1. Does the application of ice at the IV site further reduce burning sensation from IV lidocaine and
propofol induction for endoscopy?
Renu Chhokra, MD, Adil Mohiuddin, MD, Shaul Cohen, MD, Shubhankar Chhokra1, Oren Y
Ambalu, BA, Sahebjit Bhasin and Arpan G Patel, BS Anesthesiology, UMDNJ-Robert Wood Johnson
University Hospital, New Brunswick, NJ, United States, 08901.
INTRODUCTION: Propofol is a common medication used for
anesthesia induction and is frequently associated with a local
burning sensation. IV lidocaine has been shown to attenuate
this sensation.
OBJECTIVE: To determine whether application of ice at the
IV site further reduces burning sensation of IV lidocaine
injection followed by propofol induction.
METHODS: This is a retrospective review of intravenous
induction of deep sedation for GI endoscopy in the endoscopy
suite. Eighty patients were included and allocated in two
groups. Group I patients (n=97) received IV lidocaine followed
by IV propofol for induction. Group II patients (n=65) had an
ice bag applied for 1 minute at the injection site before
administration of IV lidocaine, followed by propofol. Data
collected for comparison included age, height, weight, ASA
physical status, pain score upon injection of propofol (0-10, 10
= utmost severe pain), and total propofol induction dose. A p
value <0.05 is considered as statistically significant. Statistics:
Chi Square test and student’s t test were used. Data are
presented as Mean ± S.D.
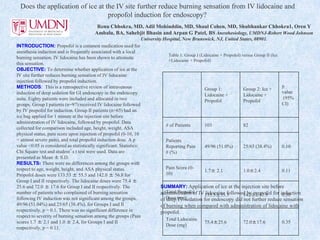
RESULTS: There were no differences among the groups with
respect to age, weight, height, and ASA physical status.
Propofol doses were 133.53 ± 55.5 and 142.0 ± 56.8 for
Group I and II respectively. The lidocaine doses were 75.4 ±
25.6 and 72.0 ± 17.6 for Group I and II respectively. The
number of patients who complained of burning sensation
following IV induction was not significant among the groups,
49/96 (51.04%) and 25/65 (38.4%), for Groups I and II
respectively, p = 0.1. There was no significant difference in
respect to severity of burning sensation among the groups (Pain
scores 1.7 ± 2.1 and 1.0 ± 2.4, for Groups I and II
respectively, p = 0.11.
SUMMARY: Application of ice at the injection site before
administration of IV lidocaine followed by propofol for induction
of deep IV sedation for endoscopy did not further reduce sensation
of burning when compared with administration of lidocaine with
propofol.
Group 1:
Lidocaine +
Propofol
Group 2: Ice +
Lidocaine +
Propofol
p
value
(95%
CI)
# of Patients 103 82
Patients
Reporting Pain
# (%)
49/96 (51.0%) 25/65 (38.4%) 0.10
Pain Score (0-
10)
1.7± 2.1 1.0±2.4 0.11
Total Propofol
Dose (mg)
133.5±55.5 142.0±41.9 0.30
Total Lidocaine
Dose (mg)
75.4±25.6 72.0±17.6 0.35
Table 1: Group I (Lidocaine + Propofol) versus Group II (Ice
+Lidocaine + Propofol)
2. Dog Bite Throat Trauma Causing Distortion of Airway Anatomy,
Misplacement of Endotracheal Tube, and Emergency Tracheostomy
Case Presentation: A 51 y/o female was brought into our trauma bay with multiple lacerations to the face/throat/chest and avulsions to the scalp after
being mauled by a pitbull. PMH & PSH were all unknown. Gauze dressings taped over the throat and chest upon arrival made the anatomy of the injury
difficult to examine. She was moving all extremities with no evidence of cervical spinal injury. An 18g IV was secured to the right hand prior to arrival, and
VS were: BP 149/72, P 115, R 30, O2 sat. 96% on 5L O2 NC. She was alert and followed commands but had hoarseness and difficulty speaking. The
decision was made to intubate her in the trauma bay due to respiratory difficulty. She was preoxygenated with 100% O2 and induced with rapid sequence
technique. Etomidate 20 mg and succinylcholine 120 mg IV were administered while cricoid pressure was applied. The patient’s airway was secured with
a 7.0 ETT passed through the vocal cords with the aid of a Glidescope. In the process of checking bilateral breath sounds and monitoring ETCO2, there
was obvious crepitus and air was seeping through numerous wounds in the throat. Blood-soaked dressings were immediately removed from her neck and
