Topic 2 Genesand health
Testing for
cystic fibrosis
Textbook page 96-100
2.
Today’s lesson
Testing forthe cystic fibrosis allele (or any faulty allele)
Understand the uses of genetic screening:
• identification of carriers
• pre-implantation genetic diagnosis
• pre-natal testing (amniocentesis and chorionic villus
sampling)
Understand the implications of prenatal genetic screening.
Be able to identify and discuss the social and ethical issues
related to genetic screening from a range of ethical
viewpoints.
3.
The sequencing ofthe CFTR protein
gene in 1989 led to the possibility of
genetic testing for the mutated CF
allele.
Genetic screening
4.
Types of geneticscreening
1. Screening adults, children or babies after symptoms seen
to confirm diagnosis of a genetic disease
2. Identification of carriers – screening for adults to
identify carriers before deciding to start a family (pre-
conception screening)
3. Pre-implantation genetic diagnosis – screens
IVF embryos (after fertilisation) but before implantation
back into the uterus
4. Pre-natal (before birth) screening - screens fetus in
the uterus or fetal DNA (3 types - chorionic villus
sampling/CVS, amniocentesis or NIPD)
Uses of genetic screening
5.
Types of geneticscreening
Uses of genetic screening
1. To confirm diagnosis of a genetic disease
2. Identification of carriers
3. Pre-implantation genetic diagnosis – screens IVF
embryos
4. Pre-natal testing - chorionic villus sampling/CVS,
amniocentesis or NIPD – screens fetus or fetal DNA
Key Summary
6.
1. To confirmdiagnosis of the disease
Usually used to screen newborn babies to confirm they
have a genetic disease when symptoms are observed
Process
• White blood/cheek cell sample taken - both easy to
collect and diploid so contain larger quantity of DNA
• DNA extracted and tested for presence of defective/
mutated allele (confirms that they have the disease)
7.
2. To identifycarriers
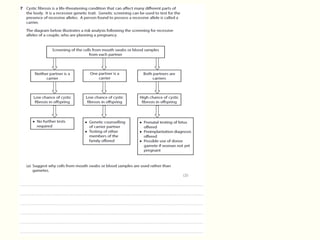
Couples considering becoming parents can be screened to
see if they are carriers for genetic diseases like CF,
especially if there is a family history of the disease -two
carriers have a 25% chance of having a child with CF
When: Any stage of life after birth (baby, child, adult)
How
• White blood/cheek cell sample taken - both easy to
collect and diploid so contain larger quantity of DNA
• DNA extracted and tested for
presence of defective/ mutated
gene – compare with normal
DNA sequence
8.
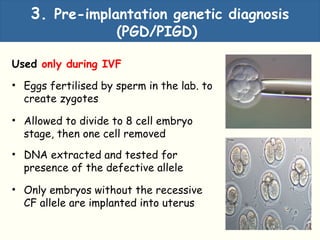
3. Pre-implantation geneticdiagnosis
(PGD/PIGD)
Used only during IVF
• Eggs fertilised by sperm in the lab. to
create zygotes
• Allowed to divide to 8 cell embryo
stage, then one cell removed
• DNA extracted and tested for
presence of the defective allele
• Only embryos without the recessive
CF allele are implanted into uterus
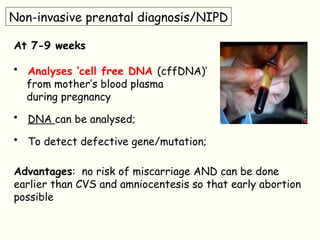
Non-invasive prenatal diagnosis/NIPD
At7-9 weeks
• Analyses ‘cell free DNA (cffDNA)’
from mother’s blood plasma
during pregnancy
• DNA can be analysed;
• To detect defective gene/mutation;
Advantages: no risk of miscarriage AND can be done
earlier than CVS and amniocentesis so that early abortion
possible
11.
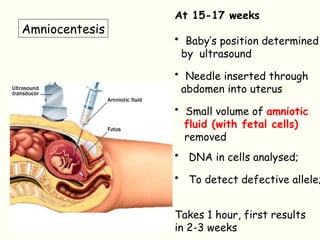
At 15-17 weeks
•Baby’s position determined
by ultrasound
• Needle inserted through
abdomen into uterus
• Small volume of amniotic
fluid (with fetal cells)
removed
• DNA in cells analysed;
• To detect defective allele;
Takes 1 hour, first results
in 2-3 weeks
Amniocentesis
12.
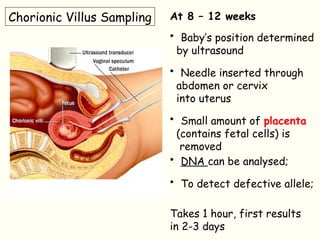
Chorionic Villus SamplingAt 8 – 12 weeks
• Baby’s position determined
by ultrasound
• Needle inserted through
abdomen or cervix
into uterus
• Small amount of placenta
(contains fetal cells) is
removed
• DNA can be analysed;
• To detect defective allele;
Takes 1 hour, first results
in 2-3 days
13.
