Downloaded 18 times
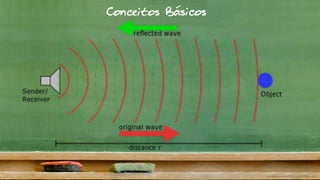
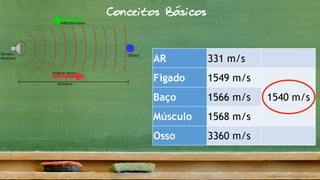
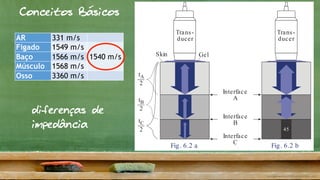
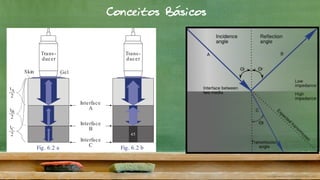
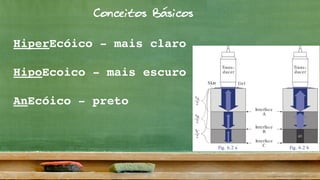
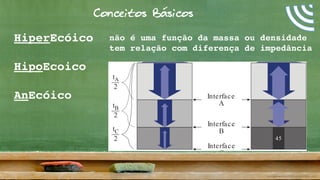
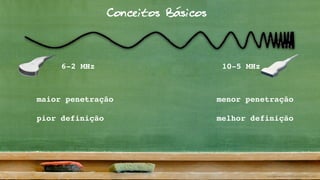

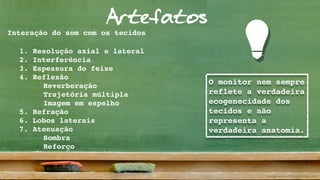
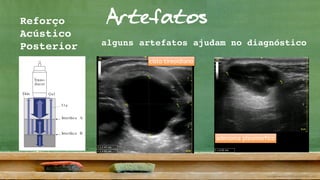


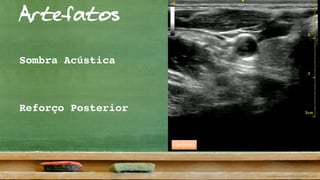
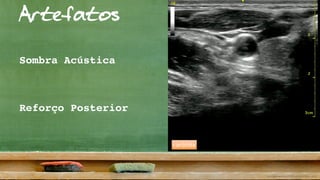

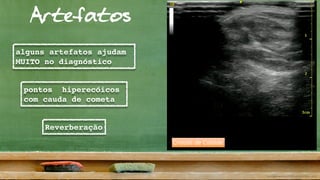
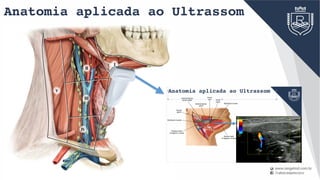


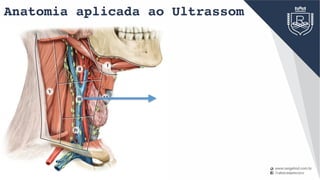




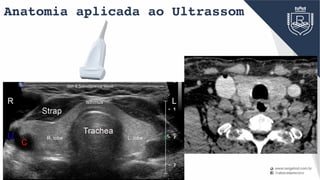
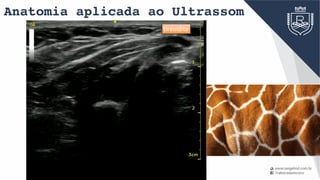
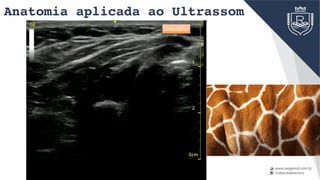
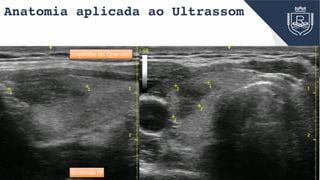




This document provides a summary of an ultrasound principles and head and neck anatomy course. It begins with some basic concepts of ultrasound including how sound waves propagate through different tissues at different speeds, how impedance mismatches cause reflections, and factors that determine image brightness. It then covers artifacts that can appear on ultrasound images. Applied head and neck anatomy is discussed next including identification of salivary glands, levels of cervical lymph nodes, and ultrasound of the thyroid gland. Finally, it provides guidance on using ultrasound to identify enlarged cervical lymph nodes.















































































