Biorisk
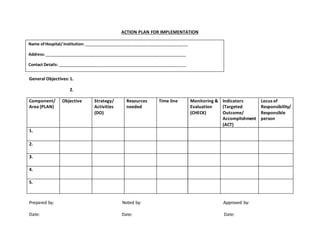
- 1. ACTION PLAN FOR IMPLEMENTATION
Name of Hospital/ Institution: _______________________________________________
Address: ________________________________________________________________
Contact Details: __________________________________________________________
General Objectives: 1.
2.
Component/
Area (PLAN)
Objective Strategy/
Activities
(DO)
Resources
needed
Time line Monitoring &
Evaluation
(CHECK)
Indicators
(Targeted
Outcome/
Accomplishment
(ACT)
Locus of
Responsibility/
Responsible
person
1.
2.
3.
4.
5.
Prepared by: Noted by: Approved by:
Date: Date: Date: