NURSING
> the diagnosisof human responses to actual and potential problems.
-- American Nurses Association
> the act of utilizing the environment of the patient to assist him in his
recovery.
-- Florence Nightingale
> to assist the individual sick or well.
-- Virginia Henderson
4.
Common Themes:
Nursing isCaring.
Nursing is an Art.
Nursing is Science.
Nursing is Client-Centered.
Nursing is Holistic.
Nursing is Adaptive.
Nursing is concerned with health Promotion,
Health Maintenance and Health Restoration.
Nursing is a Helping Profession.
5.
Nursing as aProfession.
Profession
- calling that requires special knowledge, skill and
preparation.
Primary Characterisitics:
1. Education
2. Theory
3. Service
4. Autonomy
5. Code of Ethics
I. INTRODUCTION TONURSING
1. Intuitive Nursing
(primitive times to 6th
century)
a. Nursing in ancient civilizations; instinctive nursing dates
back even during the primitive tribes; Nursing was a
function that belonged to women because of their place in
society.
b. Beliefs about the cause of disease were embedded in
superstition and magic
c. Earliest recording of healing was a 4,000 year-old clay
tablet attributed to the Sumerian civilization
8.
d. As societiesevolved, nursing became a function of
female slaves who cared for infant children of wealthy
families through wet nursing and the practice of
midwifery or the provision of care to the mother and
infant during birthing; the slave-nurse was dependent on
the master, healer or priest for instruction or direction in
the care of her charge
e. Lasted through the Christian era out of feeling of
compassion for others, out of desire to help and out of
wish to do good to others as embodied in the Christian
value of “love thy neighbor as thyself.”
9.
2. APPRENTICE NURSING(6TH
- 18TH
CENTURY)
a. Also called the period of “on the job training”
b. Men engaged in Nursing during the Crusades through:
- Knights Hospitalers or Knights of Saint John of Jerusalem
- Teutonic Knights
- Knights of Saint Lazarus
c. This historical period extends from the founding of religious nursing
orders in the 6th
century, through the Crusades which began in the 11th
century, to 1836 when Theodore Fliedner reinstituted the Order of
Deaconnesses and opened a small hospital and training school in
Kaisserwerth, Germany
d. Florence Nightingale was the most famous Kaisserweth pupil; she
changed the status of nursing to a respectable occupation for women
10.
3. “EDUCATION” NURSING
a.Began in June 1860 when the Florence Nightingale School of Nursing
opened at St. Thomas Hospital in London; this school had the first
program of formal education for the nurse
b. The Philosophy of the Nightingale’s System was based on the
following:
- training of nurses should be considered as important as any
other form of education and be supported by public funds.
- training schools for nurses should have close affiliation with
hospitals but retain financial and administrative independence
from them.
- professional nurses should be responsible for the education
of nursing students rather than persons not involved in nursing
- nursing students should be provided with residence during
their training which offer them pleasant, comfortable surroundings
close to the hospital.
11.
c. US andCanada copied the Nightingale Schools of England very closely
but the US training schools failed to remain separate from the hospitals
resulting in a form of educational abuse of nursing students by the
hospitals
d. Written physician’s orders originated with Nightingale who insisted that
nurses accompany the physicians on patient visits
e. Believed that health teaching was a critical responsibility of the nurse if
national health was to improve
f. The last two decades of the 19th
century is also called the “awakening of
nursing”
12.
g. In theearly decades of the 20th
century, hospitals started to
segregate patients according to their disease process thus the
concept of clinical nurse specialist arose
h. Between 1913 and 1937, a standardized curriculum for Schools of
Nursing was prepared by the National League for Nursing Education
13.
4. CONTEMPORARY NURSING
a.Began at the end of World War II; associated with scientific and
technological developments and social changes since 1945
b. Changing patterns in Nursing education by adding more clinical
content
c. Professionalization of Nursing
d. Globalization: borderless nursing
14.
The Earliest Hospitals:
A.Hospital Real de Manila (1577)
- it was established mainly to care for the Spanish
King’s soldiers but also admitted Spanish civilians.
