Africa's Health Care Worker Crisis: Views from the Ground
•Download as PPT, PDF•
2 likes•2,160 views

A PowerPoint presentation by the PHR Health Action AIDS team, about the health systems crisis, with photos from East Africa. http://physiciansforhumanrights.org http://healthactionaids.org
![[object Object],[object Object],[object Object],[object Object],[object Object],A health worker displays the entire drug supply at a clinic in central Kampala, Uganda’s capitol city.](data:image/gif;base64,R0lGODlhAQABAIAAAAAAAP///yH5BAEAAAAALAAAAAABAAEAAAIBRAA7)
More Related Content
Viewers also liked
Viewers also liked (8)
More from Physicians for Human Rights
More from Physicians for Human Rights (18)
Recently uploaded
Recently uploaded (20)
Africa's Health Care Worker Crisis: Views from the Ground
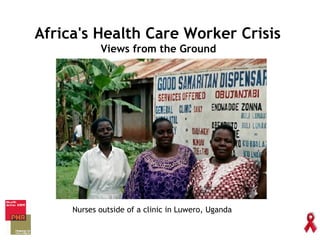
- 1. Africa's Health Care Worker Crisis Views from the Ground Nurses outside of a clinic in Luwero, Uganda
- 3. DENOSA, the national nursing union in South Africa, predicts that more than 300 specialist nurses leave the country every month. Source: The Joint Learning Initiative 2004 Above: A child sleeps in a hospital bed in Karamoja, one of the poorest and most underserved areas in Uganda. Senegal has 6 doctors per 100,000 people, the equivalent of having 36 doctors for the entire city of Boston. Ask any African doctor or nurse, any relief worker or international health official working in Africa--the continent’s health worker shortage is a catastrophe. It is caused by many factors: small government health budgets, recruitment by Western countries and research projects, and even the welcome availability of AIDS treatment, which is flooding clinics not unequipped to deal with so many people. But there are solutions.
- 4. “ I want to become a doctor because there is so much suffering here. Africa is known as the sick continent, with more illness than anywhere else. I really want, in my small way, in my small area, to help Africa. If year after year, we all go away, the Ugandan system will continue to crumble. What about our kids? What about the future of the country?” --Stella Oolo, a Ugandan Medical Student
- 5. “ Our overwhelming finding to date is that all life-saving programs, no matter how simple and obvious their potential implementation may seem, suffer from the enormous global deficit in skilled healthcare workers. The World Health Organization estimates there is currently a critical deficit of 2.4 million doctors, nurses and other healthcare professionals, meaning that people are already suffering and dying for lack of this pool of talent.” --Laurie Garrett, member of the Global Health Program of the Council on Foreign Relations, June, 2007 Health workers are the engine that drive health systems . A broken ambulance in Gulu, Uganda
- 6. What Causes the Health Worker Crisis in Africa? #1 Low salaries and benefits #2 Severely limited training and career opportunities #3 Shattered health systems #4 Inadequate occupational safety #5 Migration to wealthy nations #6 The impact of HIV/AIDS Many factors contribute to the health workforce crisis in Africa. Most African health workers want to stay and practice medicine in their own country. However, a variety of challenges make it very hard for doctors and nurses to stay:
- 7. “ I very much want to stay in Uganda but there is a big temptation to work abroad. We are offered peanuts in Uganda, and huge salaries in other countries. Ugandan doctors make $250 a month—I have a relative in UK who makes 50 pounds PER HOUR. He makes as much in 4 hours as I would make in a month. Another friend’s uncle, a psychiatrist in the UK, makes 8,000 pounds per month. Students have a passion to help their own people, but we need money.” --Ronnie Kiweewa, a Ugandan Medical Student Challenge #1: The Impact of Low Salaries Ronnie (far right) and a group of medical student activists in front of Mulago Hospital in Uganda
- 9. Empty supply shelves in Rakai, Uganda Challenge #3: Shattered Health Systems Some hospitals have no hand soap, no disinfectant to clean operating rooms, no latex gloves, no masks, and limited essential medications. In some cases there may be only one health worker for an entire clinic, who is on call seven days per week. A 2002 study by the Uganda Ministry of Health found fewer than 20% of clinics surveyed had electricity, only 66% had an on-site water source, only 40% had infection control provisions like sharps containers in place, and many lacked properly trained staff.
- 10. “ The heath system is shattered. Patients came to the clinic where I worked looking for medicine, but the only lab tech was gone. We could not send their samples for tests, so could only diagnose using clinical guidelines. We can’t properly serve our patients this way, which is discouraging.” --Nelson Igaba, a Ugandan School Student
- 11. “ There is also the obvious problem of protection—we have not had access to Hepatitis B vaccinations or PEP (and) there is no guarantee of safety—no gloves, no drugs, no vaccines.” --Nixon Nixonzima Ugandan Medical Student US and Ugandan health workers present a potential campaign on occupational safety and gloves for health workers at a symposium in Kampala Challenge #4 Inadequate Occupational Safety
- 15. YOU CAN HELP. Support the Global HEALTH Act of 2010 The Global HEALTH Act of 2010 responds forcefully and comprehensively to health systems that are broken, with the health workers who are at the core of these systems often missing. At the bill’s own core is a new Global Health Workforce Initiative to support a comprehensive approach to meeting their health workforce needs, including developing and implementing national health workforce plans. The Initiative would initially include at least 12 countries, with the bill authorizing $2 billion over five years to help countries recruit, train, retain, equitably distribute, and increase the effectiveness of their health workforce.
- 16. Above: Medical students from Physicians for Human Rights and the American Medical Students Association demonstrated at the Toronto International AIDS conference in 2006 in solidarity with their African colleagues. Empty white coats symbolized the doctors and nurses missing from African countries. Contact us to help! For more information, contact PHR National student Program coordinator Hope O’Brien at hobrien@phrusa.org.