Definition
Amniotic Fluid Embolism(AFE)
● is a rare (1:20,000 deliveries) but often lethal
complication (86% mortality rate in some
series) that can occur during labor, delivery,
or cesarean section, or postpartum.
● Anaphylactoid syndrome of pregnancy, an
alternate term used has been suggested to
emphasize the systemic role of chemical
mediators.
3.
Etiology
● AFE isconsidered an unpredictable and unpreventable event with an
unknown cause.
● Reported risk factors for development of AFE include multiparity,
advanced maternal age, male fetus, and trauma.
4.
Epidemiology
● AFE isone of the leading causes of death resulting directly from childbirth,
accounting for 5% to 15% of cases worldwide.
● Incidence of amniotic fluid embolism (AFE) is estimated at 1 case per 8,000-
30,000 pregnancies.
● The true incidence is unknown because of inaccurate diagnoses and
inconsistent reporting of nonfatal cases.
● No racial or ethnic predilection has been thought to exist.
● According to statistics, it is the most common cause of maternal death in
Australia and the second-most common in the USA and the U.K.
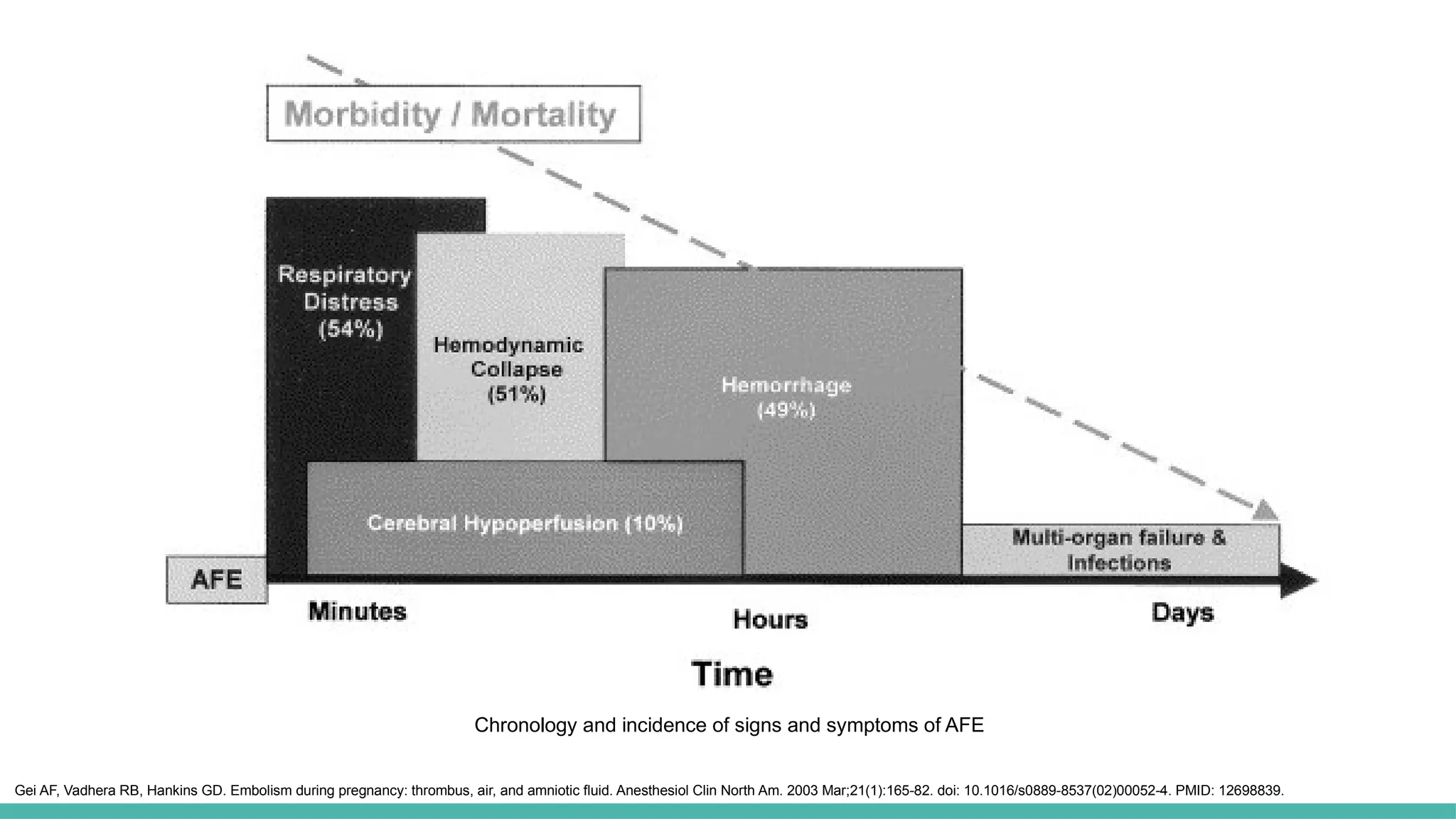
Chronology and incidenceof signs and symptoms of AFE
Gei AF, Vadhera RB, Hankins GD. Embolism during pregnancy: thrombus, air, and amniotic fluid. Anesthesiol Clin North Am. 2003 Mar;21(1):165-82. doi: 10.1016/s0889-8537(02)00052-4. PMID: 12698839.
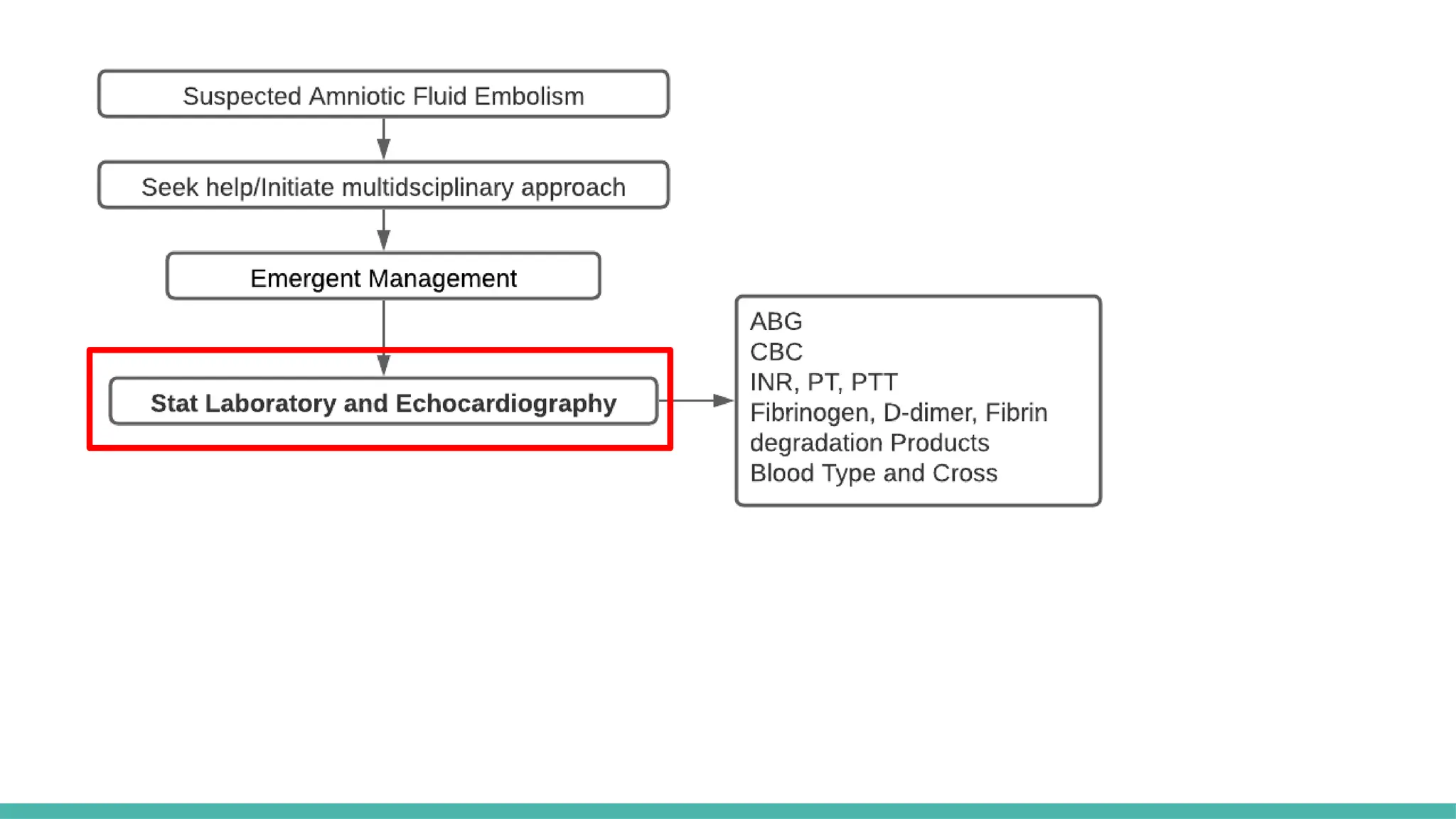
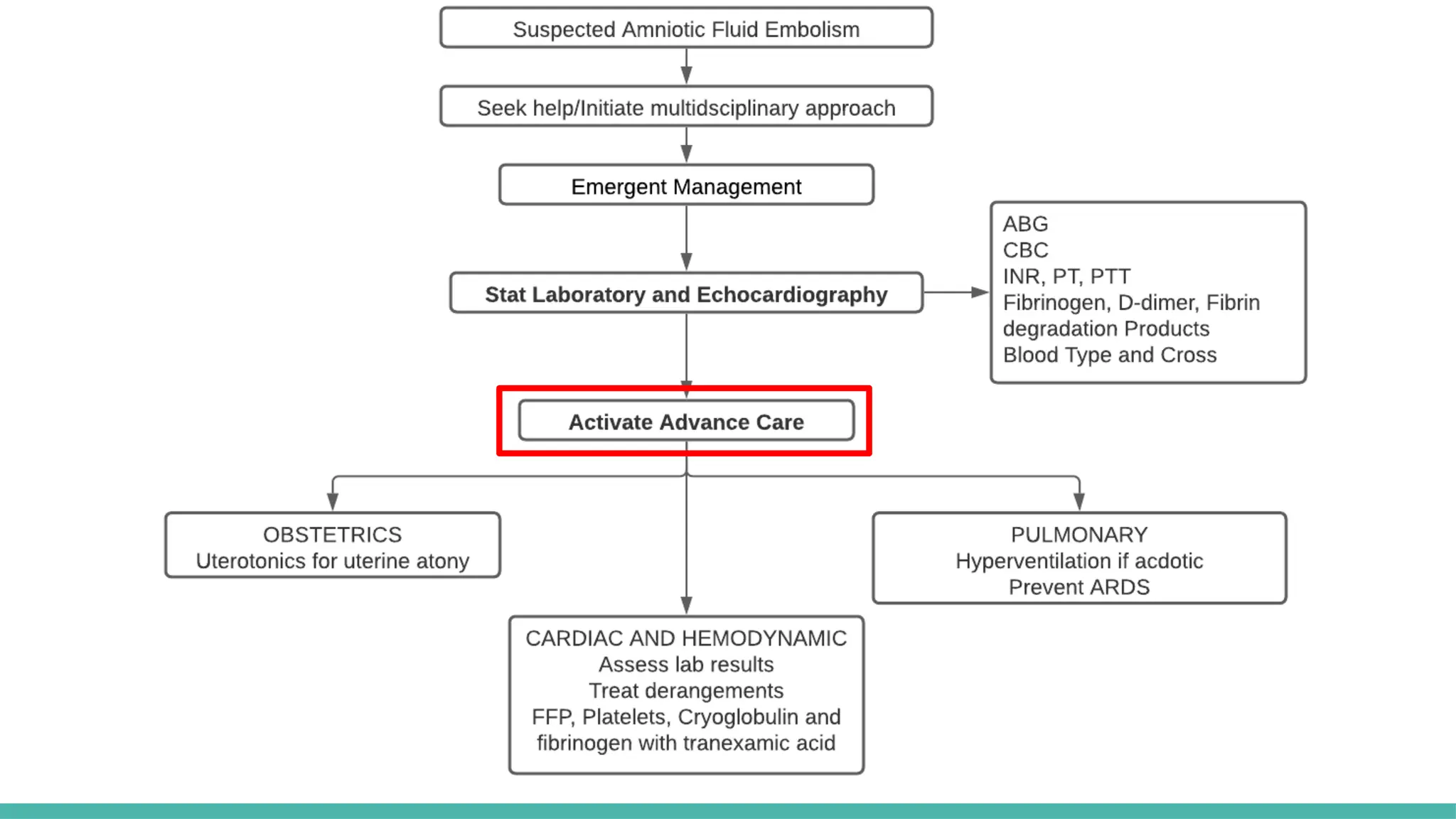
MANAGEMENT:
EMERGENCY MANAGEMENT
● Multidisciplinaryapproach
● Anticipate possible cardiorespiratory arrest and emergent C-section
● Airway Management and hemodynamic support
● Perform CPR as indicated, Do High Quality CPR
● Control Hemorrhage & Reverse Coagulopathy:
