Download to read offline


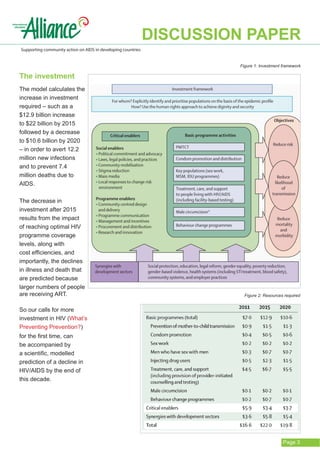





The document discusses a new investment framework for HIV/AIDS that was published in The Lancet in June 2011. The framework projects increasing spending on HIV/AIDS programs until 2015, followed by declining spending from 2015-2020 as programs reach critical coverage levels and transmission rates decline. The framework prioritizes six HIV program areas and identifies "critical enablers" like community mobilization that are needed to effectively implement programs. It provides a new model for planning and advocating for HIV resources that accounts for eventual declines in needed funding and services as control efforts succeed.










![Countdown confreport web[1]](https://cdn.slidesharecdn.com/ss_thumbnails/countdownconfreportweb1-100810075655-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




























































