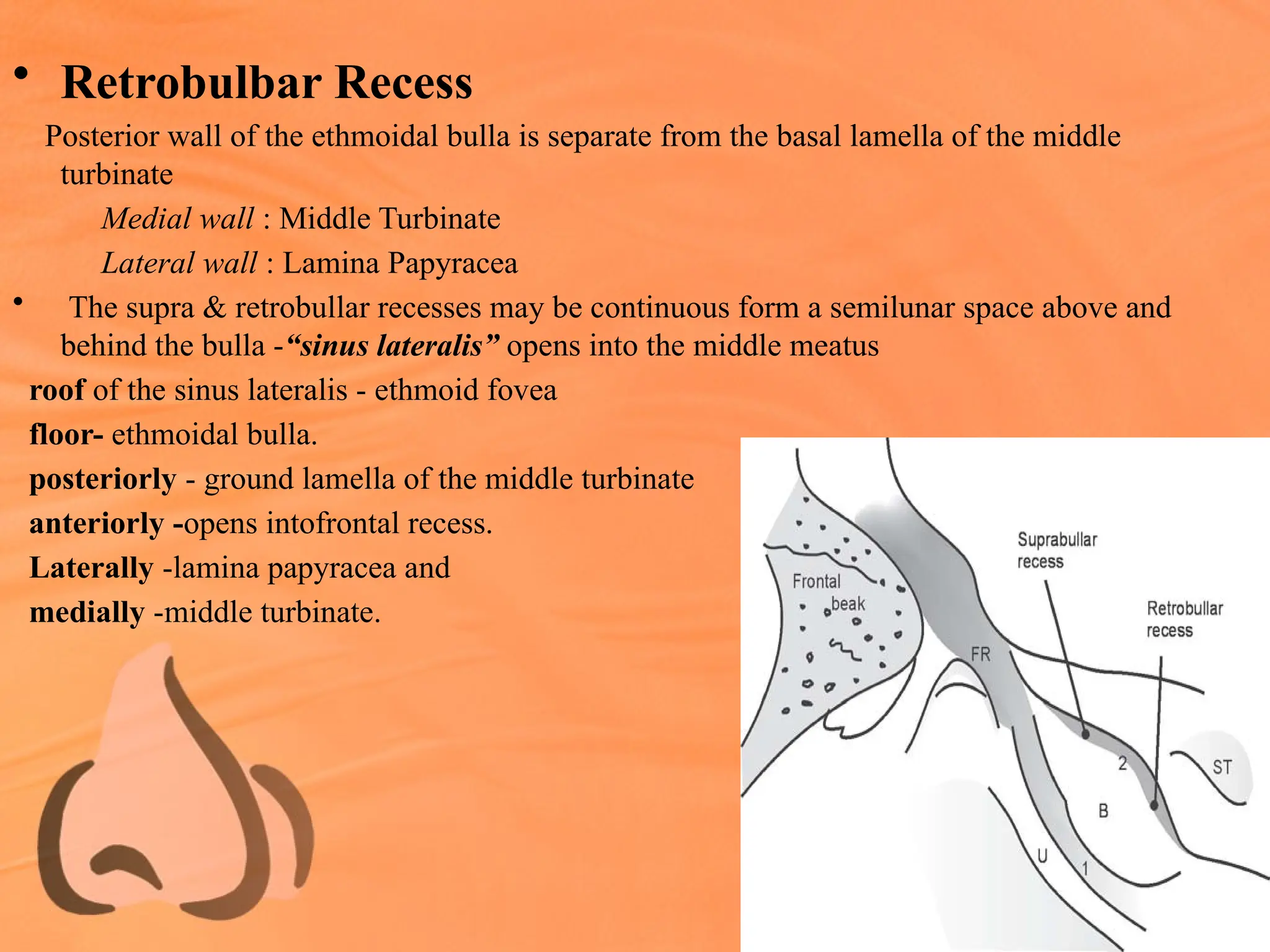
• Retrobulbar Recess
Posteriorwall of the ethmoidal bulla is separate from the basal lamella of the middle
turbinate
Medial wall : Middle Turbinate
Lateral wall : Lamina Papyracea
• The supra & retrobullar recesses may be continuous form a semilunar space above and
behind the bulla -“sinus lateralis” opens into the middle meatus
roof of the sinus lateralis - ethmoid fovea
floor- ethmoidal bulla.
posteriorly - ground lamella of the middle turbinate
anteriorly -opens intofrontal recess.
Laterally -lamina papyracea and
medially -middle turbinate.
57.