chest of patient and the ETT was found sticking outside the throat resting on her chest. The ETT was removed immediately and bag-mask ventilation was
initiated while the trauma surgeon performed an emergent tracheostomy. She was then taken directly to OR for neck wound exploration and tracheostomy
revision. Cefazolin 2 grams IV was given prior to surgical incision. General anesthesia was maintained using O2, N2O and desflurane along with
rocuronium, with intermittent boluses of fentanyl 50 mcg throughout the procedure. Investigation of the throat revealed comminuted fractures of the
proximal trachea and the thyroid cartilage. The thyroid cartilage was also partially avulsed but not devascularized to the point of needing removal. The
cricoid cartilage was also injured with a complete transection of the vagus nerve on the right. The tracheal and thyroid cartilages and neck lacerations were
repaired with revision of tracheostomy. The patient responded well to resuscitation and remained hemodynamically stable through the procedure. The
patient was transported to the PACU and vital signs were within normal range. On POD 1, further tests showed bilateral cerebral infarctions secondary to
traumatic dissection of bilateral common carotid arteries. On POD 5, she returned to the OR for feeding gastrostomy placement, and on POD 11, she was
discharged from the hospital to rehabilitation.
Sahebjit Bhasin, Gina George DO, Sameet Syed MD, Shaul Cohen MD, Niiamon Robertson BS,
Noah Rolleri BS, Michael Ullo BS, Adil Mohiuddin MD, Christine W Hunter MD
Department of Anesthesia, UMDNJ-Robert Wood Johnson Medical School, New Brunswick, NJ
Conclusion: A thorough evaluation of the face and neck after dressing removal and positive pressure ventilation trial with a bag mask should precede
endotracheal intubation of patients with head and neck trauma to ensure an intact airway and avoid possible worsening
of injury with imprudent invasive procedures. Cricoid pressure without visualization of the throat could have distorted its anatomy and enabled the ETT to
emerge out of the throat. Had the dressing been removed before intubation and the tracheal trauma been seen, a fiberoptic intubation guiding the tube past the
tracheal tear could have avoided tracheostomy.
Summary: A 51 year old healthy female was brought into the trauma bay at our emergency room with multiple lacerations to the face/throat/chest and
avulsions to the scalp covered with dressings, after being mauled by a pitbull. The patient was intubated with Glidescope due to respiratory difficulty without a
thorough examination of her injuries. The endotracheal tube penetrated her throat and was found lying on the chest. Its insertion could have caused further
airway trauma. Therefore, we suggest a thorough evaluation of the face and neck after dressing removal with a PPV trial with a bag mask of a patient with
head and neck trauma before attempting endotracheal intubation to evaluate the integrity of the airway and prevent possible worsening of the injury from ET
insertion. Had the dressing been removed before intubation and the tracheal trauma been seen, a fiberoptic intubation guiding the tube past the tracheal tear
could have avoided tracheostomy.
3. SUTURING THE EPIDURAL CATHETER REDUCES THE INCIDENCE OF FAILED
EPIDURAL BLOCK IN OBSTETRIC PATIENT
May A. Fernandez, MD; Shaul Cohen, MD; Adil Mohiuddin, MD; Shruti Shah, MD; Oren Y.
Ambalu, BA; Sahebjit Bhasin, BS., Arpan G. Patel, BS; Tejal Mehta, MD.
UMDNJ-Robert Wood Johnson University Hospital, New Brunswick, NJ
Introduction:
Recommendations for avoiding failed epidural block in obstetric patients
include using a multi-orifice epidural catheter placed at least 4 cm into the
epidural space and taping the epidural catheter with the patient in an
unflexed lateral decubitus or unflexed sitting upright position1 and also taping
the epidural catheter with a transparent adhesive dressing without gauze
swab2. We examined whether suturing the epidural catheter to the skin can
further reduce the incidence of failed epidural block.
