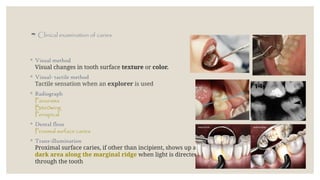
Clinical examinationof caries
◦ Visual method
Visual changes in tooth surface texture or color.
◦ Visual- tactile method
Tactile sensation when an explorer is used
◦ Radiograph
Panorama
Bite0wing
Periapical
◦ Dental floss
Proximal surface caries
◦ Trans-illumination
Proximal surface caries, if other than incipient, shows up as a
dark area along the marginal ridge when light is directed
through the tooth
3.
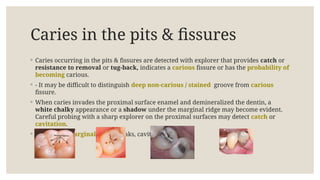
Caries in thepits & fissures
◦ Caries occurring in the pits & fissures are detected with explorer that provides catch or
resistance to removal or tug-back, indicates a carious fissure or has the probability of
becoming carious.
◦ - It may be difficult to distinguish deep non-carious / stained groove from carious
fissure.
◦ When caries invades the proximal surface enamel and demineralized the dentin, a
white chalky appearance or a shadow under the marginal ridge may become evident.
Careful probing with a sharp explorer on the proximal surfaces may detect catch or
cavitation.
◦ - When the marginal ridge breaks, cavitation occurs.
4.
Incipient Caires
◦ IncipientCaires occur mainly in gingival areas that are least accessible to cleaning.
◦ - A white spot that is visually different from the adjacent translucent enamel & will
partially or totally disappear from vision by wetting, while drying again will cause it to
reappear.
◦ This disappearing-reappearing phenomenon distinguishes it from the white spot
resulting from developmental hypocalcification.
◦ - Both types of white spots are undetectable by tactile sensation because the surface is
intact, smooth and hard.
5.
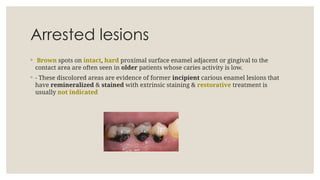
Arrested lesions
◦ Brownspots on intact, hard proximal surface enamel adjacent or gingival to the
contact area are often seen in older patients whose caries activity is low.
◦ - These discolored areas are evidence of former incipient carious enamel lesions that
have remineralized & stained with extrinsic staining & restorative treatment is
usually not indicated
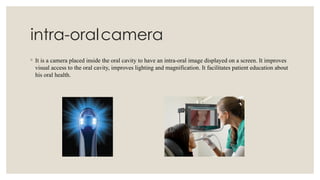
intra-oralcamera
◦ It isa camera placed inside the oral cavity to have an intra-oral image displayed on a screen. It improves
visual access to the oral cavity, improves lighting and magnification. It facilitates patient education about
his oral health.
8.
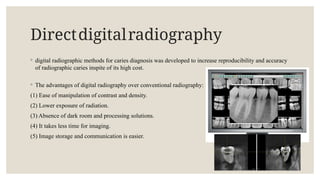
Directdigitalradiography
◦ digital radiographicmethods for caries diagnosis was developed to increase reproducibility and accuracy
of radiographic caries inspite of its high cost.
◦ The advantages of digital radiography over conventional radiography:
(1) Ease of manipulation of contrast and density.
(2) Lower exposure of radiation.
(3) Absence of dark room and processing solutions.
(4) It takes less time for imaging.
(5) Image storage and communication is easier.
9.
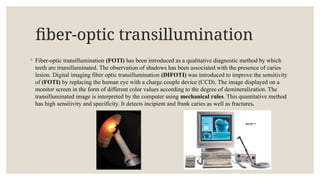
fiber-optic transillumination
◦ Fiber-optictransillumination (FOTI) has been introduced as a qualitative diagnostic method by which
teeth are transilluminated. The observation of shadows has been associated with the presence of caries
lesion. Digital imaging fiber optic transillumination (DIFOTI) was introduced to improve the sensitivity
of (FOTI) by replacing the human eye with a charge couple device (CCD). The image displayed on a
monitor screen in the form of different color values according to the degree of demineralization. The
transilluminated image is interpreted by the computer using mechanical rules. This quantitative method
has high sensitivity and specificity. It detects incipient and frank caries as well as fractures.