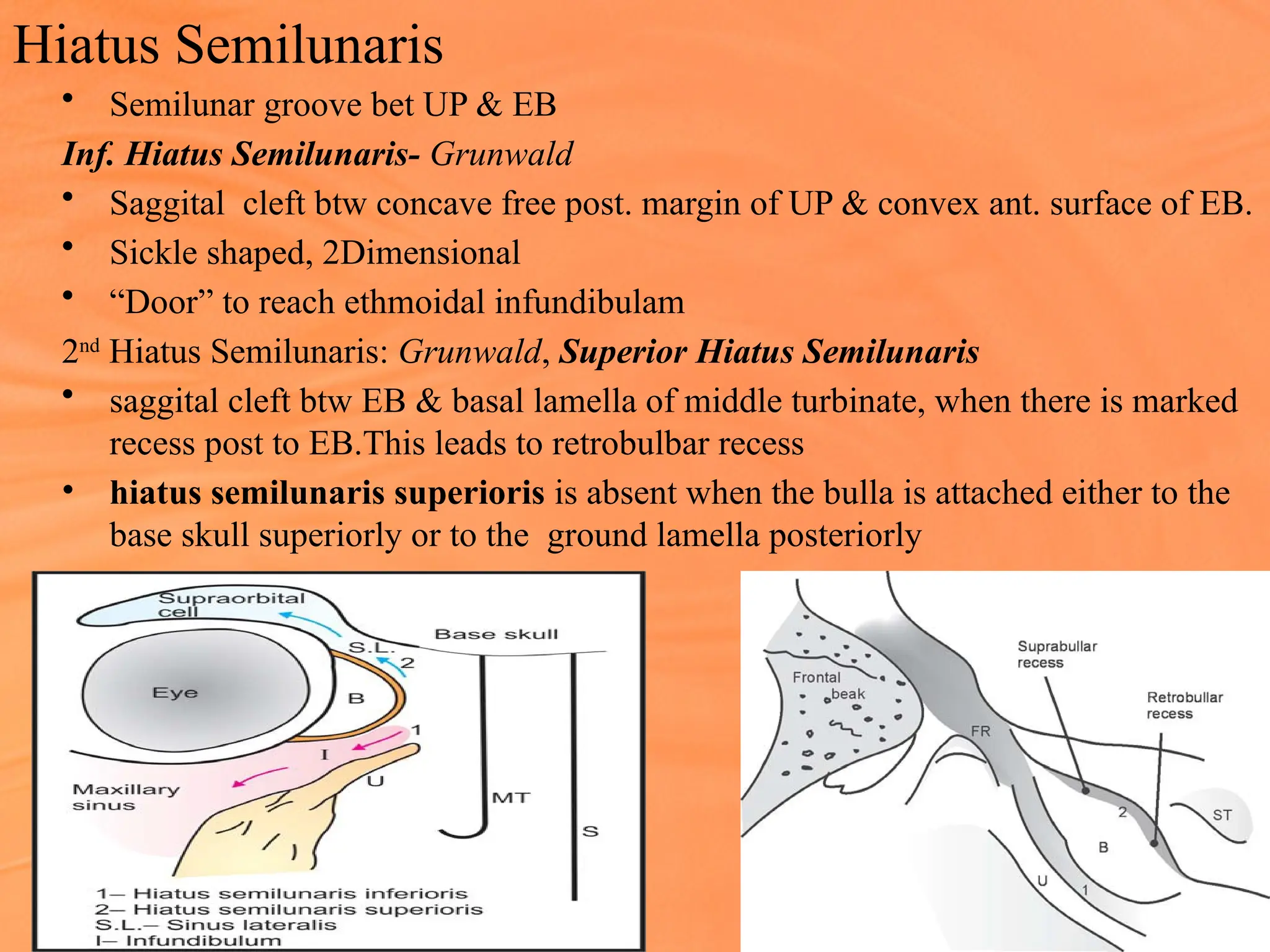
Hiatus Semilunaris
• Semilunargroove bet UP & EB
Inf. Hiatus Semilunaris- Grunwald
• Saggital cleft btw concave free post. margin of UP & convex ant. surface of EB.
• Sickle shaped, 2Dimensional
• “Door” to reach ethmoidal infundibulam
2nd
Hiatus Semilunaris: Grunwald, Superior Hiatus Semilunaris
• saggital cleft btw EB & basal lamella of middle turbinate, when there is marked
recess post to EB.This leads to retrobulbar recess
• hiatus semilunaris superioris is absent when the bulla is attached either to the
base skull superiorly or to the ground lamella posteriorly
58.
Anatomical Variations
Ethmoidal Bulla
•May be hypoplastic or rarely even a solid
non-pneumatized hillock
• More commonly - extensively
pneumatized to produce a large bulge,
which abuts against UP ant or MT,
compromising infundibulum or middle
meatus respectively.
59.
Ethmoid Air Cells
•Ant & post ethmoid air cells may pneumatize surrounding bones
like lacrimal , maxilla, frontal & sphenoid bone to produce
varying patterns of pneumatization - “migrated” air cells
60.
• Ant ethmoidcells pneumatize lacrimal bone & frontonasal process
of maxilla to produce agger nasi cells. Well pneumatized produce a
distinct bulge on lateral nasal wall & compromise drainage of
frontal recess.
• Ant ethmoid cells may pneumatize roof of maxillary sinus -
