Download as PDF, PPTX




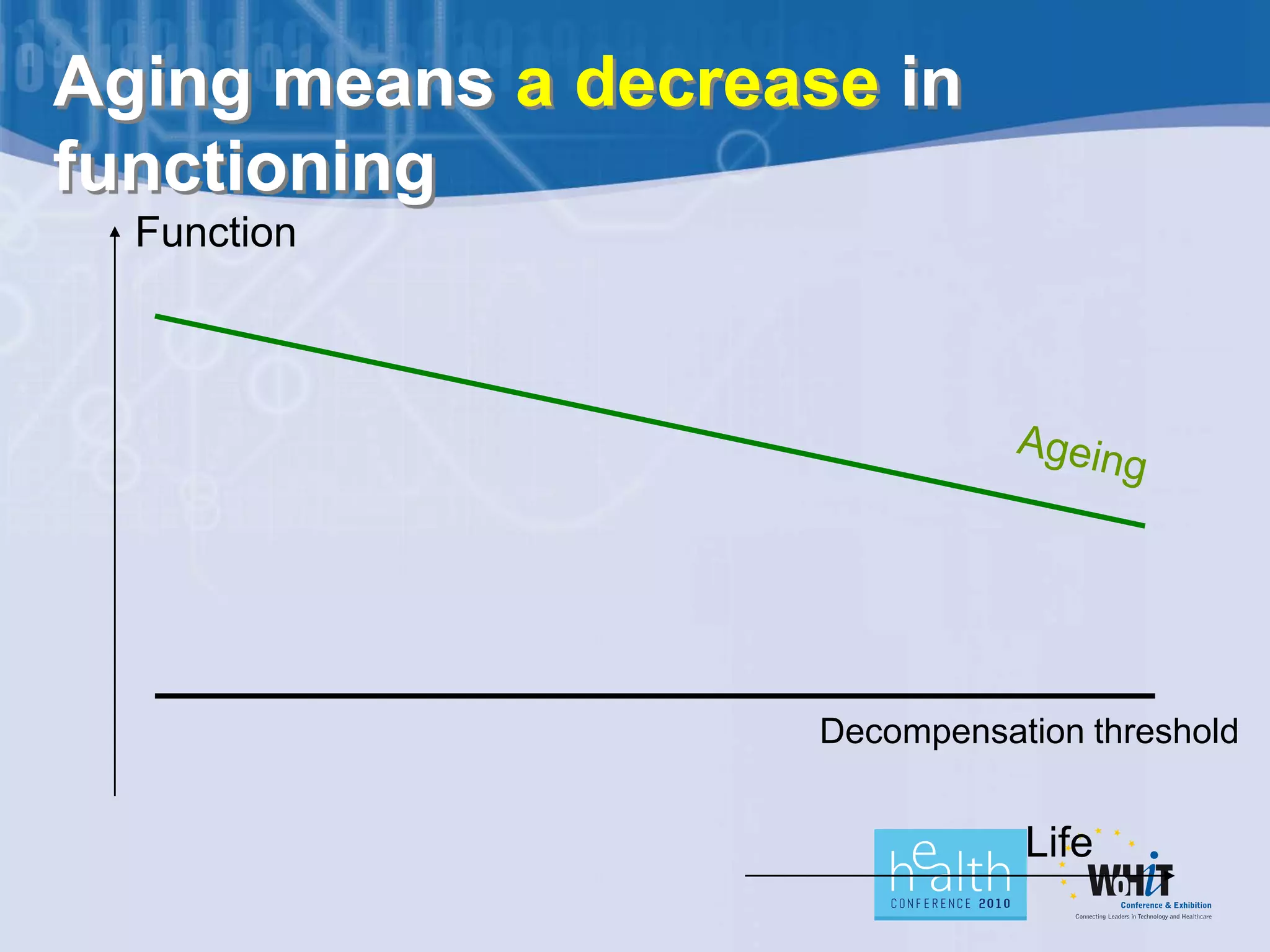
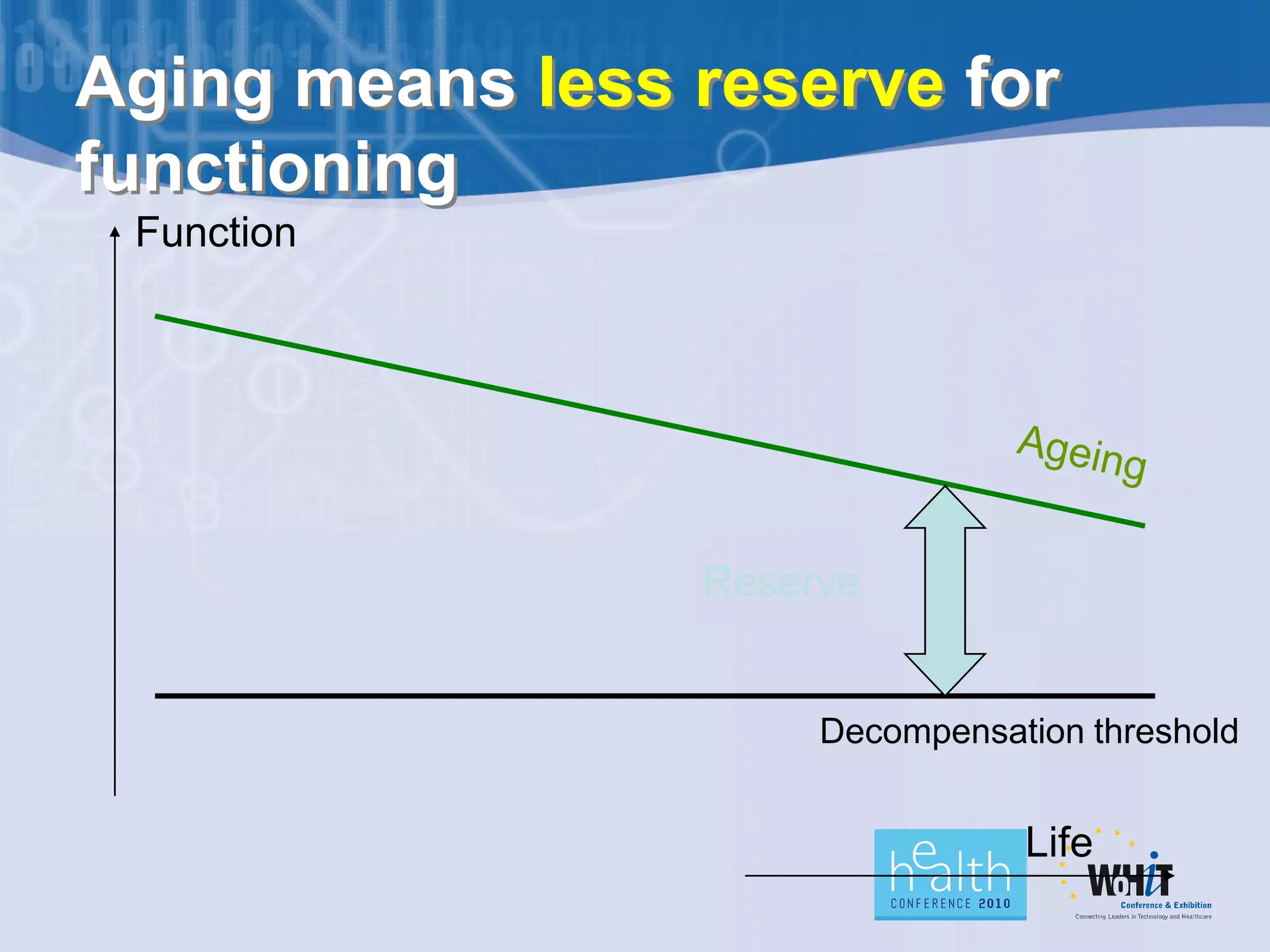
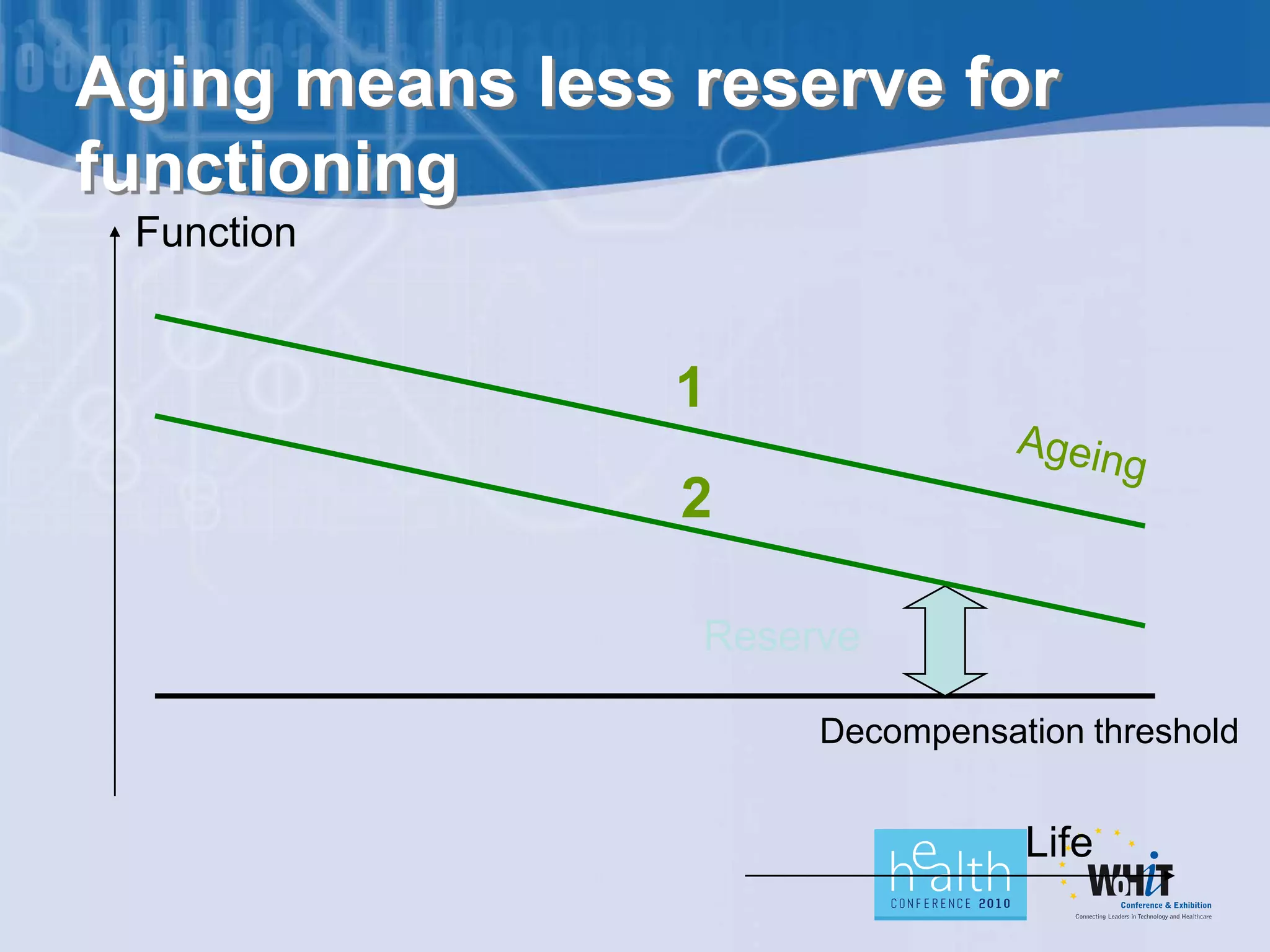
