...............................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................



![How Does An Oral Device Work?
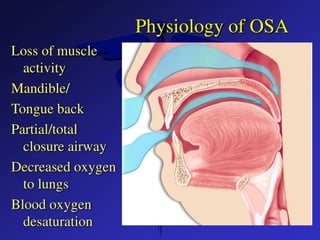
z Snoring/OSA caused by loss of airway
space
z Most oral devices advance the mandible
This pulls the șenioșlossus forwai d
z This pulls the ton•ue ìorwaid
Uÿ]3Sl“ ílii”way space is l”egained
z Snoiin•/OSA diminished oi eliminated
Othei's simply lteep the tongue pt oti
uded](https://image.slidesharecdn.com/8-250906071045-3d48d0e4/85/8-sleep-related-breathing-disorders-pptx-24-320.jpg)