Haller’s cell & it is usually seen in floor of orbit at level btw
inferior and medial rectus - compromise the infundibulum
61.
• Ant ethmoidcells may migrate
into frontal recess area -frontal
cells, four types:
Type I: A single cell above
agger nasi cell
• Type II: Two or more cells
above agger nasi cell
62.
• Type III:(Frontal bulla) A cell which
extends well into frontal sinus &
simulates frontal sinus itself on
endoscopy
• Type IV: An isolated “loner cell”
within frontal sinus
63.
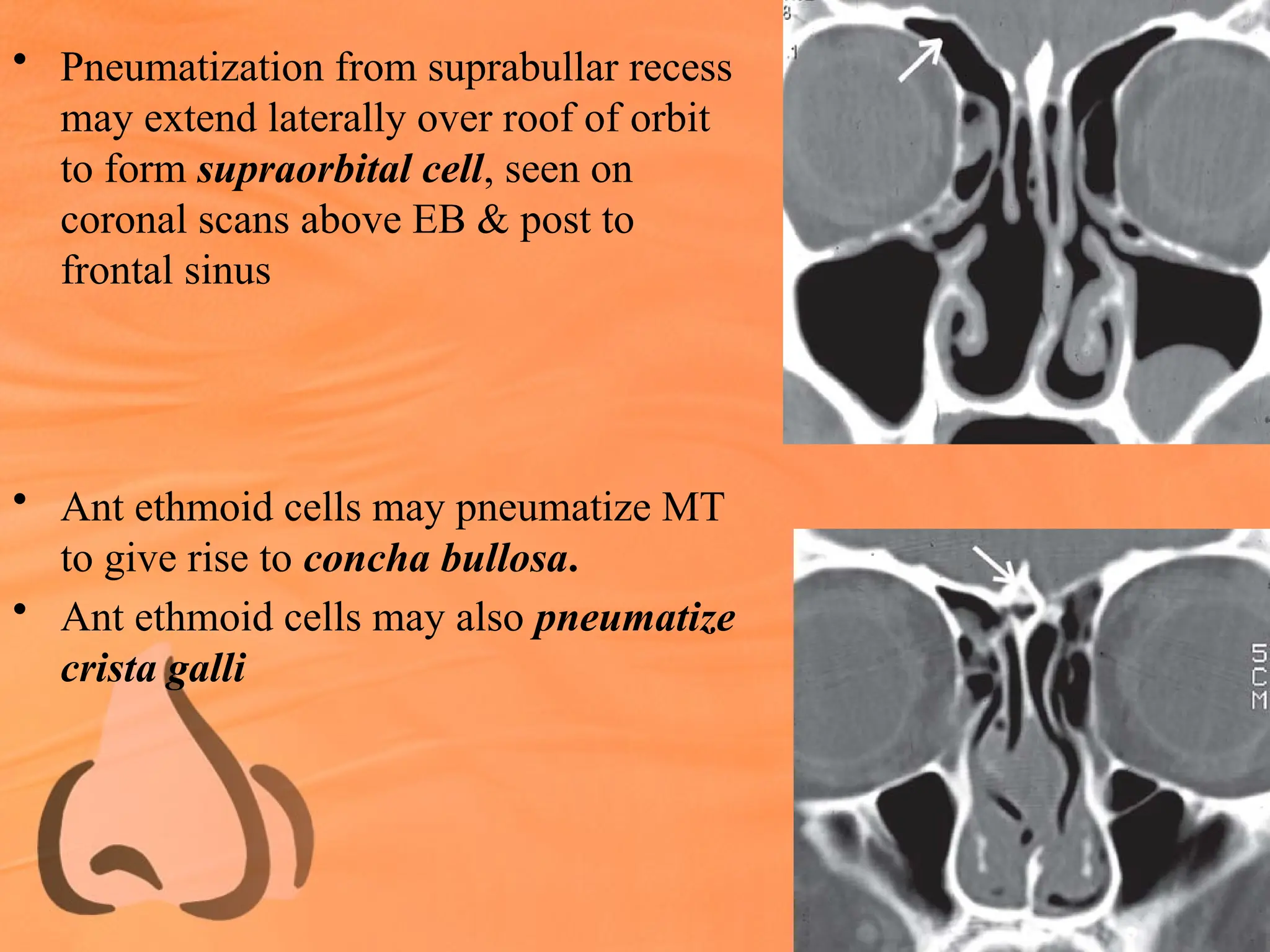
• Pneumatization fromsuprabullar recess
may extend laterally over roof of orbit
to form supraorbital cell, seen on
coronal scans above EB & post to
frontal sinus
• Ant ethmoid cells may pneumatize MT
to give rise to concha bullosa.
• Ant ethmoid cells may also pneumatize
crista galli
64.
• Post ethmoidcells may pneumatize sphenoid bone posteriorly
to give rise to a cell, which extends superolateral to sphenoid
sinus - Onodi cell
• Optic nerve & at times internal carotid artery are in close
relation with lateral wall of this cell rather than with sphenoid
sinus
65.
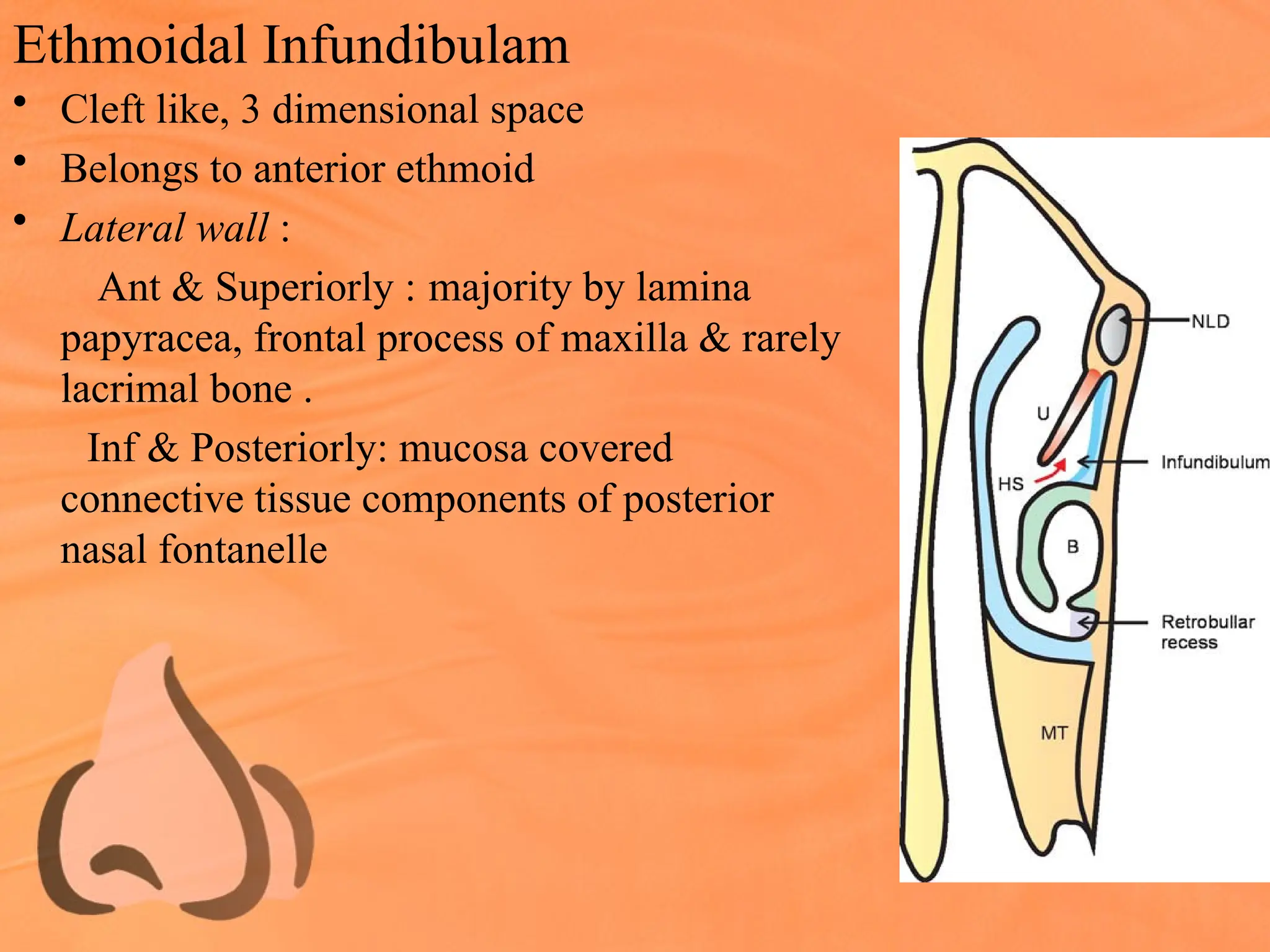
Ethmoidal Infundibulam
• Cleftlike, 3 dimensional space
• Belongs to anterior ethmoid
• Lateral wall :
Ant & Superiorly : majority by lamina
papyracea, frontal process of maxilla & rarely
lacrimal bone .