○ Tranexamic Acid (TXA)
○ Institute Massive Transfusion Protocol
● Monitoring: EKG, SpO2, EtCO2 , Urine Output
24.
MANAGEMENT: Airway andbreathing
● Prepare for need for emergent intubation
● Give 100% O2, high-flow
● Maintain an arterial PO2 > 60 mm Hg (or O2 Sat of 90% and above)
25.
MANAGEMENT: Hemodynamic Instability
●Establish large volume IV Access
● Support circulation with IV fluid, vasopressors and inotropes
● Anticipate massive hemorrhage and DIC
● Maintaining systolic blood pressure ≥ 90 mm Hg, or MAP ≥65 mmHg ,
and acceptable peripheral organ perfusion (urine output ≥ 25
mL/hour)
● Consider transfer to intensive care unit
Rezai et al.(2017). Atypical Amniotic Fluid Embolism Managed with a Novel Therapeutic Regimen. Case Rep Obstet Gynecol.
31.
Limitations
● Limited casestudies
● Inaccurate diagnosis and inconsistent reporting
● No confirmatory laboratory tests
● Difficulty of obtaining human evidence
● Little value from animal studies
32.
Morgan, G. E.,Mikhail, M. S., & Murray, M. J. (2006). Clinical anesthesiology. New York: Lange Medical Books/McGraw Hill Medical
Pub. Division.
Cunningham, F. G., et . al. (2014). Williams obstetrics (24th edition.). New York: McGraw-Hill Education.
Gist, Richard S. MD*
; Stafford, Irene P. MD†
; Leibowitz, Andrew B. MD*
; Beilin, Yaakov MD*‡
Amniotic Fluid Embolism, Anesthesia &
Analgesia: May 2009 - Volume 108 - Issue 5 - p 1599-1602 doi: 10.1213/ane.0b013e31819e43a4
Gei AF, Vadhera RB, Hankins GD. Embolism during pregnancy: thrombus, air, and amniotic fluid. Anesthesiol Clin North Am. 2003
Mar;21(1):165-82. doi: 10.1016/s0889-8537(02)00052-4. PMID: 12698839.
Rezai et al. (2017). Atypical Amniotic Fluid Embolism Managed with a Novel Therapeutic Regimen. Case Rep Obstet Gynecol.