Methods:
One thousand three hundred and twenty four ASA physical status I-II parturients
requesting epidural block for labor and delivery or C/S were studied
The epidural space was located at L2-3 or L3-4 using loss of resistance to air
technique and a midline approach with the patient in lateral or sitting flexed position
An 18 guage “Braun” (B. Braun Medical Inc., Bethlehem, PA 18018) closed end tip
catheter was directed 5 cm cephalad and the patient was then asked to unflex her
back
The patients were randomized to one of two groups: GROUP I (660) parturients had
their epidural catheters sutured with 3-0 silk suture at the insertion site and then
looped downward 5 cm
GROUP II (664) parturients had their epidural catheters looped downward 5 cm
without being sutured
Mastisol glue and transparent dressing were then applied
An investigator recorded the patient’s age, height, weight, parity, position for insertion
of catheter, distance of epidural space from skin, and previous history of epidural
block, spinal block, spinal tap, dural puncture or blood patch
Also recorded were incidence of failed epidural block (a properly functioning epidural
block which subsequently failed), catheter dislodgment, blood vessel puncure, dural
puncture, need for catheter readjustment or reinsertion, occurrence of unilateral block,
efficacy of sensory block for C/S, maximum lumbar and sacral sensory block, lowest
Bromage Score (1= complete motor block, 5=no weakness of hip flexion), catheter
position and length of catheter coiled under the skin at time of catheter removal, and
overall satisfaction (0=worst, 10=best)
Results:
Groups did not differ in age, weight, height, parity or previous history, distance of
epidural space from the skin, lowest Bromage Score, maximum sensory level or
efficacy of sensory block for C/S
Overall satisfaction was high in both groups, 9.5+0.9 vs. 9.1+1.1 (p<0.00001) for
Groups I & II respectively
The length of catheter coiled under skin upon removal was 0.7+0.8cm vs. 0.4+0.8cm
(p<0.0001) for Groups I & II respectively
Incidence of catheter movements and resulting complications and corrections are
shown in Tables I & II respectevely
Table I: Catheter Movement Upon Removal
None Outward Inward Dislodged
Group I 528 62 49 0
Group II* 218 229 111 49
*Significantly greater than Group I, p<0.00001
Table II: Incidence Of Complications & Corrections
Failed One-sided Blood Vessel Readjustment Reinsertion
Block Anesthesia Puncture of Catheter of Catheter
Group I 9 6 4 7 5
Group II *43 **34 ***17 **30 ****23
*Sig. greater than Group I, p<0.00001 **Sig. greater than Group I, p<0.00002
***Sig. greater than Group I, p<0.008 ****Sig. greater than Group I, p<0.001
Conclusion:
Suturing the epidural catheter reduced catheter movement and need for
reinsertion, decreased the incidence of one-sided anesthesia and catheter
puncture of epidural vessels, and increased the success rate of epidural block
1. Hamilton et al. Anesthesiology 83:A950, 1995
2. Schmitt et al. Anesth Analg 69:856-7, 1989
References:
4. EPIDURAL ANESTHESIA FOR CESAREAN SECTION IN A PARTURIENT WITH INTRACRANIAL TUMOR.
Heather Skiff DO, Shaul Cohen MD, Shruti Shah MD, Jeremy Grayson MD, Adil Mohiuddin MD, Sahebjit Bhasin,
Renu Chhokra MD.
Department of Anesthesia, UMDNJ-Robert Wood Johnson Medical School, New Brunswick, NJ
Case Report: We would like to report a case of a successful epidural anesthesia for cesarean section in a parturient with intracranial tumor
This 33-year-old white parturient ( Height 165 cm, weight 70 kg) was scheduled for elective cesarean section to be followed two days later by a scheduled elective
craniotomy for removal of left frontal lobe tumor. She was afebrile, BP 110/70. HR 80, had muscle weakness of the right face, arm and leg without trouble swallowing. She
had slight slurred speech, and denied headache or photophobia. Her neurosurgeon reported a normal intracranial pressure without midline shift and preferred an epidural
anesthesia for her cesarean section, which would be, followed two days letter by craniotomy. If the dura was to be punctured accidentally, an immediate epidural blood patch
was recommended. The risks and the benefits of epidural and general anesthesia were explained to the patient and her husband and they preferred epidural anesthesia..
The epidural space was located at L3-4 interspace using 17g Hustead needle in right lateral decubitus position. The stylet was reinserted upon reaching ligamentum
flavum each time the needle was advanced 1-2 mm into the epidural space to reduce the risk of unintentional dural puncture [1]. Following a loss-of resistance to air injection,
3,5,5 and 5 ml 2 % lidocaine with 5mcg/ml epinephrine and 5 mcg/ml fentanyl were administered by gravity technique [2] via 22 inches extension tube into the needle. A 19
gauge Arrow FlexTip Plus® (Arrow International Inc.) open-end tip catheter placed 4 cm in the epidural space and additional 3 ml was administered via the catheter. This
technique provided an excellent bilateral L3-S5 epidural block for an uneventful cesarean section of a healthy but premature female with Apgar scores of 8 and 8. The patient
received 2400 ml of lactated Ringer’s solution, had an estimated blood loss of 800 ml and urine output of 800 ml, and had stable vital signs throughout the operation.
Following an uneventful course in the recovery room she was transferred to the intensive care unit with epidural-PCA ropivacaine 0.025% with fentanyl 3 mcg/ml and
epinephrine1 mcg/ml, 15 ml/hr, 4 ml PCA dose with lockout time of 10 min. The following day she had an episode of seizures, was intubated, connected to a ventilator and the
epidural catheter was removed. The day after she underwent craniotomy with only partial removal of a rapidly growing tumor. In the postoperative period in the surgical ICU
the treatment of her persistently increased intracranial pressure was unsuccessful. Two days after surgery she was declared brain dead and care was subsequently withdrawn.
Summary: There are no guidelines for the optimal time for craniotomy in the pregnant patient with intracranial tumor. Neurosurgery is usually delayed until after delivery.
The clinical course of the tumor and its location determines the indication for surgery. In most cases, pregnancy is allowed to continue under closed observation until the
maturity of the fetus. The use of neuraxial block has been controversial when a parturient was presented for labor and delivery with intracranial mass and increased intracranial
pressure [3]. Intentional dural puncture is relatively contraindicated when intracranial pressure is elevated because of the potential risk of cerebellar pons herniation when CSF
is lost rapidly under increased pressure. Epidural block may further increase the intracranial pressure when a large volume of fluid is administered into the space. Increased
CSF pressure may push the dura against the epidural needle and increase the risk of dural puncture. Case reports on this subject were inconclusive. Several case reports have
shown that in patients with brain tumors with or without increased intracranial pressure, labor and subsequent cesarean delivery have been managed successfully with epidural
blocks if extreme care was taken to avoid inadvertent dural puncture [4-6]. There have been poor outcomes associated with inadvertent dural puncture [7].
In our case, upon insertion of the epidural catheter, there was no clinical evidence of increased intracranial pressure. We still made every effort to reduce the risk of accidental
dural puncture by performing the block in lateral decubitus position, reinserting the stylet upon each advancement of the needle, administering the local anesthetic by gravity
technique and applying Arrow catheter. The aggressive nature of the tumor caused this bad outcome. We suggest that epidural block may still be a viable option for parturients
with intracranial tumors who are admitted for labor and delivery.
References:
1. Cohen S, Sakr A, Groysman R, Bhavsar V, Amar D. Does stylet reinsertion upon reaching ligamentum flavum with an epidural needle reduce the incidence of accidental dural puncture? Anesthesiology 2003;
99:A1161.
2. Cohen S, Amar D. Epidural block for obstetrics: Comparison of bolus injection of local anesthetic with gravity flow technique Clin Anesth 1997; 9:623-628.
3. Chang L, Looi-Lyons L, Bartosik L, Tindal S. Anesthesia for cesarean section in two patients with brain tumours. Can J Anaesth 1999; 46:61-65
4. Goroszeniuk T, Howard RS, Wright JT. The management of labour using continuous lumbar epidural analgesia in a patient with malignant cerebral tumour. Anaesthesia 1986; 41: 1128-1129.
5. Boyd AH, Pigston PE. Postpartum headache and cerebral tumour. Anaesthesia 1992; 47: 450-451.
6. Finfer SR. Management of labour and delivery in patients with intracranial neoplasm. Br J Anaesth 1991; 67: 784-787.
7. Duffy GP. Lumbar puncture in the presence of raised intracranial pressure. BMJ 1969; 1: 407-409.