Inf & Posteriorly: mucosa covered
connective tissue components of posterior
nasal fontanelle
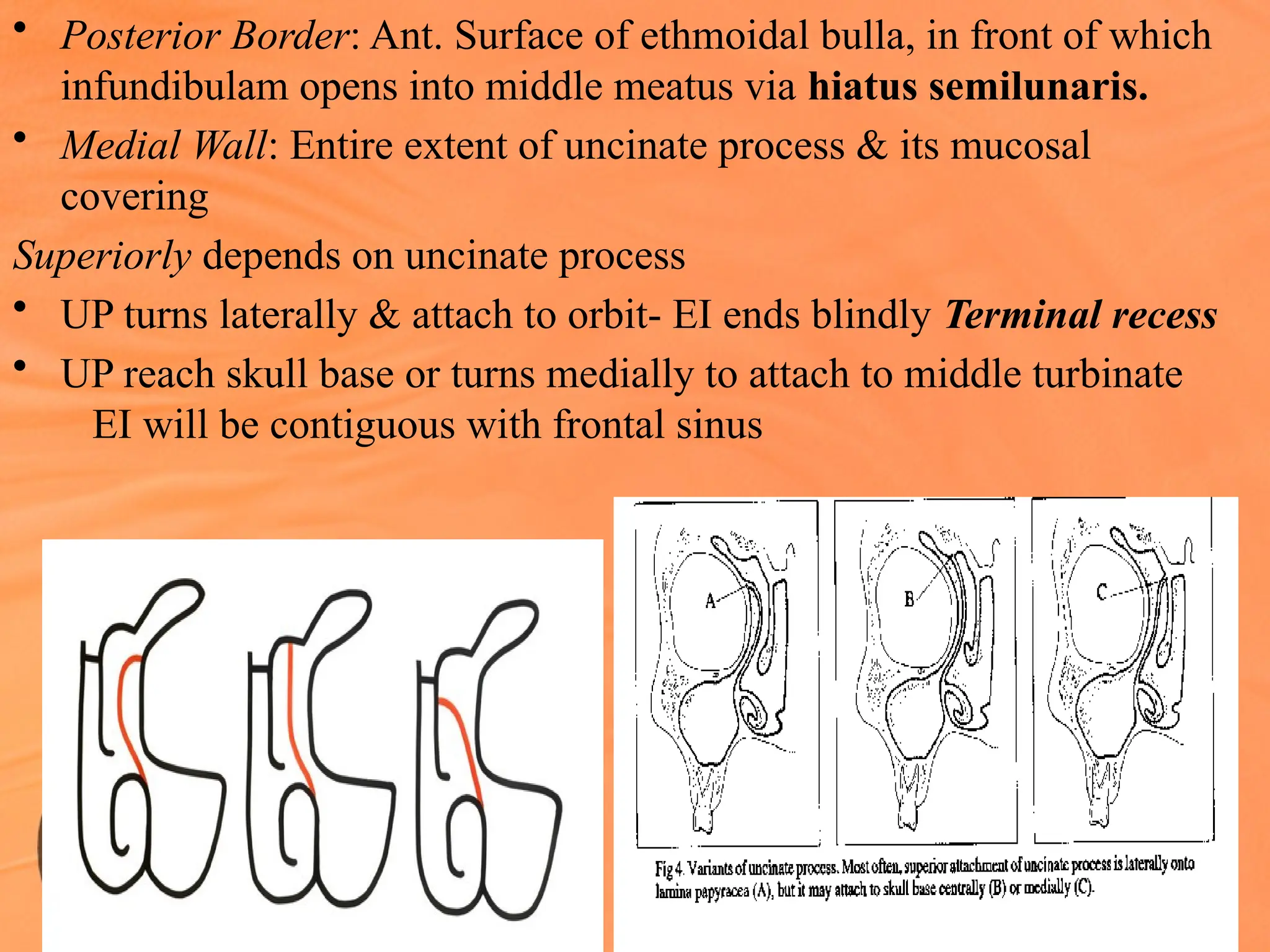
66.
• Posterior Border:Ant. Surface of ethmoidal bulla, in front of which
infundibulam opens into middle meatus via hiatus semilunaris.
• Medial Wall: Entire extent of uncinate process & its mucosal
covering
Superiorly depends on uncinate process
• UP turns laterally & attach to orbit- EI ends blindly Terminal recess
• UP reach skull base or turns medially to attach to middle turbinate
EI will be contiguous with frontal sinus
67.
• If terminalrecess is present :
EI & frontal recess are separate, in this case frontal recess
opens in the middle meatus medial to EI, btw uncinate process &
middle turbinate.
Posteriorly, tapers parallel to tapering of UP
• Ant length of EI- 4-5 cm
• Greatest depth -12cm ( measured from free post margin of UP)
• Greatest width – 5-6cm ( measured from free margin of UP to lamina
papyracea)
• Maxillary sinus ostium- medial wall of EI at middle & post third.
68.
Frontal Recess
• Anterosup.portion of middle meatus.
• May be defined as:
Ant : Pneumatisation of aggar nasi cells
medial : Middle turbinate,UP
Lateral : Lamina papyracea, lacrimal bone
Sup : Skull base, frontal sinus & ostium
Inf : Depend on attachment of UP (open to infundibulam or middle meatus)
Post : Bulla, bulla lamella, ant. ethmoidal artery
• Natural ostium of frontal sinus - variable
Most frequantly- hour glass narrowing
Rarely – longer narrowed region
10% - multiple ostia
69.