- founded by Gov. Francisco de Sande.
B. San Lazaro Hospital (1578)
- built exclusively for patients with leprosy.
- founded by Briother Juan Clemente.
C. Hospital de Indio (1586)
- service was in general supported by alms and
contributions from charitable persons.
15.
D. Hospital deAguas Santas (1590)
- founded by Brother J. Bautista of the Franciscan
Order.
E. San Juan De Dios Hospital (1596)
- founded byBrotherhood of Misericordia and
administered by the Hospitalliers of San Juan de
Dios.
16.
The Prominent persons:
1.Josephine Bracken
- wife of Jose Rizal. Installed a field hospital in an estate
house of Tejeros. Provided nursing care to the wounded
night and day.
2. Rosa Sevilla De Alvero
- converted their house into quarters for the Filipino soldier
during the Philippine-American war that broke out in 1899.
3. Doña Hilaria de Aguinaldo
-wife of Amelio Aguinaldo; organized the Filipino Red
Cross under the inspiration of Apolinario Mabini.
17.
4. Doña Mariade Aguinaldo
- second wife of Emilio Aguinaldo. Provided nursing care
for the Filipino soldiers during the Revolution. President of
the Filipino Red Cross branch in Batangas.
5. Melchora Aquino (Tandang Sora)
- nurse the wounded Filipino soldiers and gave them
shelter and food.
6. Trinidad Tecson
- “Ina ng Biac na Bato”, stayed in the hospital at Biac na
Bato to care for the wounded soldiers.
18.
Hospitals and NursingSchools:
1. Iloilo Mission Hospital School of Nursing
(Iloilo City, 1906)
> It was run by the Baptist Foreign Mission Society of
America.
> Miss Rose Nicolet – first superintendent
> Miss Flora Ernst – an American nurse, took charge of
the school in 1942
2. St. Paul’s Hospital School of Nursing
(Manila, 1907)
>The hospital was established by the Archbishop of
Manila, The Most Reverend Jeremiah Harty, under the
supervision of the Sisters of St. Paul de Chartres.
19.
3. Philippine GeneralHospital School of Nursing
(Manila, 1907)
> In 1907, with the support of the Gov. Gen. Forbes and
the Director of Health and among others, opened classes
in nursing under the auspices of the Bureau of Education.
> Anastacia Giron-Tupas, was the first Filipino to occupy
the position of Chief Nurse and Superintendent in the
Philippines.
20.
4. St. Luke’sHospital School of Nursing
(Quezon City, 1907)
> The Hospital is an Episcopalian Institution. It began as a
small dispensary in 1903. In 1907, the school opened with
3 Filipino girls admitted.
> Mrs. Vitiliana Beltran was the first Filipino Director of
the school.
5. Mary Johnston Hospital and School of Nursing
(Manila, 1907)
> It started as a small dispensary on Calle Cervantes.
> It was called Bethany Dispensary and was founded by
the Methodist Mission.
> Miss Librada Javelera was the first Filipino Director of
the school.
21.
The First Collegesof Nursing in the Philippines:
University of Santo Tomas, College of Nursing
> 1946
> Sor Taciana Trinanes – First Directress
Manila Central University, College of Nursing
> 1948
> Consuelo Gimeno – First Principal
University of the Philippines, College of Nursing
> 1948
> Ms. Julita Sotejo – First Dean
1. Socialization
- processby which a person learns the ways of a group or society in
order to become a functioning participant
Benner’s (1984) five levels of proficiency as the nurse acquires SKA and
values of nursing
5 STAGES:
Stage 1: Novice
- may be student or nurse entering a clinical setting where that
person has no experience
Stage 2: Advanced beginner
- demonstrates marginally accepted performance
24.