10.
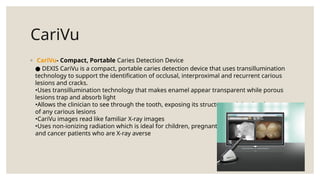
CariVu
◦ CariVu- Compact,Portable Caries Detection Device
DEXIS CariVu is a compact, portable caries detection device that uses transillumination
●
technology to support the identification of occlusal, interproximal and recurrent carious
lesions and cracks.
•Uses transillumination technology that makes enamel appear transparent while porous
lesions trap and absorb light
•Allows the clinician to see through the tooth, exposing its structure and the development
of any carious lesions
•CariVu images read like familiar X-ray images
•Uses non-ionizing radiation which is ideal for children, pregnant women
and cancer patients who are X-ray averse
11.
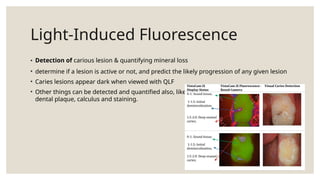
Light-Induced Fluorescence
• Detectionof carious lesion & quantifying mineral loss
• determine if a lesion is active or not, and predict the likely progression of any given lesion
• Caries lesions appear dark when viewed with QLF
• Other things can be detected and quantified also, like
dental plaque, calculus and staining.
12.
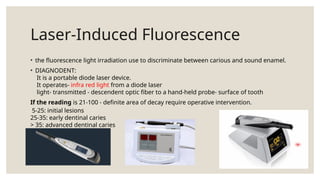
Laser-Induced Fluorescence
• thefluorescence light irradiation use to discriminate between carious and sound enamel.
• DIAGNODENT:
It is a portable diode laser device.
It operates- infra red light from a diode laser
light- transmitted - descendent optic fiber to a hand-held probe- surface of tooth
If the reading is 21-100 - definite area of decay require operative intervention.
5-25: initial lesions
25-35: early dentinal caries
> 35: advanced dentinal caries
13.
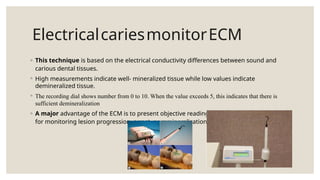
ElectricalcariesmonitorECM
◦ This techniqueis based on the electrical conductivity differences between sound and
carious dental tissues.
◦ High measurements indicate well- mineralized tissue while low values indicate
demineralized tissue.
◦ The recording dial shows number from 0 to 10. When the value exceeds 5, this indicates that there is
sufficient demineralization
◦ A major advantage of the ECM is to present objective readings, which have the potential
for monitoring lesion progression, arrest, or remineralization.
14.
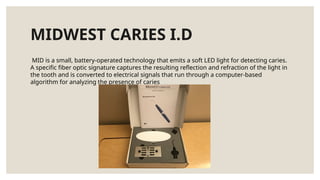
MIDWEST CARIES I.D
MIDis a small, battery-operated technology that emits a soft LED light for detecting caries.
A specific fiber optic signature captures the resulting reflection and refraction of the light in
the tooth and is converted to electrical signals that run through a computer-based
algorithm for analyzing the presence of caries
15.
Ultrasoniccariesdetection
◦ In dentistry,ultrasound has been used to image the tooth and to find caries lesion on smooth surfaces. It
was concluded from this initial study that results showed great promise for ultrasound caries detection for
approximal surfaces.
◦ Diagnosis of carious lesion:
◦ Occlusal surface
◦ Proximal surface
◦ Facial and lingual surfaces
◦ Root surface.









![Methods of Caries Detection[1].pptx by jerry](https://cdn.slidesharecdn.com/ss_thumbnails/methodsofcariesdetection1-250906073723-a458b0cd-thumbnail.jpg?width=640&height=640&fit=bounds)





















![CystS in oral pathology dental edu[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cysts1-250430234019-1ab3f067-thumbnail.jpg?width=640&height=640&fit=bounds)
