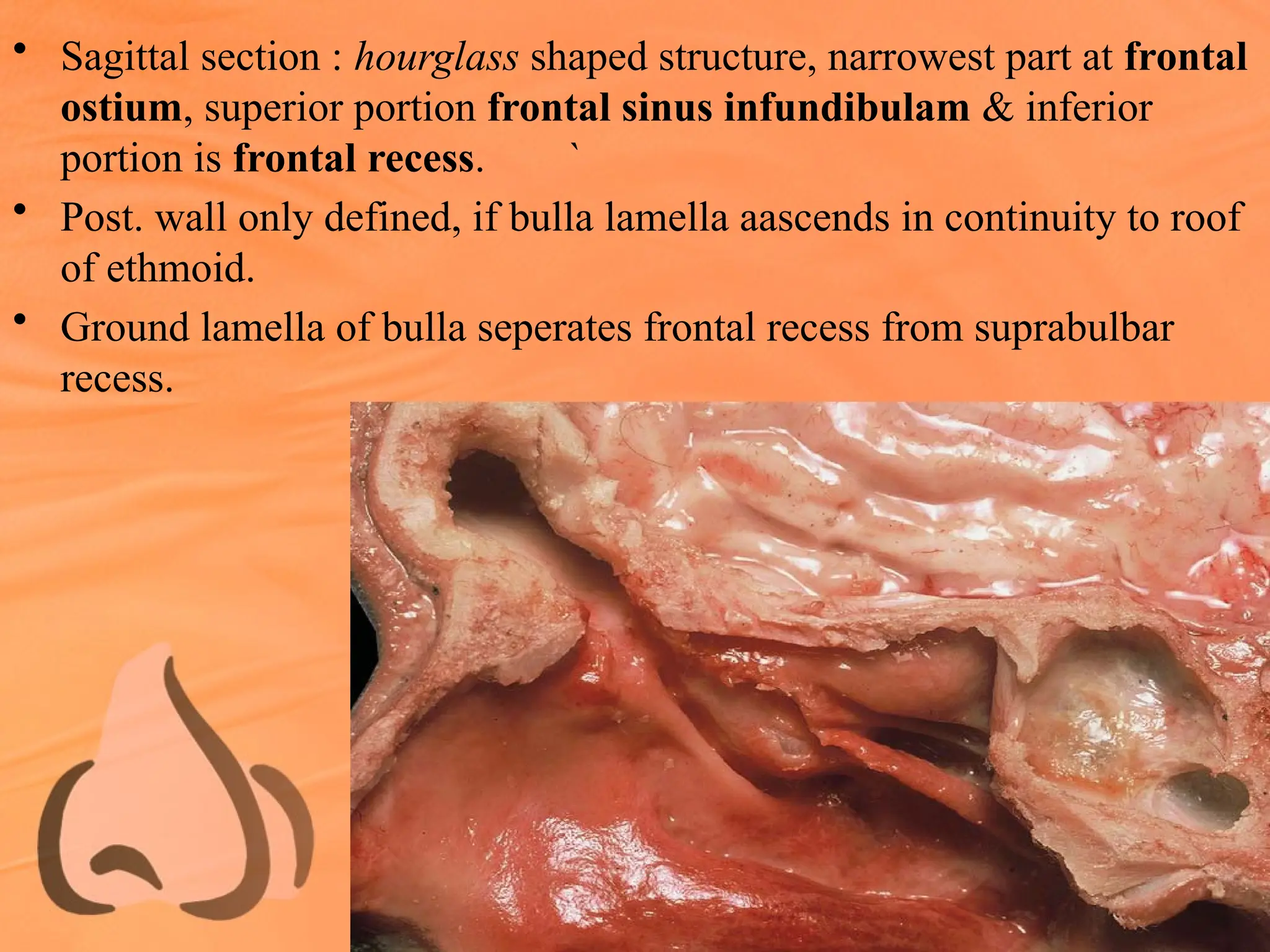
• Sagittal section: hourglass shaped structure, narrowest part at frontal
ostium, superior portion frontal sinus infundibulam & inferior
portion is frontal recess. `
• Post. wall only defined, if bulla lamella aascends in continuity to roof
of ethmoid.
• Ground lamella of bulla seperates frontal recess from suprabulbar
recess.
70.
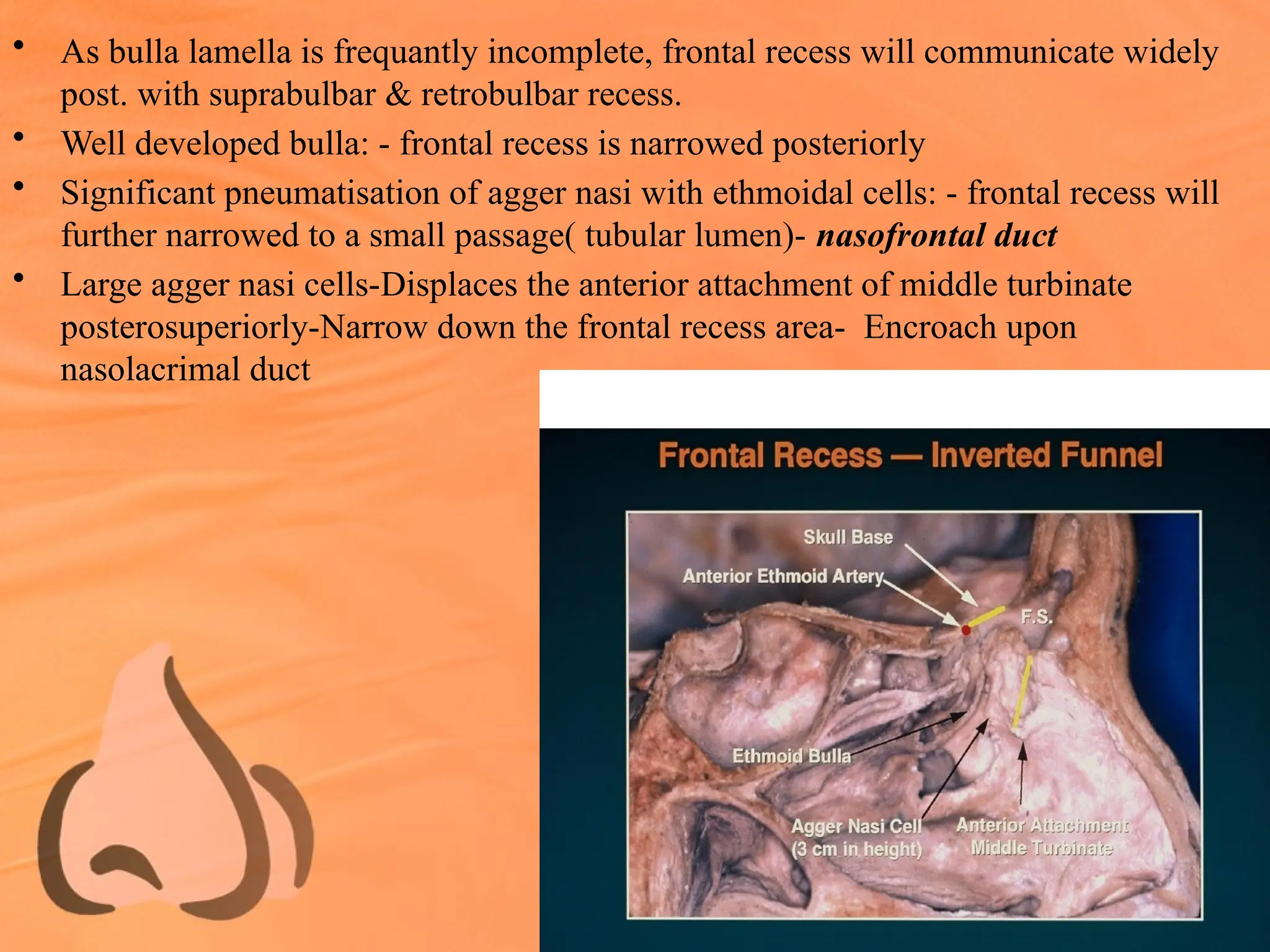
• As bullalamella is frequantly incomplete, frontal recess will communicate widely
post. with suprabulbar & retrobulbar recess.
