APPROACH TO THEPATIENT:
• Abdominal pain is the major symptom of acute pancreatitis. Pain may vary from
mild discomfort to severe, constant, and incapacitating distress.
• Characteristically, the pain, which is steady and boring in character, is located in
the epigastrium region and may radiate to the back, chest, flanks, and lower
abdomen.
• Nausea, vomiting, and abdominal distention due to gastric and intestinal
hypomotility are also frequent complaints.
• Physical examination frequently reveals a distressed and anxious patient.
• Low-grade fever, tachycardia, and hypotension are common.
• Shock is not unusual and may result from
(1) hypovolemia secondary to exudation of blood and plasma proteins into the
retroperitoneal space;
(2) increased formation and release of kinin peptides, which cause vasodilation and
increased vascular permeability; and
(3) systemic effects of proteolytic and lipolytic enzymes released into the
circulation.
3.
• Jaundice occursinfrequently; when present, it may be a consequence of
extrinsic compression due to peripancreatic edema or a pancreatic head
mass or of intraductal obstruction from a common bile duct stone or
sludge.
• Erythematous skin nodules due to subcutaneous fat necrosis rarely occur.
In 10–20% of patients, there are pulmonary findings, including basilar rales,
atelectasis, and pleural effusion, the latter most frequently left-sided.
• Abdominal tenderness and muscle rigidity are present to a variable degree,
but compared with the intense pain, these signs may be less impressive.
• Bowel sounds are usually diminished or absent.
• An enlarged pancreas from an acute fluid collection, walled-off necrosis, or
a pseudocyst may be palpable in the upper abdomen later in the course of
the disease (i.e., 4–6 weeks).
4.
• A faintblue discoloration around the umbilicus (Cullen’s sign) may
occur as the result of hemoperitoneum, and a blue-red-purple or
green brown discoloration of the flanks (Turner’s sign) reflects tissue
breakdown of hemoglobin from severe necrotizing pancreatitis with
hemorrhage; both findings are rare but reflect an increased clinical
severity
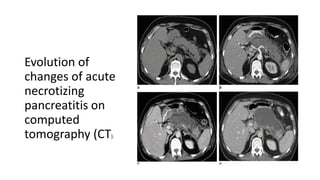
1. CT scanof the abdomen without IV contrast performed on admission for
a patient with acute gallstone pancreatitis, showing mild peripancreatic
stranding.
2. Contrast-enhanced CT scan of the abdomen performed on the same
patient 1 week after admission shows extensive intrapancreatic necrosis,
evidenced by the lack of contrast enhancement in the pancreatic body
with very minimal enhancement noted at the distal most aspect of the
pancreatic tail.
3. Contrast-enhanced CT scan of the abdomen performed on the same
patient 2 weeks after admission demonstrates a semiorganized,
heterogeneous fluid collection, referred to as an acute necrotic
collection. On this image, a small area of viable pancreatic parenchyma is
seen at the tail of the pancreas.
4. Contrast-enhanced CT scan of the abdomen performed on the same
patient 5 weeks after admission demonstrates a well-encapsulated fluid
collection, essentially replacing the pancreas, referred to as walled-off
necrosis.
11.
ACUTE PANCREATITIS MANAGEMENT
•It is important to recognize that 85–90% of cases of acute pancreatitis are
self-limited and subside spontaneously, usually within 3–7 days after onset,
and do not exhibit organ failure or local complications.
• The management of acute pancreatitis begins in the emergency ward.
• After a diagnosis has been confirmed, early and aggressive fluid
resuscitation is critical.
• Additionally, intravenous analgesics are administered, severity is assessed,
and a search for etiologies that may impact acute care is begun.
• Patients who do not respond to aggressive fluid resuscitation in the
emergency ward should be considered for admission to a step-down or
intensive care unit for aggressive fluid resuscitation, hemodynamic
monitoring, and management of any organ failure.
12.
Fluid Resuscitation andMonitoring Response to Therapy
• The most important treatment intervention for acute pancreatitis is
early, aggressive intravenous fluid resuscitation to prevent systemic
complications from the secondary systemic inflammatory response.
• The patient is initially made NPO to minimize nutrient-induced
stimulation of the pancreas and is given intravenous narcotic
analgesics to control abdominal pain and supplemental oxygen (as
needed).