Benefits/advantages of testing(genetic screening)/why
would some people choose to be tested?
• Gives information about abnormalities in fetus/DNA
• Allows people to make informed decisions/opportunity
for choice /consider a termination (abortion)
• Information allows people to prepare/ research
treatment/ start counselling
• Gives the choice of IVF – to implant only embryos
without the gene mutation
Key Summary
14.
Disadvantages of testing(genetic screening)
• Tests may not be 100% accurate, leading to false
negative or positive result – decisions based on false
info
• Screening does not test for all the possible mutations
that can cause cystic fibrosis
• Other genetic abnormalities may be found/may cause
further stress
Key Summary
15.
Why would somepeople choose not to be tested?
• Increased risk of procedure causing a miscarriage;
• potentially a healthy fetus would be lost;
OR
• Test result may be inaccurate (false positive/negative) ;
• false positive may lead to abortion of a healthy fetus;
OR
• Prenatal testing / abortion may be against values or
beliefs of parents
Key Summary
16.
Ethical issues relatingto the use of prenatal testing.
• risk of a miscarriage
• foetus is living – potential human being ;
• positive test result may result in a choice of abortion;
• who has the right to make the decision for the foetus /
foetus has decision rights/right to life;
• Some people believe it is unethical to cause the death of a
foetus /destroy a potential human being – it is wrong /
murder – foetus has a right to live;
• risk of false negative or false positive;
- if false positive - healthy fetus could be aborted ;
- if false negative – parents would not be prepared for a
child with a genetic disease;
Key Summary
17.
Ethical/social (paired points)
•who has right to decide if tests should be performed;
• implications of medical costs /disagreements over next step
• some other abnormality may be found;
• possible problems with future employment / insurance;
• parents may not fully understand possible risks of prenatal
testing;
• possibility of miscarriage or harm to child – healthy chold
could be lost;
• confidentiality issues for {parents / child};
• {some other abnormality may be found / paternal DNA does
not match / do other family members have right to know
results?} ;
18.
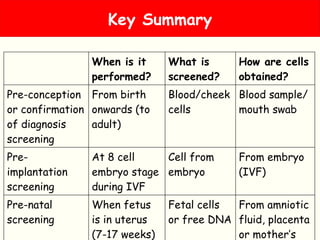
Key Summary
When isit
performed?
What is
screened?
How are cells
obtained?
Pre-conception
or confirmation
of diagnosis
screening
From birth
onwards (to
adult)
Blood/cheek
cells
Blood sample/
mouth swab
Pre-
implantation
screening
At 8 cell
embryo stage
during IVF
Cell from
embryo
From embryo
(IVF)
Pre-natal
screening
When fetus
is in uterus
(7-17 weeks)
Fetal cells
or free DNA
From amniotic
fluid, placenta
or mother’s
19.
Amniocentesis
Check that youcan …
• State the uses of genetic screening and know the situation
in which each is used
• Describe the process of amniocentesis
• Describe the process of chorionic villus sampling/ CVS
• Compare amniocentesis and CVS and give an advantage and
disadvantage of using CVS rather than amniocentesis
• Describe the process of NIPD and state advantages
• Explain ethical and social issues/implications of genetic
screening (especially prenatal)
• State advantages and disadvantages of genetic screening
Genetic screening self-test list
Stretch and challenge
Readjournals/information
http://www.nhs.uk/Conditions/Genetics/Pages/genetic-testing-an
d-counselling.aspx
(NHS genetic testing and counselling)
http://www.pku.com/What-is-PKU/history-of-phenylketonuria.php
?gclid=CPvIk-XdsrsCFdLItAodcQUAbA
(testing newborn babies for phenylketonuria)
http://www.nuffieldbioethics.org/genetic-screening (council on
bioethics)
http://www.bostonglobe.com/lifestyle/health-wellness/2013/12/09/
increase-breast-cancer-gene-screening-angelina-jolie-effect/0iw
wmG7KqyPUQpHRouD0hN/story.html
(Angelina Jolie and screening for breast cancer gene)
http://www.ndsu.edu/pubweb/~mcclean/plsc431/students/firas.ht
m
27.
Careers
Investigate a careeras a genetic counsellor
Genetic counsellors help patients and their families understand and make
informed decisions about a range of genetic conditions
As a genetic counsellor your role is to interpret and explain genetic information to
patients and to support them and their families to make use of this information.
You'll help them to understand the medical facts, including how heredity
contributes to their condition, and the options for dealing with the risk of
recurrence.
Your support will be key for patients and their families to make decisions and to
adjust to a condition, and/or the risk of recurrence of that condition.
Genetic counselling is a career attracting
graduates with an interest in medical genetics
and face-to-face patient interaction. Genetic
counsellors are highly-skilled healthcare
professionals with training and expertise in
genetic medicine and counselling.
https://www.prospects.ac.uk/job-profiles/genetic-counsellor