• Well developed bulla: - frontal recess is narrowed posteriorly
• Significant pneumatisation of agger nasi with ethmoidal cells: - frontal recess will
further narrowed to a small passage( tubular lumen)- nasofrontal duct
• Large agger nasi cells-Displaces the anterior attachment of middle turbinate
posterosuperiorly-Narrow down the frontal recess area- Encroach upon
nasolacrimal duct
71.
Anterior Ethmoidal Artery
•Course is of clinical significance
As in its course from orbit to olfactory fossa,
it traverse three cavities : Orbit
Ethmoidal labrynth
Ant. cranial fossa
• Most critical area- were it enters ant cranial
fossa through lateral lamella of lamina
cribrosa ( thinnest area)
• Origin:- opthalmic artery in orbit, passes
btw sup oblique & medial rectus muscle
• Passes through ant ethmoidal foramen into
anterior ethmoid.
72.
• Cross antethmoidal either:
at level of ethmoidal roof, or
as much as 5mm below roof ( running in mucous memb fold or thin bony
mesentry in the roof)
• Artery is surrounded by thin walled bony channel, dehiscent in 40%
• Artery enters olfactory fossa, (intracarnial) via lamina cribrosa
• Turns anteriorly forming a groove in lateral lamella- ethmoidal sulcus, gives of ant
meningeal branches
• Reach nasal cavity through cribroethmoidal foramen & cribriform plate, divides
into ant nasal artery with sup, lat, medial br, as well as post branch
73.
• M/C siteto find AEA- Suprabulbar recess (85%)
• Unilateral absent ant ethmoidal artery- 14%
• Bilateral absent ant ethmoidal artery - 2%
• Multiple ant ethmoidal artery – 30%
• Absent ant ethmoidal artery- replaced by branch of
post ethmoidal artery
• CSF leakage- trauma in the area were it enter
olfactory foss – dura is not only thin but firmly
adherent to bone
• Infraorbital hematoma
Posterior Ethmoidal Complex
•Ground lamella of middle turbinate is the border btw ant & post ethmoidal sinuses
• All cells opening post to basal lamella
• Spenoid sinus opens into sphenoethmoidal recess medial to sup turbinate
• Number 1-5
• Most post cells can develop laterally & or superiorly
optic nerve & int carotid artery bulge into spheno ethmoidal cells onodi cells
77.
Superior Meatus
• Postethmoid cells open
• Related to superior turbinate
• 60-67% supreme is seen above superior
turbinate
• Sphenoethmoidal Recess
Medial to sup turbinate
Ostium of sphenoid
sinus
78.
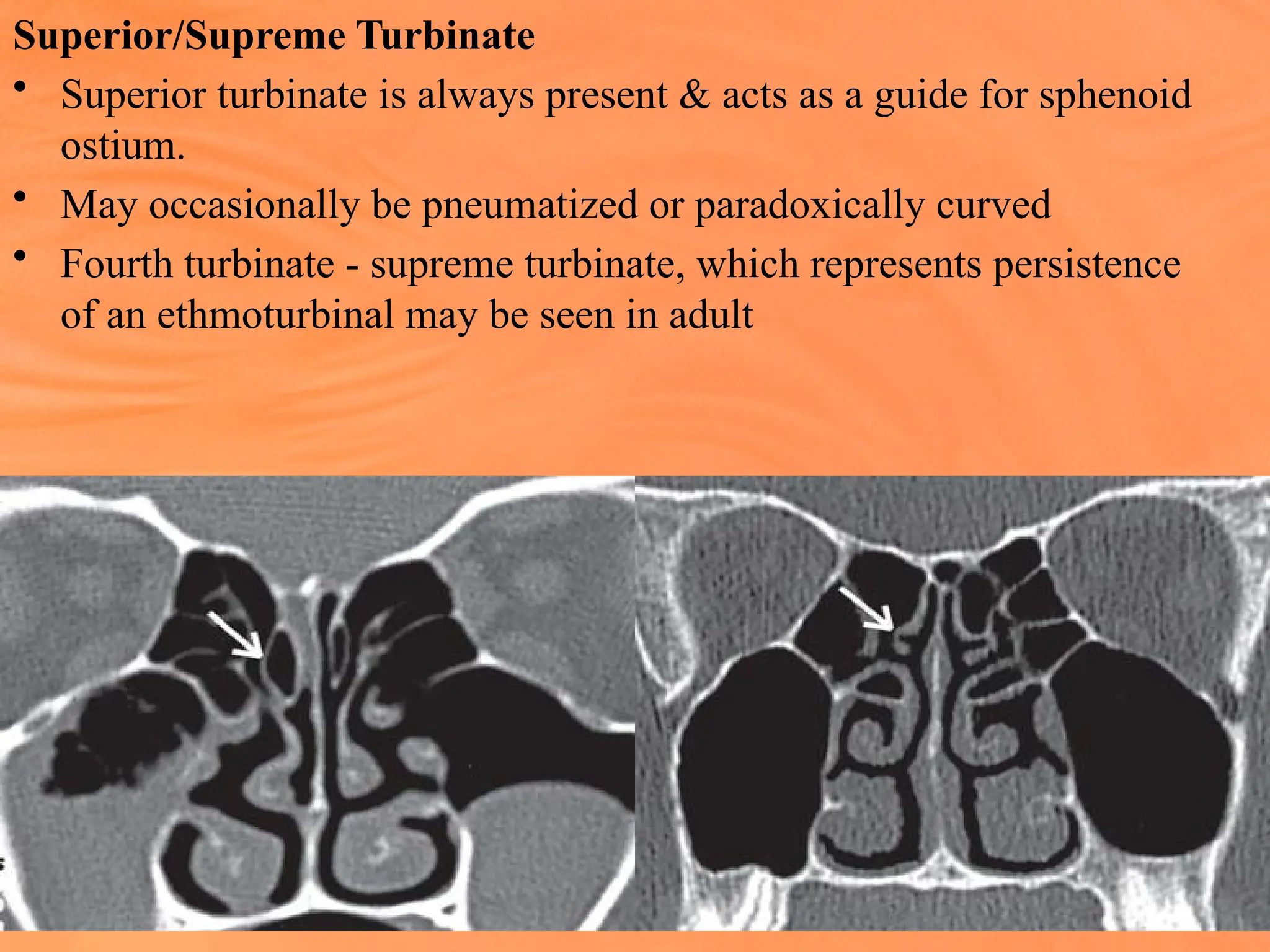
Superior/Supreme Turbinate
• Superiorturbinate is always present & acts as a guide for sphenoid
ostium.
• May occasionally be pneumatized or paradoxically curved
• Fourth turbinate - supreme turbinate, which represents persistence
of an ethmoturbinal may be seen in adult
79.
Sphenoid Ostium
• Medialto posterior sup. turbinate
• Located between nasal septum and inferior aspect of sup.
turbinate
• Located at the same level as the roof of the maxillary sinus
• Located 1-1.5 cm above the roof of post choana &
approximately 2-3 mm away from the septum.
• Drains into sphenoethmoidal recess
80.
Sphenopalatine Foramen
• Boundaries:
Above:Body of Sphenoid
Front: Orbital process of Palatine bone
Below: Upper border of perpendicular plate of palatine bone
Ant margin - related to projection in palatine bone - Ethmoidal
crest- postinf base of middle turbinate attach
• Opens- middle or superior meatus
• Transmit: sphenopalatine A & V, Nasopalatine N
• Sphenopalatine branches out into post lat nasal & post septal
beyond foramen; 39%- divide before foramen
81.
Blood Supply
• INTERNAL& EXTERNAL CAROTID ARTERY
• Majority- Sphenopalatine branch of maxillary (ECA), enters through
sphenopalatine foramen ( lies just inferior to horizontal attachment of middle
turbinate, which is usually damaged due to excessive enlargement of middle
meatal antrostomy)
Branches enter posteriorly to turbinate & meatus
• On concha, vessels are partially embedded in deep groves
• Inferior Meatus- sphenopalatine dips below level of palate to re-emerge anteriorly,
leaving central portion of meatus avascular.
• Lateral wall adjacent to palate – Greater palatine artery
• Anteriorly – Facial artery branch (ICA)
• Sup. Lateral wall – Ethmoidal artery (ICA)
• Overlap btw ICA & ECA, complicate while ligation in case of epistaxis
83.
Venous Drainage
• Cavernousplexus in lamina propria
on inf & middle turbinate, controlled
autonomically
• Veins –btw 0.1 & 0.5 mm wide &
anastomose with each other
• Venous drainage :-
Sphenopalatine veins via facial &
opthalmic vessels
Vein on dura via ethmoidal veins
Sup Sagittal sinus via foramen
caecum
84.
Nerve supply oflateral wall
• Sup concha – Olfactory supply
• Anterosup – Ant Ethmoidal nerve
• Post – Branch of Pterygopalatine ganglion & Ant palatine nerves
• Ant small area – Infraorbital nerve
• Area of overlap – Ethmoid & Maxillary N
• Ant inferior Meatus – small branch from ant sup alveolar nerve
85.
Lymphatic Drainage
• Anteriorly:With external nose to
submandibular nodes
• Posteriorly : lateral pharyngeal,
retropharyngeal & upper deep cervical
Secretion in maxillarysinus
• mucous is transported along ant, medial, post & lateral walls as
well as roof & finally converge at ostia,
which open into ethmoidal infundibulam, which opens into middle
meatus via hiatus semilunaris, which is transported over the medial
face of inf. Turbinate post. into nasopharynx
• Secretions from sinus is always transported via natural ostium.
88.
Secretion transport infrontal sinus
• Along interfrontal septum, then laterally along roof & back medially
via floor & inf portions of post & ant wall of sinus
• Secretion exit via lateral aspect of ostia
• After exit – frontal recess (collect secretion from lateral sinus, agger
nasi, pneumatised middle turbinate & ant ethmoidal cells)
• Drain either :directly to infundibulam, or medial to infundibulam
• Secretion from frontal sinus merge with maxillary sinus secretions &
transported to nasopharynx
89.
Secretion transport fromant & post ethmoidal & sphenoidal sinus
cells anteroinf to ground lamella drain to middle meatus
cells opening post & sup are post ethmoidal & drain via superior
meatus into sphenoethmoidal recess
supreme or fourth turbinate – drain into sphenoethmoidal recess
Secretion transport in lateral wall of nose
Two route :
1st
- frontal, maxillary & ant ethmoidal complex,after it reach
nasopharynx;secretion pass ant & inf to eustachian tube orifice
(active transport upto borderline of ciliated & squamous epithelium
in nasopharynx)
90.