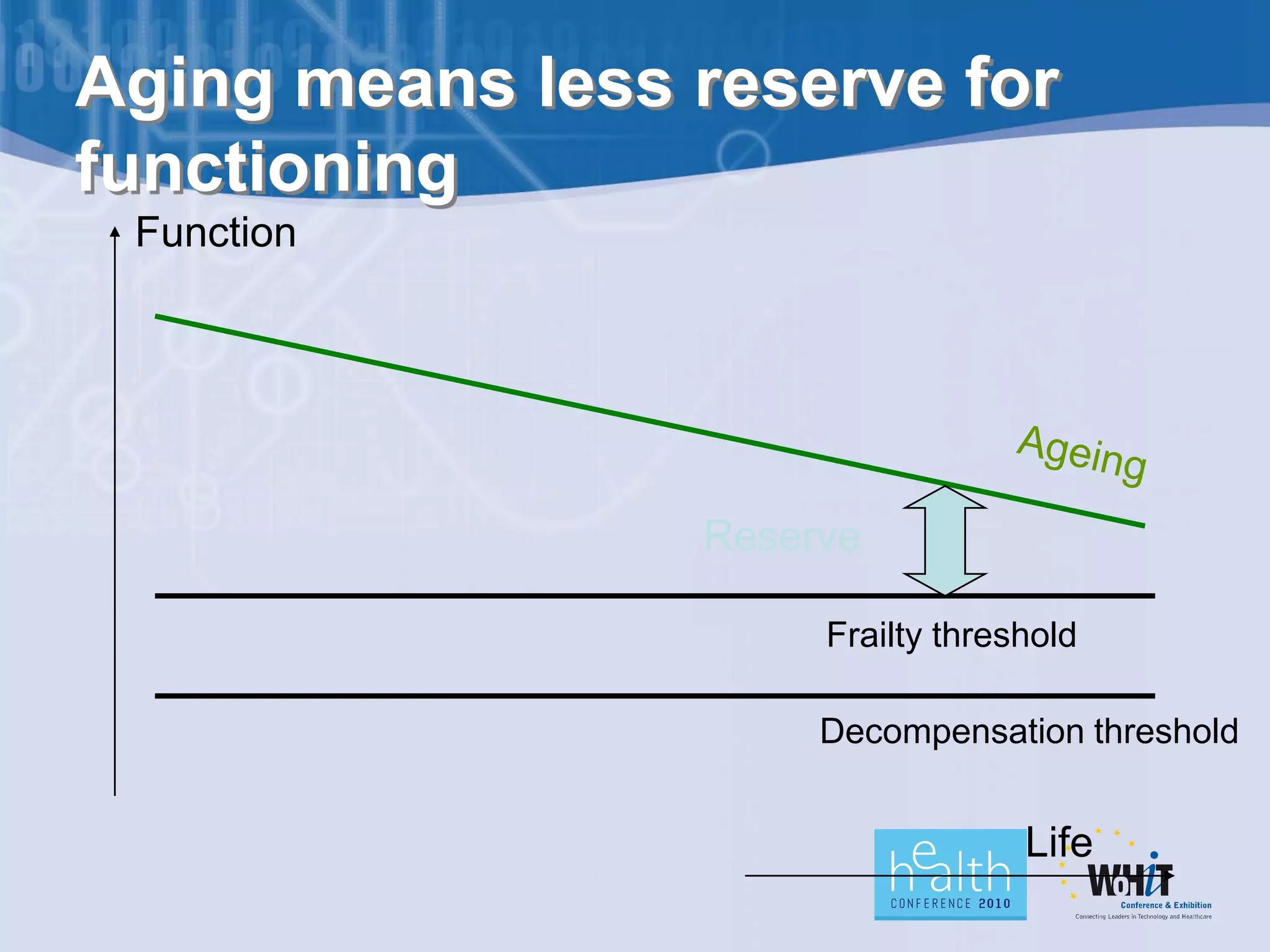
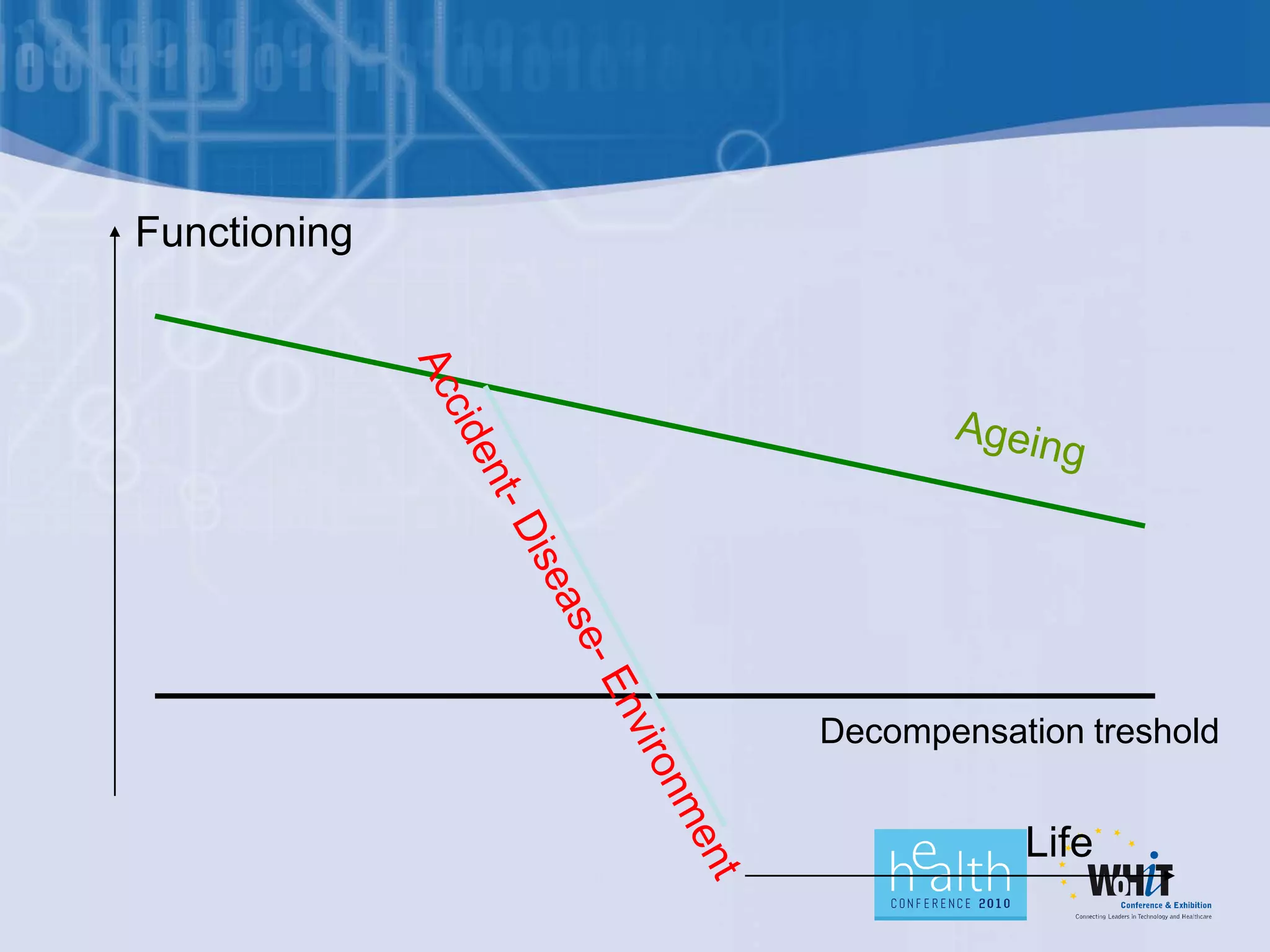
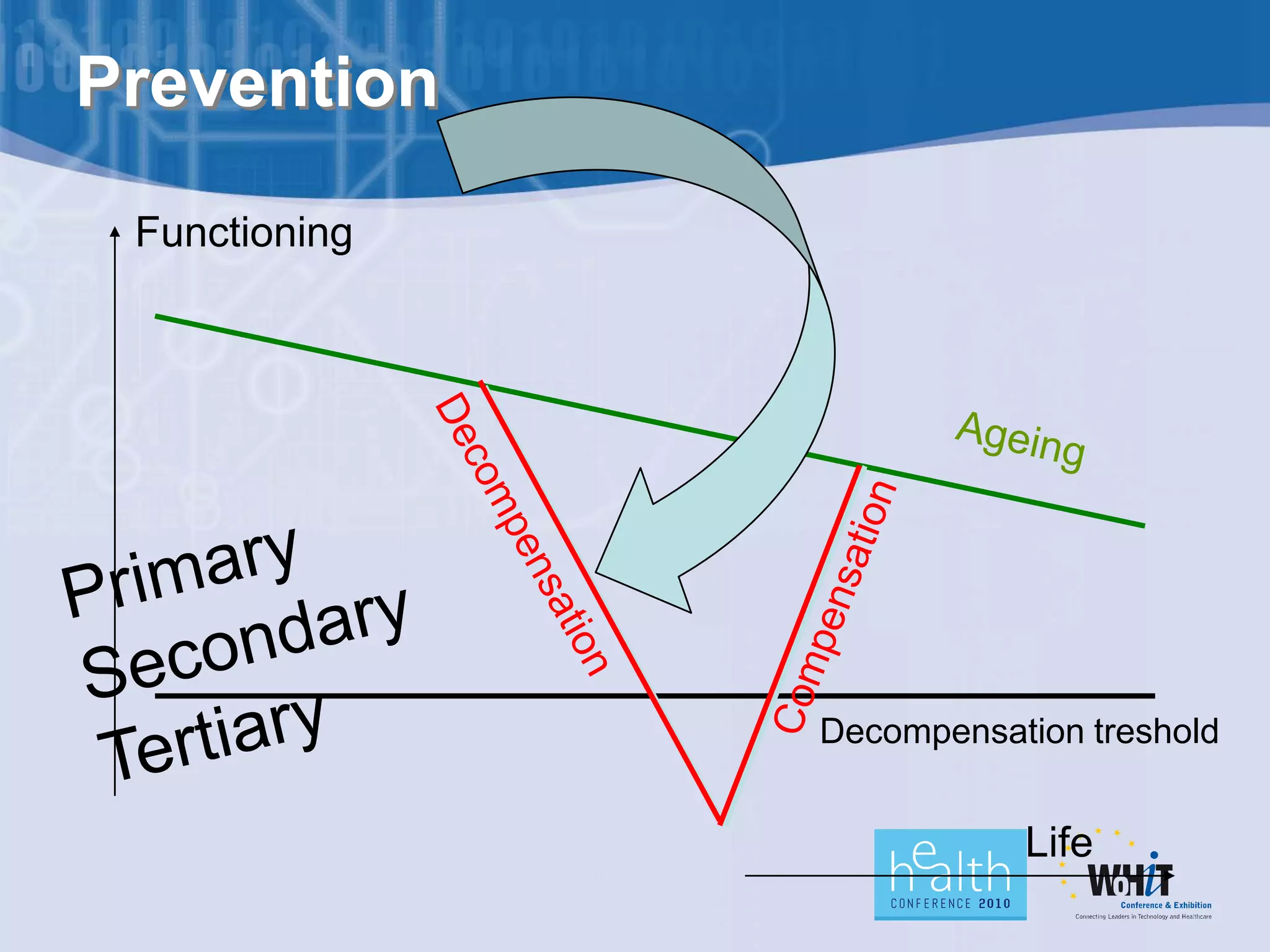
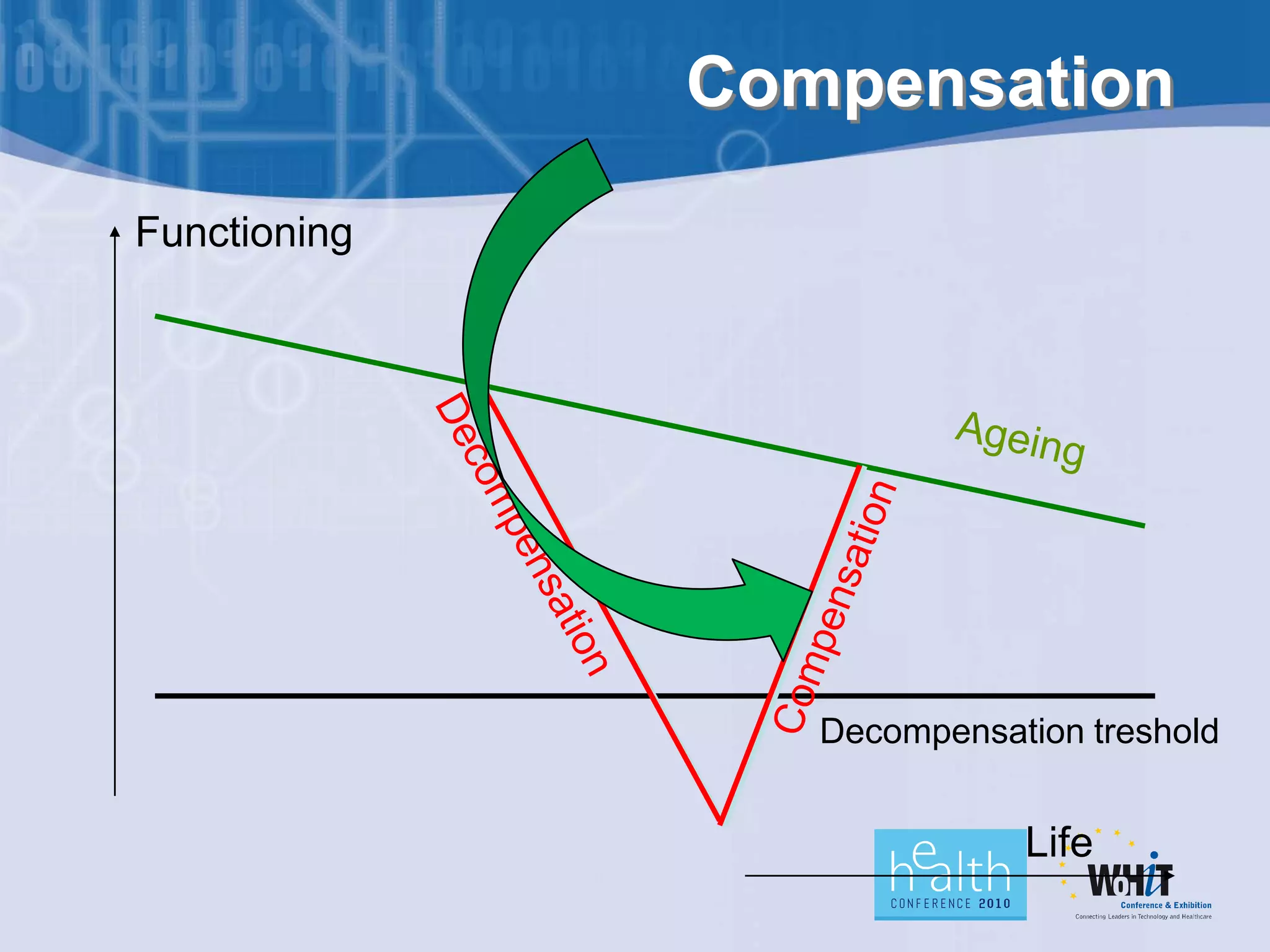