• Intravenous fluids of lactated Ringer’s or normal saline are initially
bolused at 15–20 mL/kg (1050–1400 mL), followed by 2–3 mL/kg per
hour (200–250 mL/h), to maintain urine output >0.5 mL/kg per hour.
• Serial bedside evaluations are required every 6–8 h to assess vital
signs, oxygen saturation, and change in physical examination to
optimize fluid resuscitation.
13.
• Lactated Ringer’ssolution has been shown to decrease systemic inflammation
(lower C-reactive protein levels from admission) and may be a better crystalloid
than normal saline.
• A targeted resuscitation strategy with measurement of hematocrit and BUN every
8–12 h is recommended to ensure adequacy of fluid resuscitation and monitor
response to therapy, noting that a less aggressive resuscitation strategy may be
needed in milder forms of pancreatitis.
• A rising BUN during hospitalization is not only associated with inadequate
hydration but also higher in-hospital mortality.
• A decrease in hematocrit and BUN during the first 12–24 h is strong evidence that
sufficient fluids are being administered.
• Serial measurements and bedside assessment for fluid overload are continued,
and fluid rates are maintained at the current rate.
• If the BUN or hematocrit fails to respond (i.e., remains elevated or does not
decrease) to this bolus challenge and increase in fluid rate, consideration of
transfer to an intensive care unit is strongly recommended for hemodynamic
monitoring.
14.
Nutritional Therapy
• Alow-fat solid diet can be administered to subjects with mild acute
pancreatitis once they are able to eat.
• Enteral nutrition should be considered 2–3 days after admission in
subjects with more severe pancreatitis instead of total parenteral
nutrition (TPN).
• Enteral feeding maintains gut barrier integrity, limits bacterial
translocation, is less expensive, and has fewer complications than
TPN.
15.
Management of LocalComplications
• Patients exhibiting signs of clinical deterioration despite aggressive
fluid resus citation and hemodynamic monitoring should be assessed
for local complications, which may include necrosis, pseudocyst
formation, pancreas duct disruption, peripancreatic vascular
complications, and extrapancreatic infections.
• A multidisciplinary team approach is recommended, including
gastroenterology, surgery, interventional radiology, and intensive care
specialists, and consideration should also be made for transfer to a
tertiary pancreas center of excellence.
16.
NECROSIS
• Repeated CTor MRI imaging should also be considered with any
change in clinical course to monitor for complications (e.g.,
thromboses, hemorrhage, abdominal compartment syndrome).
• In general, sterile necrosis is most often managed conservatively
unless complications arise. Once a diagnosis of infected necrosis is
established and an organism identified, targeted antibiotics should be
instituted.
• Pancreatic drainage and/or debridement (necrosectomy) should be
considered for definitive management of infected necrosis, but
clinical decisions are ultimately influenced by the clinical response
since almost two-thirds of patients respond to antibiotic treatment
with or without percutaneous drainage.
17.
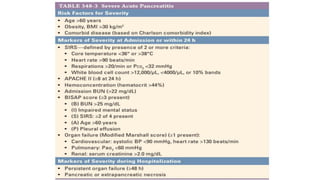
Assessment of Severityand Hospital Triage:
• The Bedside Index of Severity in Acute Pancreatitis (BISAP) incorporates five
clinical and laboratory parameters obtained within the first 24 h of hospitalization
(BUN >25 mg/dL, impaired mental status (Glasgow coma scale score] 60 years,
and pleural effusion on radiography—that can be useful in assessing severity.
• The presence of three or more of these factors was associated with substantially
increased risk for in-hospital mortality among patients with acute pancreatitis.
• In addition, an elevated hematocrit >44% and admission BUN >22 mg/dL are also
associated with more severe acute pancreatitis.
• Incorporating these indices with the overall patient response to initial fluid
resuscitation in the emergency ward can be useful at triaging patients to the
appropriate hospital acute care setting.
• In general, patients with lower BISAP scores, hematocrits, and admission BUNs
tend to respond to initial management and can be safely triaged to a regular
hospital ward for ongoing care.
18.
• If SIRSis not present at 24 h, the patient is unlikely to develop organ
failure or necrosis.
• Therefore, patients with persistent SIRS at 24 h or underlying
comorbid illnesses (e.g., chronic obstructive pulmonary disease,
congestive heart failure) should be considered for a step-down unit
setting if available.