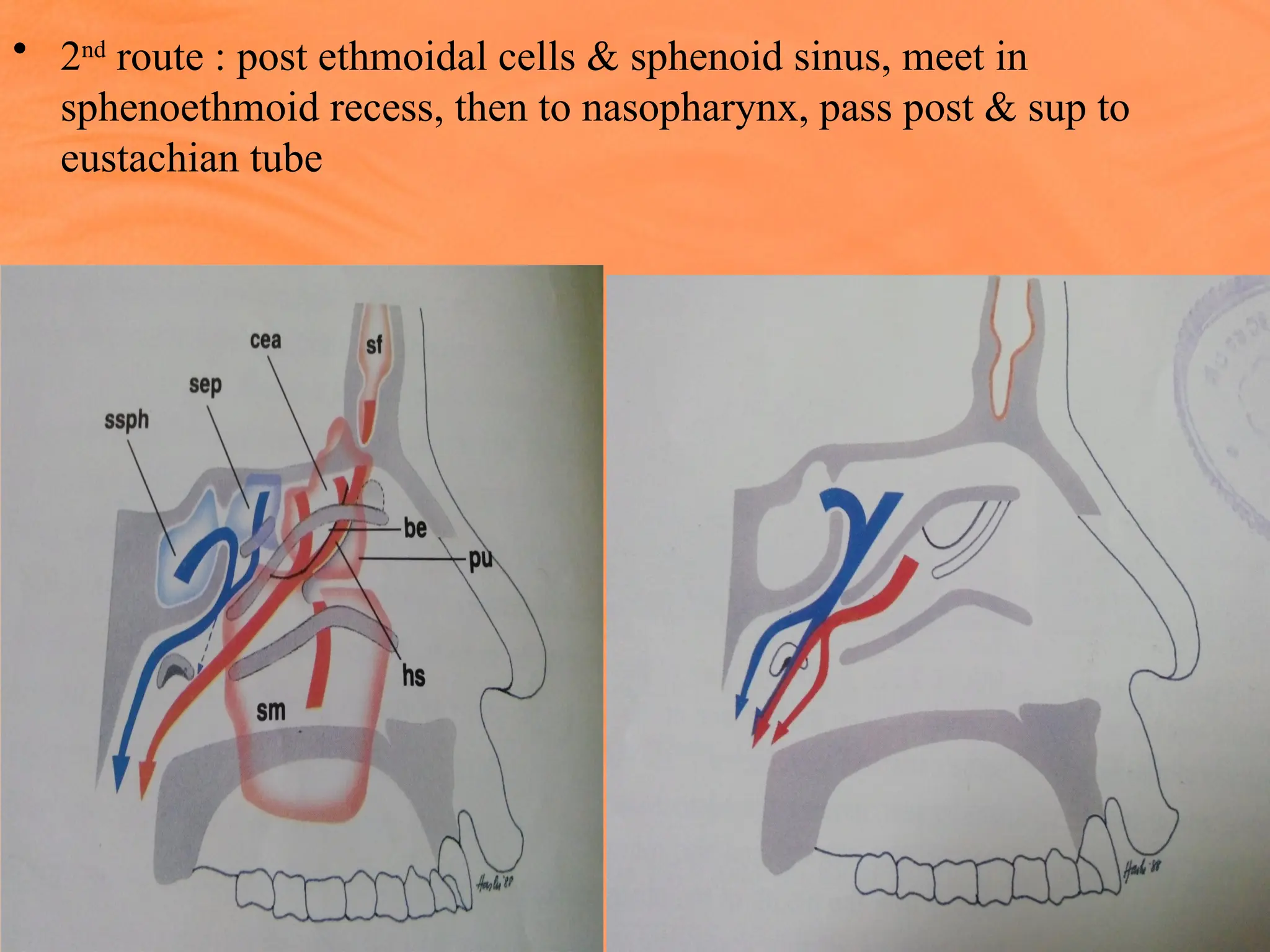
• 2nd
route :post ethmoidal cells & sphenoid sinus, meet in
sphenoethmoid recess, then to nasopharynx, pass post & sup to
eustachian tube
92.
Reference
• Essentials offunctional endoscopic sinus
surgery-Heinz Stammberger, Micheal Hawke
• Scott-brown’s Otorhinolaryngology, Head and
Neck Surgery vol 2
• Anatomical principles of endoscopic sinus
surgery: a step by step approach- Renuka
Bradoo
• Paediatric otolaryngology- Bluestone-vol 2
• Rhinology Journal- supplement 24
• Various Websites
93.
case presentation-A unit
drsantosh kumar
moderator- A unit staff
Case presentation- B unit
Dr Tarakeshwari
moderator-B unit staff
• Seminar presentation
• Topic-ANATOY OF FRONTAL SINUS
& ITS DRAINAGE PATHWAY
• Presentor-Dr Mohan
• Moderator-Dr Abilash
Journal presentation-A unit
Dr Hiran
Moderator- Dr Abilash sir
Journal presentation-B unit
Dr Snehalatha
Moderator – Dr srilaxmi mam










![• Cribriform plate shows a horizontal medial
lamella & oblique / vertical lateral lamella.
• Lateral lamella articulates with the frontal bone
forms - Ethmoid fovea
[medially by the lateral lamella of the
cribriform plate & laterally by the frontal bone]
• Frontal bone - ethmoid fovea - 0.5 mm thick
lateral lamella of the cribriform plate -0 .2 mm.
• The region where the anterior ethmoidal artery
pierces the dura medially is the thinnest area in
the base skull -0.05 mm thick.](https://image.slidesharecdn.com/anatomyofnose-250410181913-056aba62/75/ANATOMY-of-NOSE-power-point-presentation-15-2048.jpg)































![Kennedy’s Nipple [Ant Ethmoidal Foramen]](https://image.slidesharecdn.com/anatomyofnose-250410181913-056aba62/75/ANATOMY-of-NOSE-power-point-presentation-74-2048.jpg)