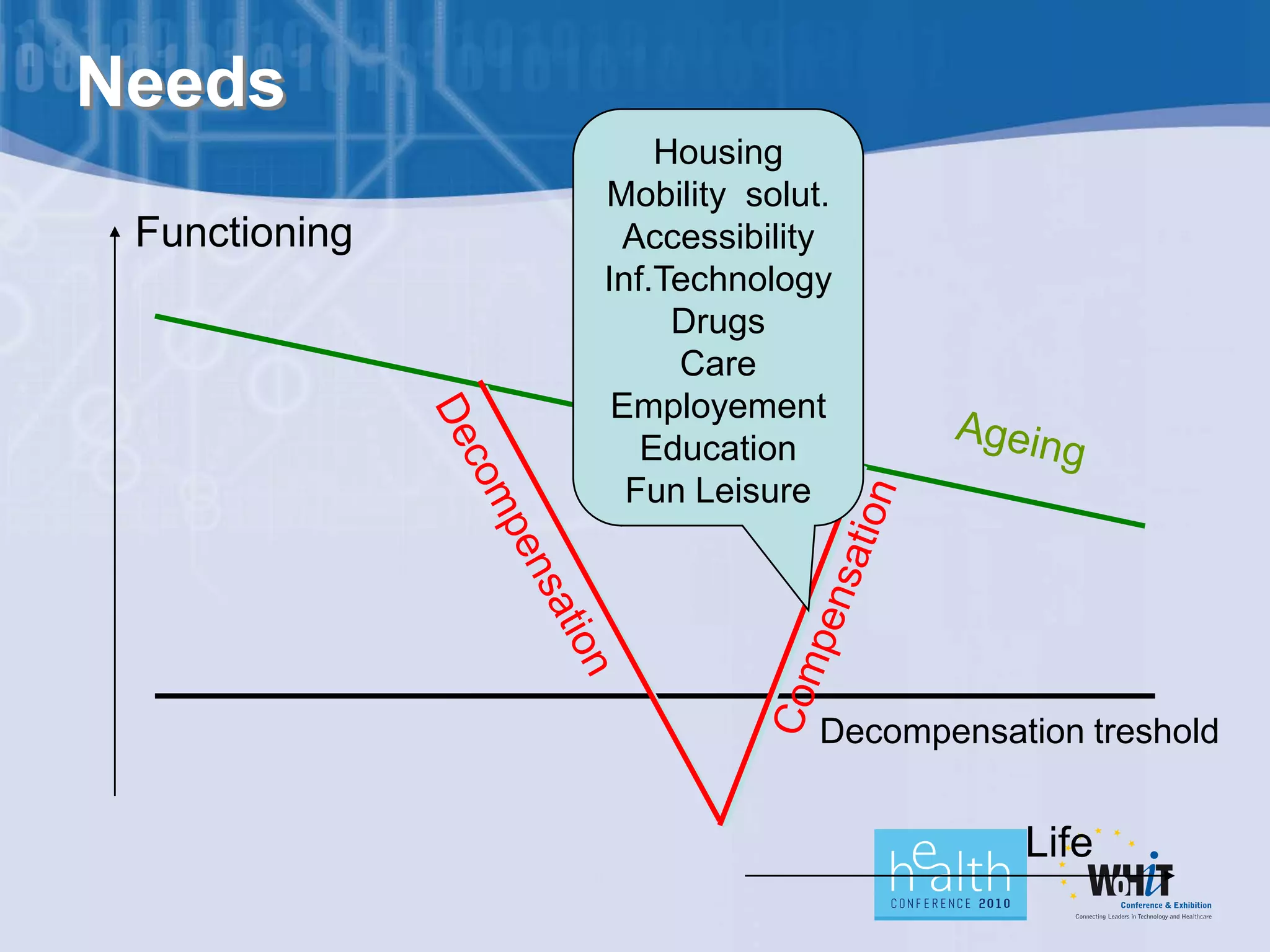
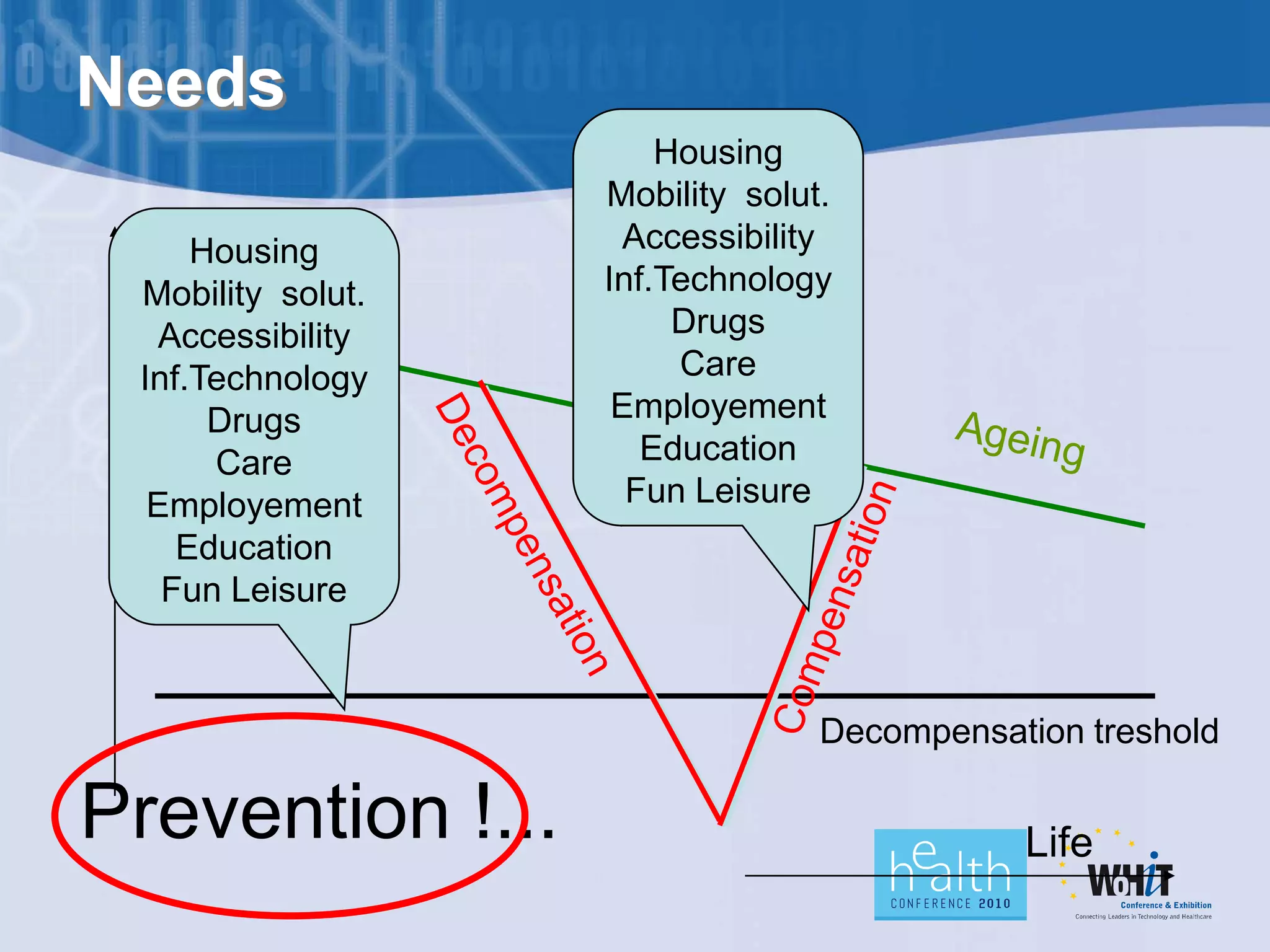
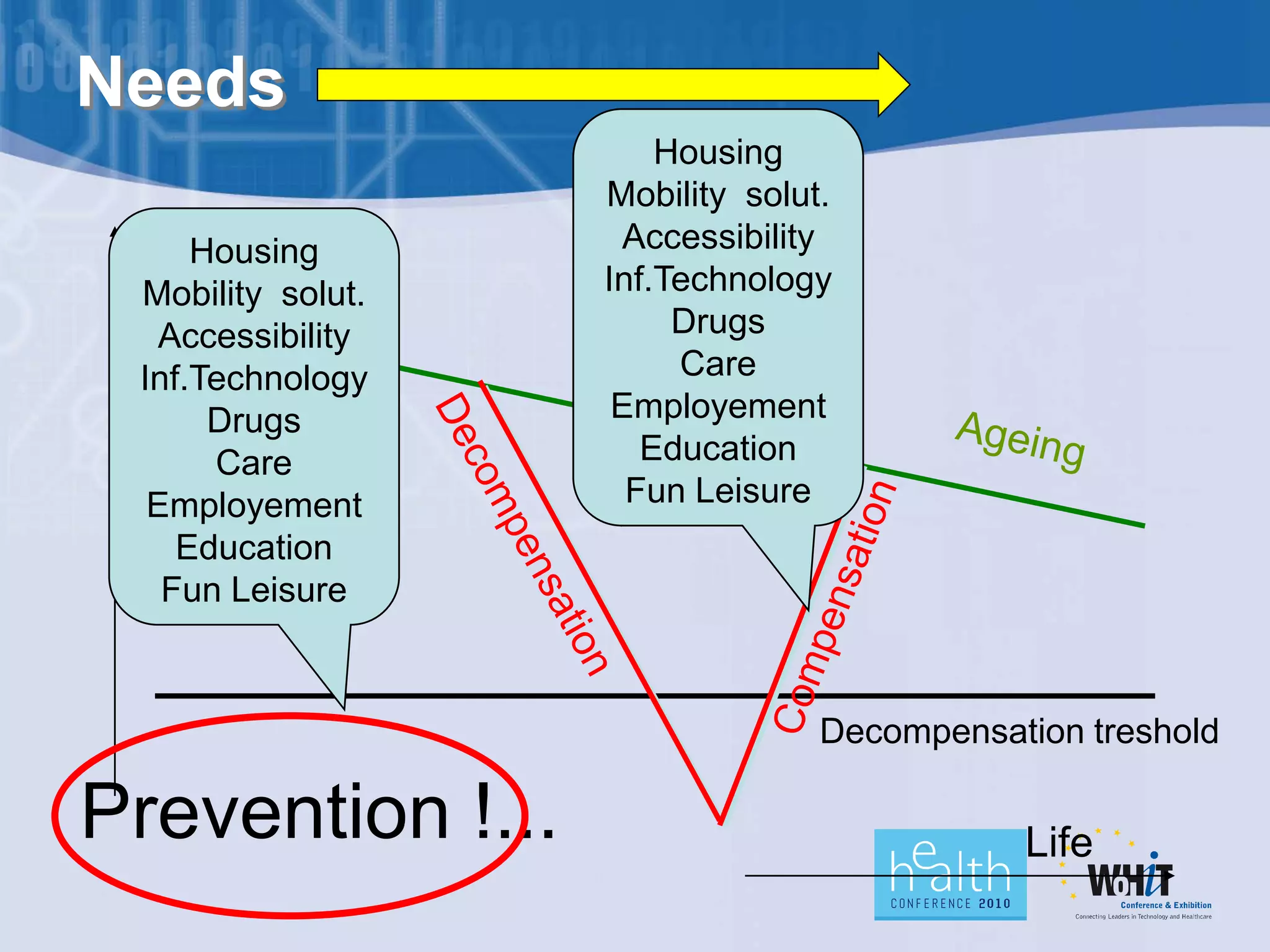
