1. Effect of extended infusion piperacillin/tazobactam on mortalityEffect of extended infusion piperacillin/tazobactam on mortality
and length of stay at a two hospital community health systemand length of stay at a two hospital community health system
Brian Thomas, PharmD Candidate1
; Shari Rosen, PharmD, BCPS2
; Daniel Abazia, PharmD, BCPS1,2
; Douglas St. John, PharmD2
; Terri Catalano-Christou, MS, RPh2
1
Ernest Mario School of Pharmacy, Rutgers, The State University of New Jersey; 2
Capital Health
IRB-approved, retrospective chart review
Inclusion Criteria
Inpatients aged 18 years and older
Received at least 72 hours of TI-PT from January 2012 to
June 2013, or
Received at least 72 hours of EI-PT from January to June
2014
Exclusion Criteria
Receipt of both TI-PT and EI-PT regimens
Unpaired, 2-sided t-test for continuous data
Chi-squared or Fisher’s exact test for categorical data
RESULTS
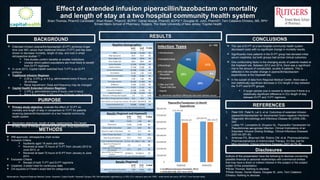
Abbreviations: Regional-Regional Medical Center; Hopewell- Capital Health, Hopewell Campus; NS- Not statistically significant (p > 0.05); ICU- intensive care unit; WBC - white blood cell count; AST/ALT- liver function tests;
The use of EI-PT at a two-hospital community health system
decreased costs with no significant change in mortality results.
Significantly more patients in the EI-PT group had elevated initial
serum creatinine, but both groups had similar clinical outcomes.
One confounding factor is the changing acuity of patients treated at
the Hopewell site. Between 2012 and 2014, there was a significant
rise in the amount of complicated, acutely ill patients. This is
reflected in the smaller change in piperacillin/tazobactam
expenditures at the Hopewell site.
In the subset of data from Regional Medical Center, there was a
non-statistically significant decrease in ICU length of stay between
the TI-PT and EI-PT groups.
A larger sample size is needed to determine if there is a
statistically significant difference in ICU length of stay
between EI-PT and TI-PT regimens.
CONCLUSIONS
REFERENCES
1. Patel GW, Patel N, Lat A, et al. Outcomes of extended infusion
piperacillin/tazobactam for documented Gram-negative infections.
Diagnostic Microbiology and Infectious Disease 64 (2009) 236–
240.
2. Lodise TP, Lomaestro B, Drusano GL. Piperacillin-Tazobactam for
Pseudomonas aeruginosa Infection: Clinical Implications of an
Extended- Infusion Dosing Strategy. Clinical Infectious Diseases
2007;44:357–63.
3. Ambrose PG, Bhavnani SM, Rubino CM, et al. Pharmacokinetics-
Pharmacodynamics of Antimicrobial Therapy: It’s Not Just for
Mice Anymore. Clinical Infectious Diseases 2007;44:79–86.
Disclosures
Authors of this presentation have the following to disclose concerning
possible financial or personal relationships with commercial entities
that may have a direct or indirect interest in the subject or the subject
matter of this presentation:
Brian Thomas: Nothing to disclose
Shari Rosen, Daniel Abazia, Douglas St. John, Terri Catalano-
Christou: Nothing to disclose
Results (Regional and Hopewell)
EI-PT
(n = 50)
TI-PT
(n = 50)
P-value
Death 5 (10) 2 (4) NS
Readmission 7 (14) 9 (18) NS
Mean Length of Stay (days) 12.0 12.0 NS
Mean ICU Length of Stay (days) 7.6 11.7 NS
Mean Therapy Days (days) 6.4 6.3 NS
Mean Drug Used (grams) 57.7 77.8 0.03
Mean Ventilated Therapy Days 4.72 (n = 9) 3.96 (n = 14) NS
Mean SCr at Therapy End
(mg/dL)
2.0 1.2 NS
Mean WBC at Therapy End
(103
cells/uL)
12.1 10.5 NS
Mean AST/ALT at Therapy End
(units/L)
50.9/61.2 73.2/64.4 NS
All data presented as n (%) unless otherwise specified
Baseline Demographics
EI-PT
(n = 50)
TI-PT
(n = 50)
P-value
Male 28 (56) 23 (46) NS
Mean Age (years) 65.0 62.0 NS
Mean Height (cm) 170.8 169.8 NS
Mean Weight (kg) 83.9 83.8 NS
Cardiac Morbidity 12 (24) 16 (32) NS
Diabetes Mellitus 17 (34) 9 (18) NS
Chronic Kidney Disease 10 (20) 5 (10) NS
Hemodialysis 8 (16) 1 (2) 0.04
Pulmonary Comorbidity 5 (10) 8 (16) NS
Cirrhosis 2 (4) 1 (2) NS
Neurologic disorder 16 (32) 12 (24) NS
Malignancy 9 (18) 11 (22) NS
Source Control Procedure 6 (12) 6 (12) NS
Concomitant Antibiotics 19 (38) 19 (38) NS
Surgical Procedure 17 (34) 16 (32) NS
Mean SCr at Therapy Start (mg/dL) 2.3 1.1 0.01
Mean WBC at Therapy Start (103
cells/uL) 14.5 14.9 NS
Mean AST/ALT at Therapy Start (units/L) 44.1/42.7 46.4/43.8 NS
Patients Admitted to ICU 30 (60) 23 (46) NS
All data presented as n (%) unless otherwise specified
Results (Regional)
EI-PT
(n = 12)
TI-PT
(n = 18)
P-value
Mean ICU Length of Stay (days) 5.50 11.61 NS
All data presented as n (%) unless otherwise specified
Extended infusion piperacillin/tazobactam (EI-PT) achieves longer
time over MIC values than traditional infusion (TI-PT) and has been
shown to decrease mortality, length of stay, and cost in small
retrospective studies1,2,3
Few studies confirm benefits at smaller institutions
Unclear which patient populations are most likely to benefit
from EI-PT regimens
In June 2013, Capital Health switched from TI-PT to an EI-PT
protocol
Traditional Infusion Regimen
2.25 g, 3.375 g, or 4.5 g, administered every 6 hours, over
30 minutes
Renal Adjustment: Dose and frequency may be changed
Capital Health Extended Infusion Regimen
3.375 g, administered every 8 hours, over 4 hours
Renal Adjustment: 3.375 g every 12 hours, over 4 hours
BACKGROUND
Primary study objective: evaluate the effect of EI-PT on
mortality and length of stay in comparison to TI-PT for patients
receiving piperacillin/tazobactam at a two hospital community
health system
Secondary objectives: length of stay, readmissions, ICU length
of stay, days of therapy, amount of drug used, drug expenditures
PURPOSE
METHODS
21%
3%
18%
22%
29%
1%
6%
No statistically significant differences were seen between groups