Stanford Anesthesia Emergency Manual (2016)
References:
Editor's Notes
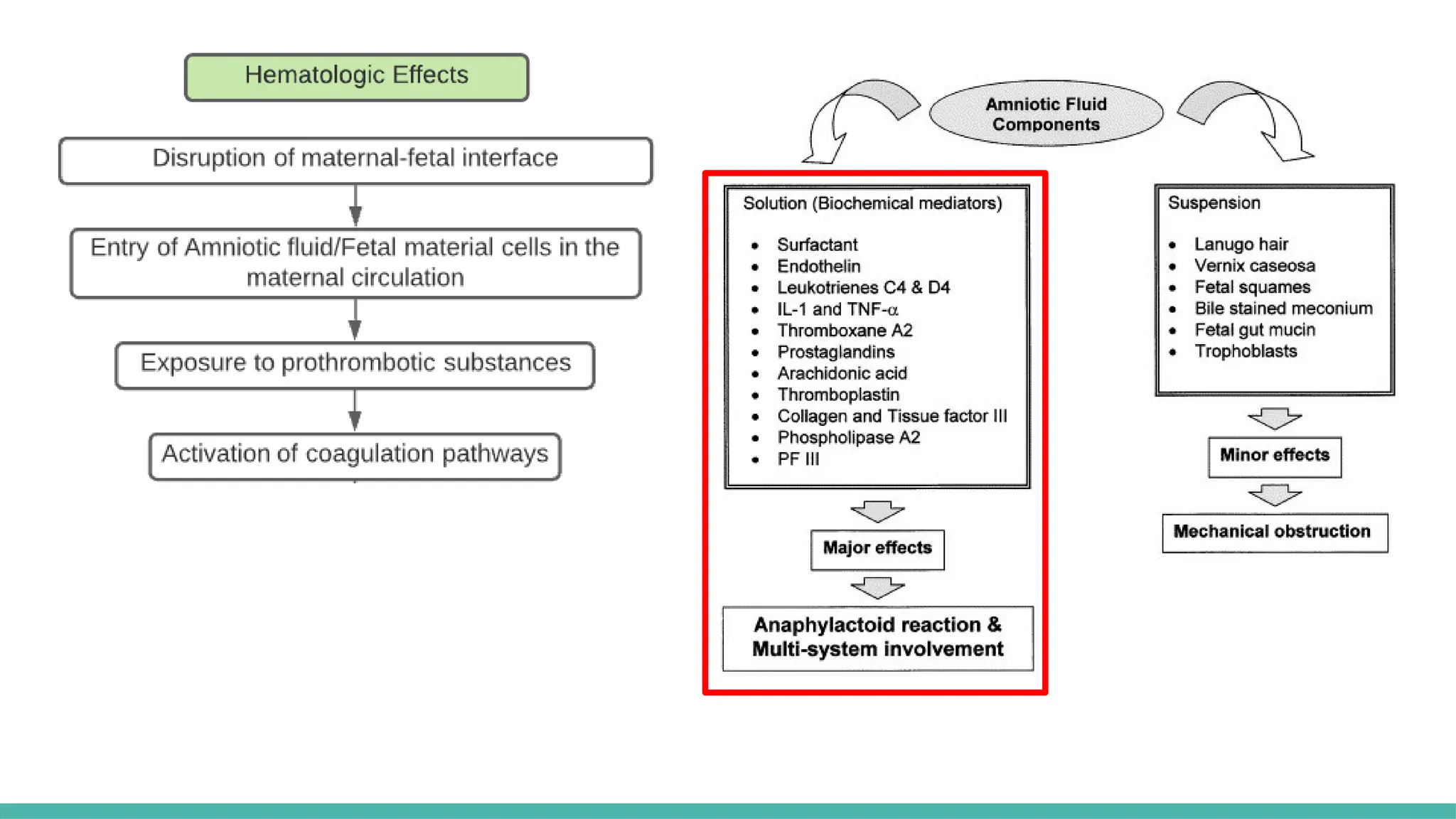
#2 Life threatening obstetric emergency characterized