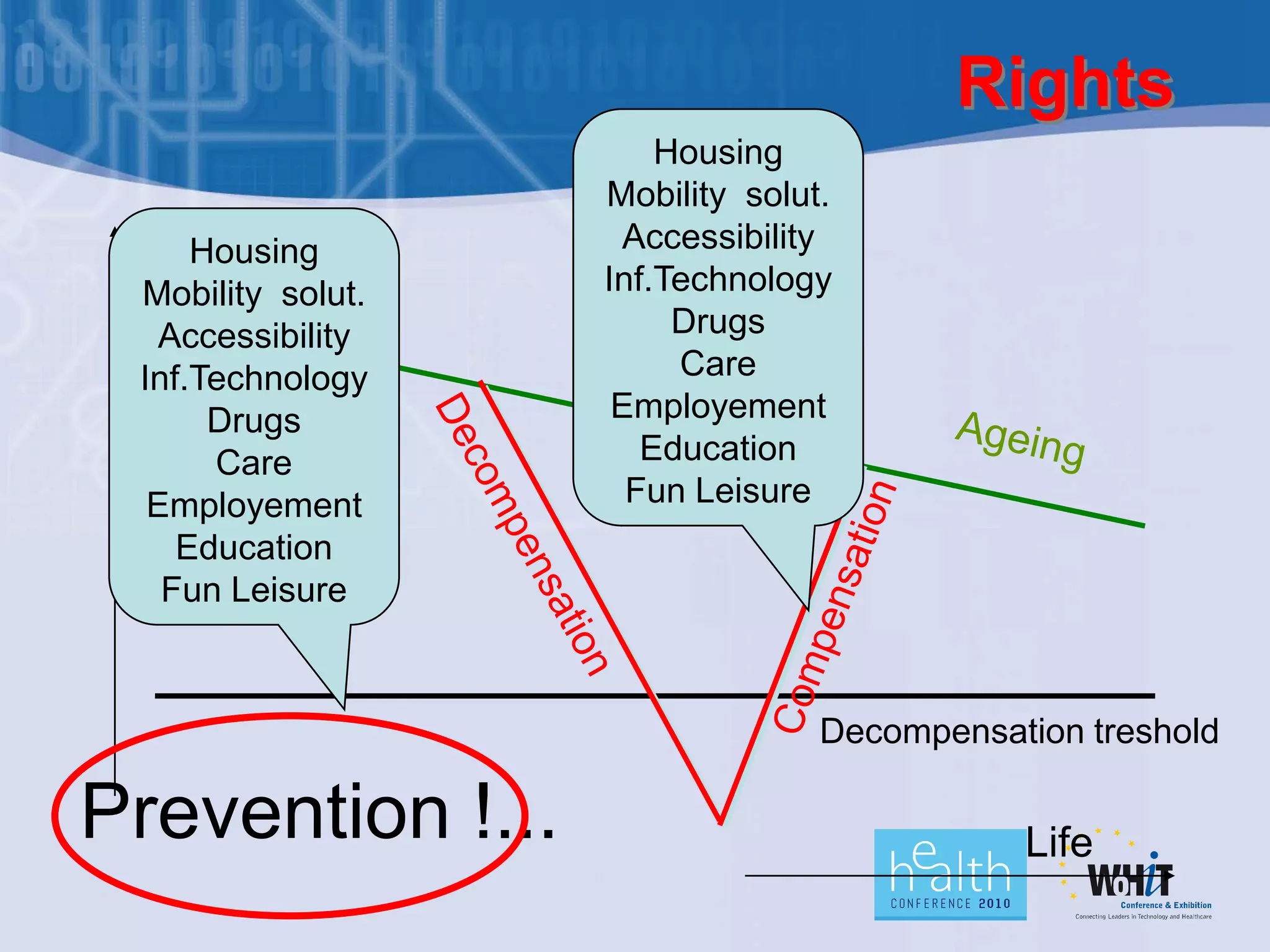
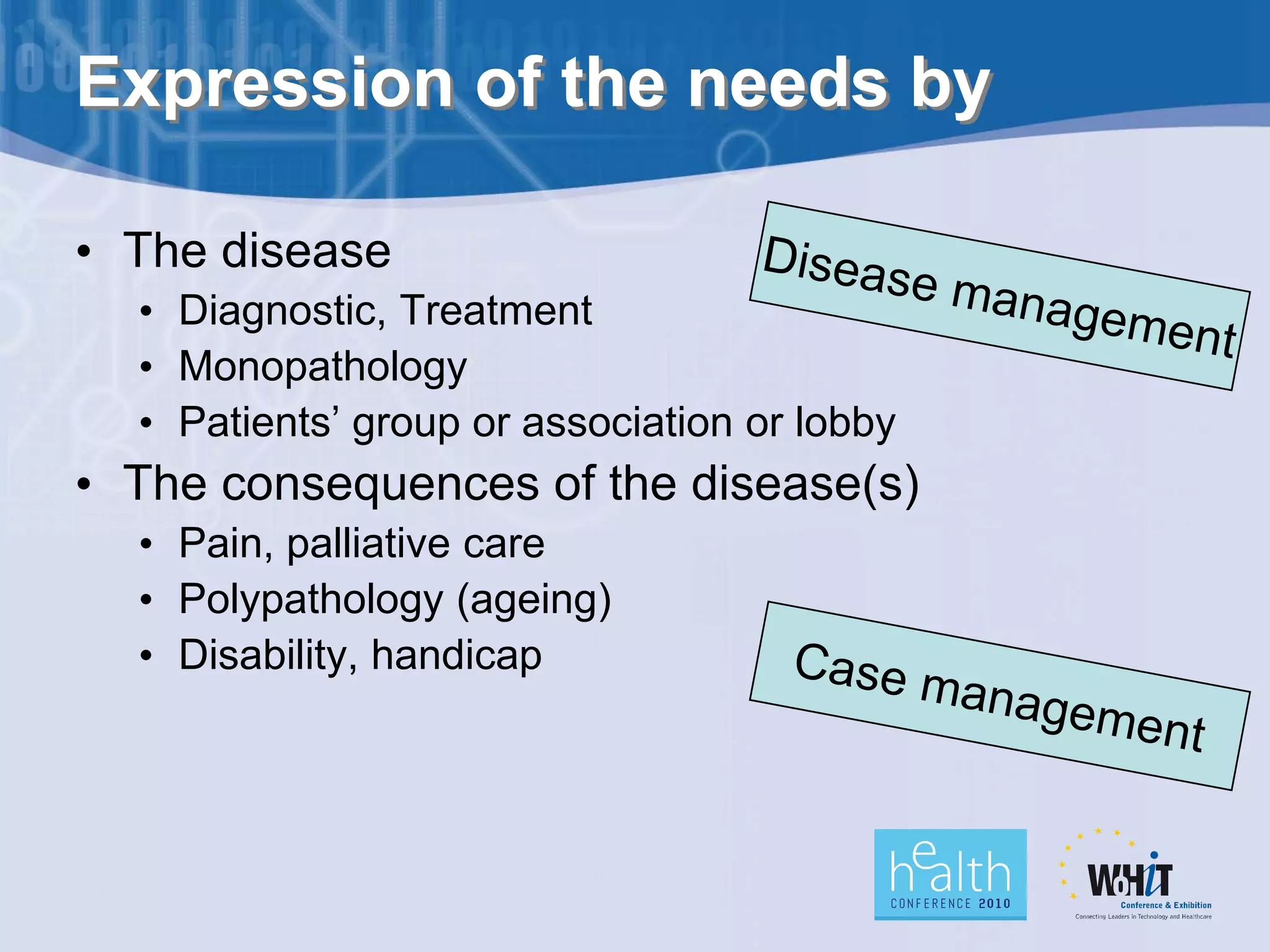
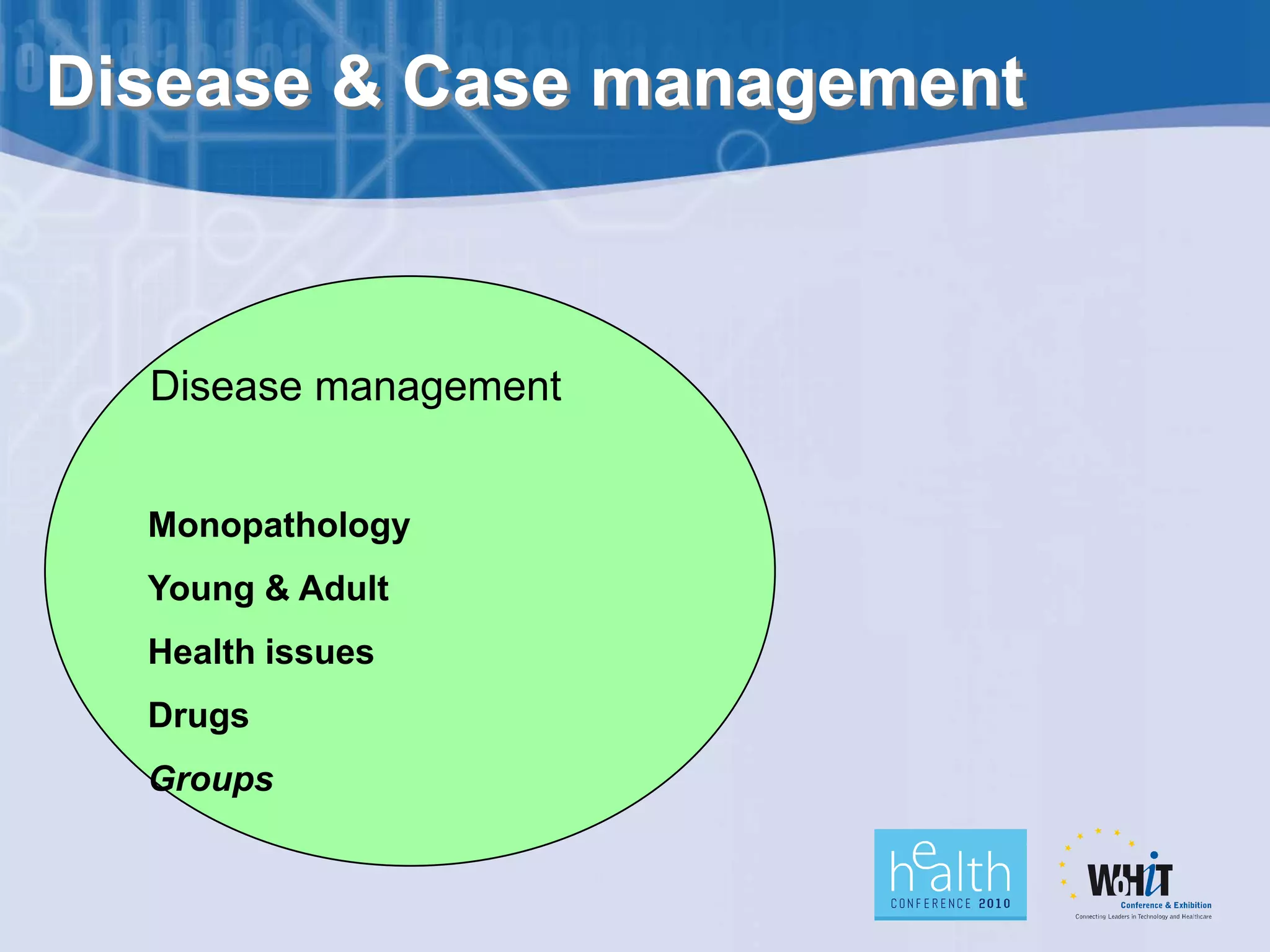
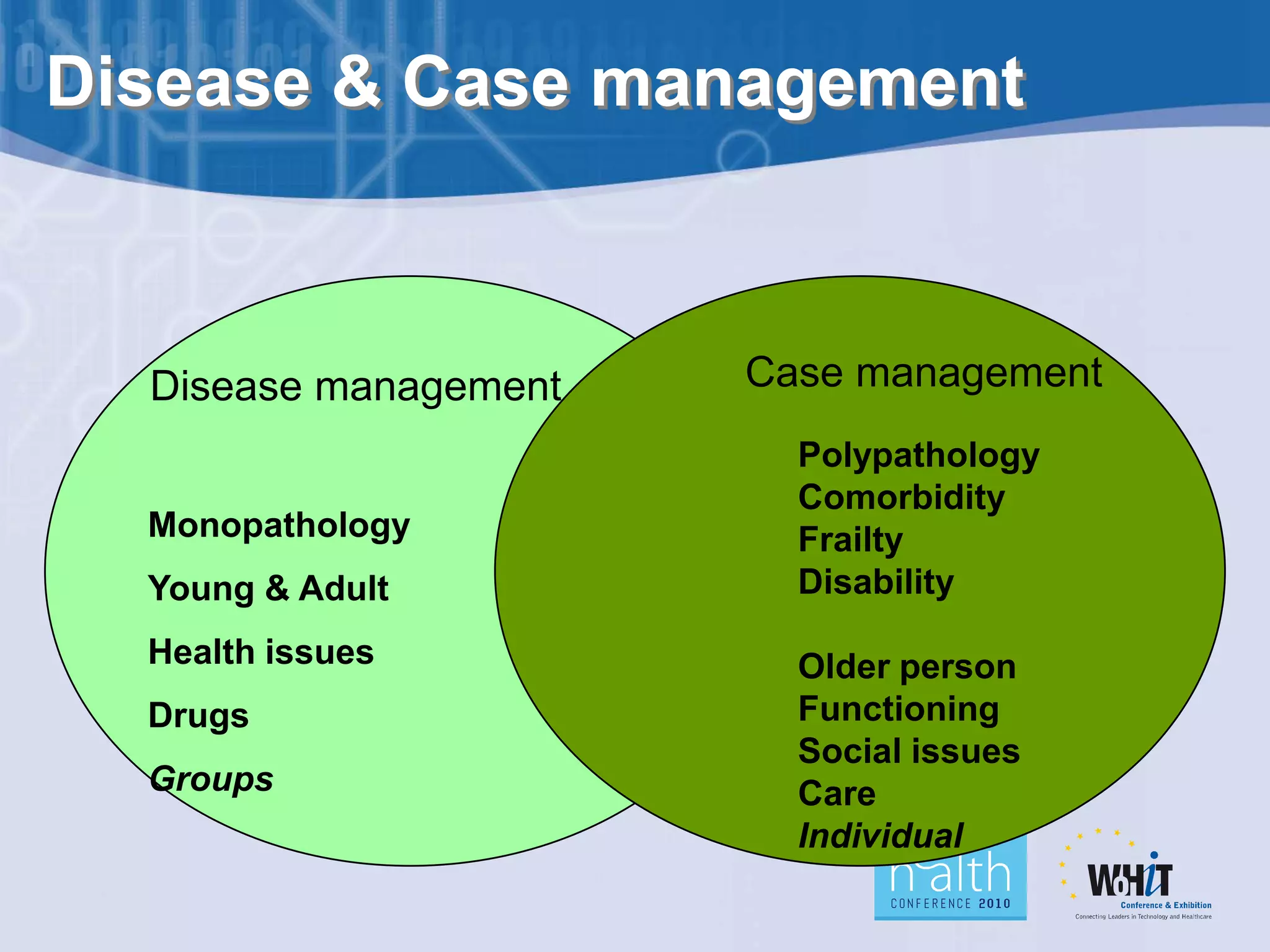