• Patients with higher BISAP scores and elevations in hematocrit and
admission BUN who do not respond to initial fluid resuscitation and
exhibit evidence of respiratory failure, hypotension, or organ failure
should be considered for direct admission to an intensive care unit.
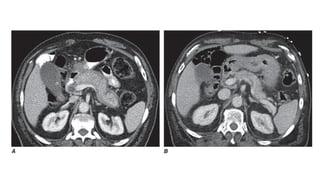
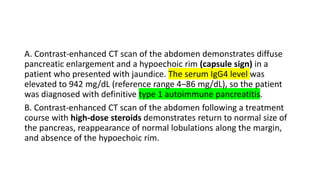
A. Contrast-enhanced CTscan of the abdomen demonstrates diffuse
pancreatic enlargement and a hypoechoic rim (capsule sign) in a
patient who presented with jaundice. The serum IgG4 level was
elevated to 942 mg/dL (reference range 4–86 mg/dL), so the patient
was diagnosed with definitive type 1 autoimmune pancreatitis.
B. Contrast-enhanced CT scan of the abdomen following a treatment
course with high-dose steroids demonstrates return to normal size of
the pancreas, reappearance of normal lobulations along the margin,
and absence of the hypoechoic rim.
26.
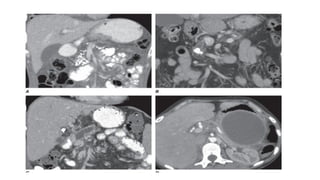
• A. Numerouspunctate calcifications involving the pancreatic
parenchyma in the head and body.
• B. A moderate-sized calculus visualized in the pancreatic duct with
associated ductal dilation.
• C. Significant pancreatic duct dilation and adjacent parenchymal
atrophy secondary to a pancreatic duct stricture (which is not well
seen on this scan).
• D. A large unilocular, encapsulated cyst in the tail of the pancreas
consistent with a pseudocyst from prior pancreatitis. Note adjacent
pancreatic parenchymal atrophy.
28.
TREATMENT OF ChronicPancreatitis
• STEATORRHEA
1. The treatment of steatorrhea with pancreatic enzyme replacement
therapy is conceptually straightforward, yet complete correction of
steatorrhea is uncommon.
2. Enzyme therapy usually brings diarrhea under control and restores
absorption of fat to an acceptable level and affects weight gain.
3. Thus, pancreatic enzyme replacement is the cornerstone of therapy.
4. In treating steatorrhea, it is important to use a potent pancreatic
formulation that will deliver sufficient lipase into the duodenum to
correct maldigestion and decrease steatorrhea.
29.
1. For adultpatients with exocrine pancreatic insufficiency, it is
generally recommended to start at a dosage of 25,000–50,000 units
of lipase taken during each meal;
2. however, the dose may need to be increased up to 100,000 units of
lipase depending on the response in symptoms, nutritional
parameters, and/or pancreas function test results.
3. Additionally, some may require acid suppression with proton pump
inhibitors to optimize the response to pancreatic enzymes.
4. Monitoring nutritional parameters such as fat-soluble vitamins, zinc
levels, body weight, and periodic bone mineral density
measurement should be considered.

![Assessment of Severity and Hospital Triage:
• The Bedside Index of Severity in Acute Pancreatitis (BISAP) incorporates five
clinical and laboratory parameters obtained within the first 24 h of hospitalization
(BUN >25 mg/dL, impaired mental status (Glasgow coma scale score] 60 years,
and pleural effusion on radiography—that can be useful in assessing severity.
• The presence of three or more of these factors was associated with substantially
increased risk for in-hospital mortality among patients with acute pancreatitis.
• In addition, an elevated hematocrit >44% and admission BUN >22 mg/dL are also
associated with more severe acute pancreatitis.
• Incorporating these indices with the overall patient response to initial fluid
resuscitation in the emergency ward can be useful at triaging patients to the
appropriate hospital acute care setting.
• In general, patients with lower BISAP scores, hematocrits, and admission BUNs
tend to respond to initial management and can be safely triaged to a regular
hospital ward for ongoing care.](https://image.slidesharecdn.com/pancreatitis-250801040054-42f2b101/85/Acute-Pancreatitis-UG-MBBS-General-Surgery-17-320.jpg)