by sudden cardiorespiratory collapse and disseminated intravascular coagulation
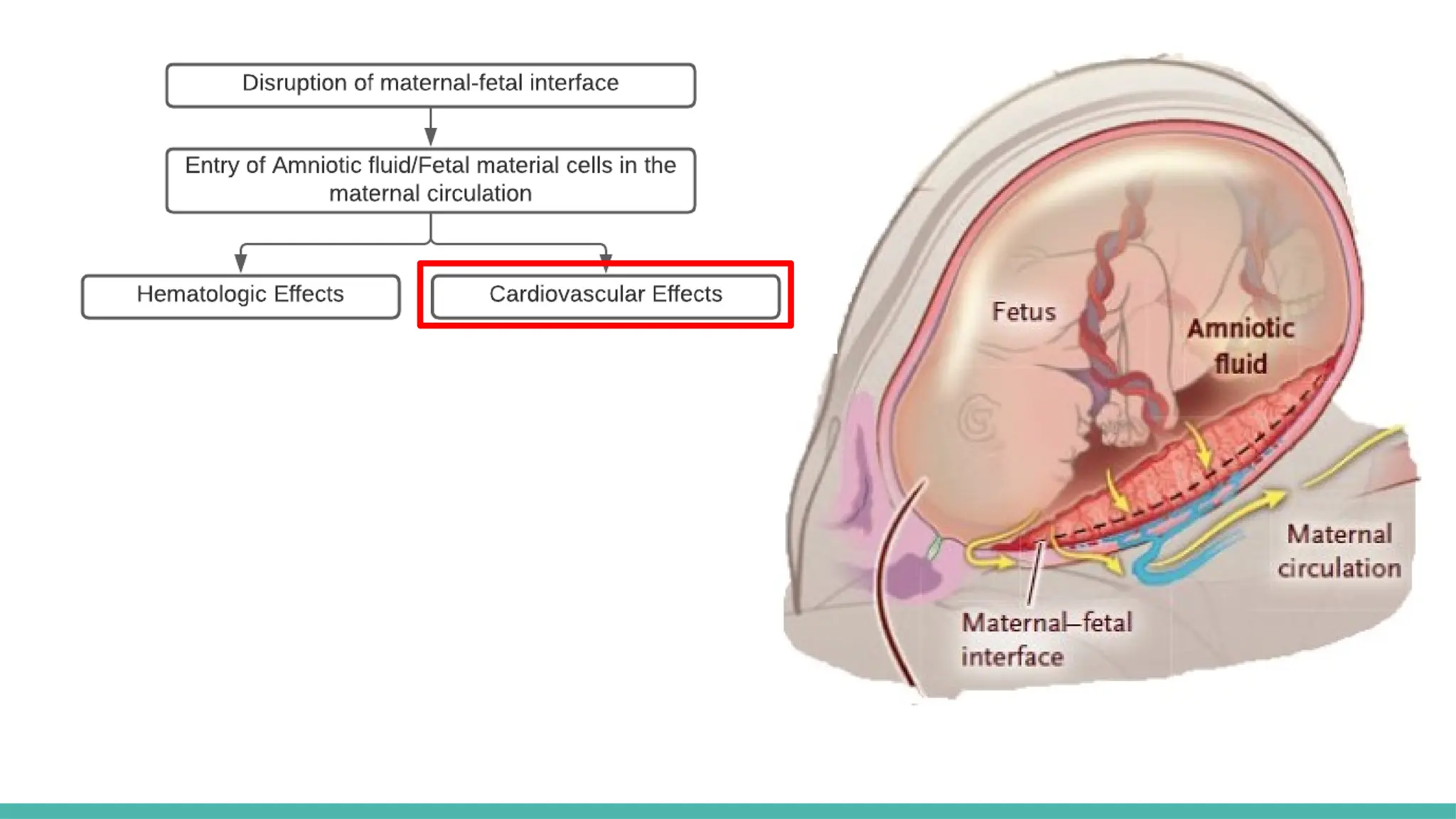
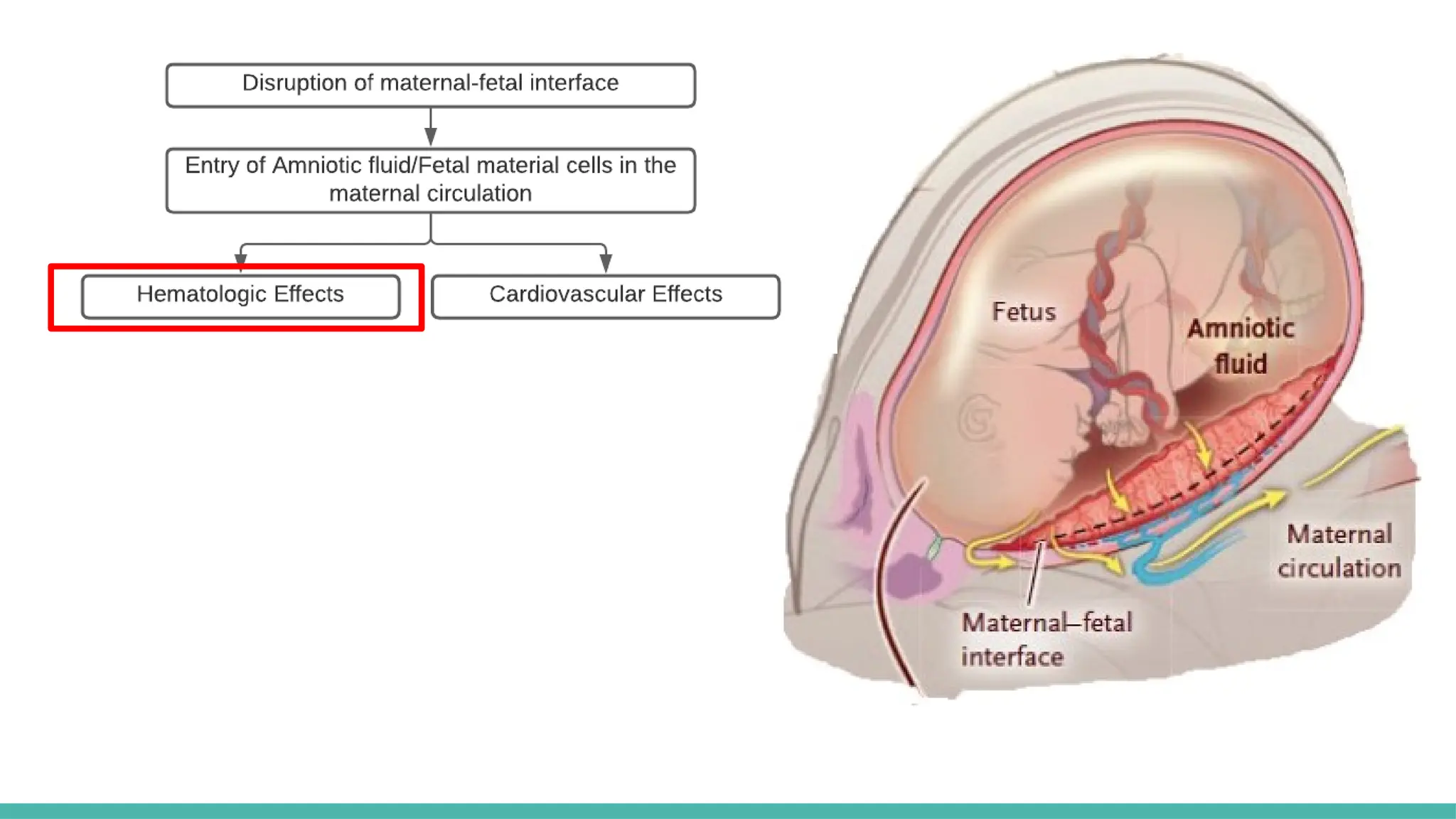
ASP is a rare but serious condition that causes a widespread, proinflammatory, anaphylactic-like reaction after amniotic fluid enters the maternal circulation