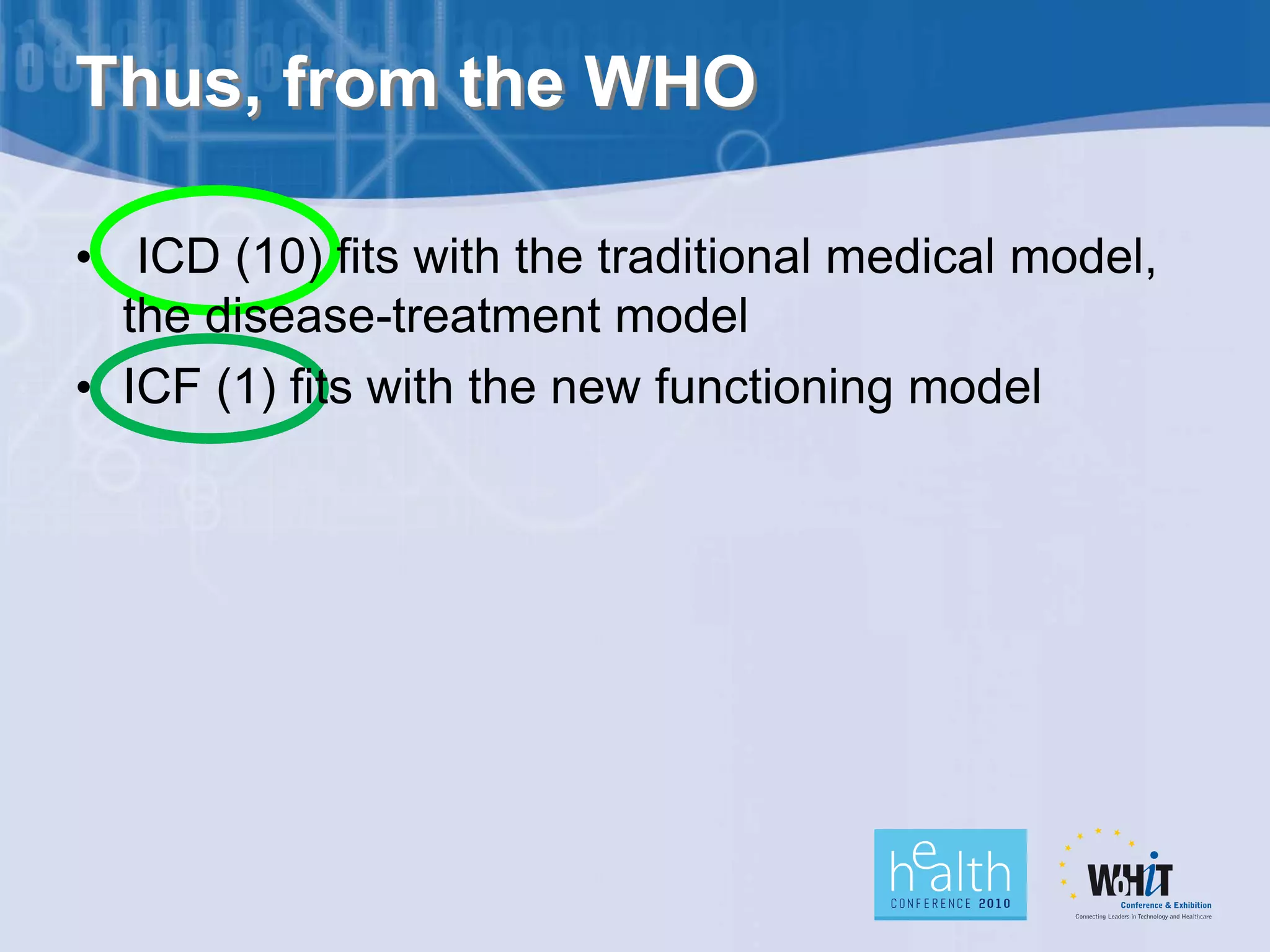
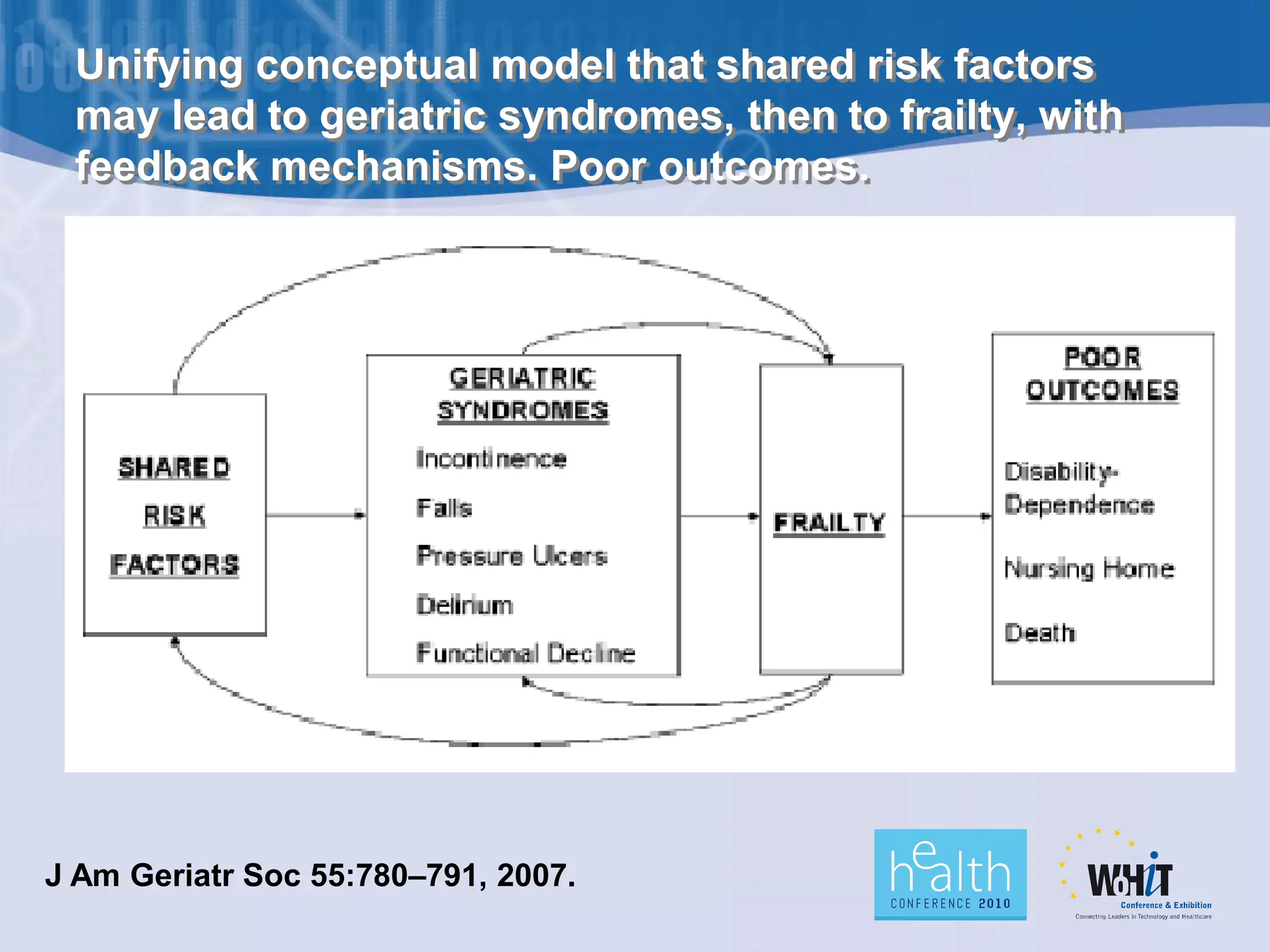




The document discusses a shift towards a new health paradigm focusing on aging, frailty, and the role of technology in elderly care. It highlights the need for a functional approach to healthcare that addresses the lived experiences of older adults, including environmental and human rights needs. Ultimately, it emphasizes the importance of gerontechnology in enhancing quality of life and reducing caregiver burden.



































