Stage 3: Competent
-nurse has been on the job in the same situation for 2 to 3
years; demonstrates organizational ability but lacks the
speed and flexibility of the proficient nurse
Stage 4: Proficient
- perceives a situation as a whole rather than just its
individual aspects; nurse focuses on long-term goals and is
oriented toward managing the nursing care of the client rather
than performing specific tasks
Stage 5: Expert
- no longer relies on rule, guidelines or maxims to
connect an understanding of the situation to an appropriate
action; have highly developed perceptual acuity or
recognitional ability, and their performance is fluid, flexible and
highly proficient
1. Care provider/ParentSurrogate
- primarily concerned with the clients needs.
*** Recognize the patient’s most immediate needs.
2. Communicator/Helper
- communicates with the client, support persons
and colleagues.
***Establish trust.
3. Teacher
- provides health teaching to effect behavior
change which focuses on acquiring new knowledge
or technical skills.
*** Assess client’s learning needs/ Assess client’s
readiness to learn.
27.
4. Counselor
- processof helping a client to recognize and cope
with stressful psychological or social problems, to
develop improved interpersonal relationships and
to promote personal growth.
*** Render active listening/ Do not give advice.
5. Client advocate
- advocates for client rights.
6. Change agent
- initiates changes and assists the client makes
modifications in the lifestyle to promote health.
- helps the client to speak up for themselves.
*** Patient must develop self awareness.
28.
7. Leader
- mutualprocess of interpersonal influence through
which the nurse helps a client make decisions in
establishing and achieving goals to improve client’s
well-being.
8. Manager
- plans, gives direction, develops staff, monitors
operations, gives reward fairly and represents both
staff members and administration as needed.
9. Researcher
- participates in scientific investigation and uses
research findings in practice.
10. Collaborator
- initiates nursing actions within the health team.
Focus of Nursing
1.Health and Wellness Promotion
- helping people develop resources to maintain or
enhance their well-being.
2. Illness Prevention
- maintain optimal health by preventing disease.
3. Health Restoration
- helping people to improve health following health problems
or illness.
4. Care of the Dying
- comforting and caring for people of all ages while they are
dying.
31.
The 4 MajorConcepts:
1. Person
- recipient of the nursing care.
2. Health
- the degree of wellness and well being that a
person experiences.
3. Environment
- pertains to the internal and external surroundings
that affects a person.
4. Nursing
- pertains to attributes, characteristics and actions
of the nurse providing care in behalf of the client or in
conjunction with the client.
GENERAL THEORIES
1. Nightingale’sEnvironmental Theory
> focuses on the patient and his environment.
> her work in Crimea (1854-1856) earned her the title
“The Lady with the Lamp”.
> also known as the First Nurse Scientist Theorist
for her work, Notes on Nursing: What it is and What it
is Not (1860).
- > she focused on changing and manipulating the
environment in order to put the patient in the best
possible conditions for nature to act.
34.
2. Virginia Henderson’sNature of Nursing
Model
> conceptualizes the nurse’s role as assisting sick or
healthy individuals to gain independence in meeting
14 FUNDAMENTAL NEEDS.
> she postulated that the unique function of a nurse is
assist the individual, sick or well, in the performance of
those activities contributing to health or its recovery (or
peaceful death) that he would perform unaided if he
had the necessary strength, will or knowledge.
> she further believed that nursing involves assisting the
client in gaining independence as rapid as possible, of
assisting him achieves peaceful death if recovery is no
longer possible.
35.
14 BASIC COMPONENTSOF NURSING
CARE ACCORDING TO VIRGINIA
HENDERSON
1. Breath normally
2. Eat and drink adequately
3. Eliminate body wastes
4. Move and maintain desirable posture
5. Sleep and rest
6. Select suitable clothes
7. Maintain body temperature within normal range by
adjusting clothing or modifying the environment
8. Keep the body clean and well-groomed and protect the
integument
9. Avoid dangers in the environment and avoid injuring
others
36.
10. Communicate withothers in expressing emotions,
needs, fears or opinions
11. Worship according to one’s faith
12. Work in such a way that there is a sense of
accomplishment
13. Play or participate in various forms of recreation
14. Learn, discover or satisfy the curiosity that leads to
the normal development and health and use the
available health facility
1-9 Physiologic Component
10 & 14 Psychological
11 Spiritual
12 & 13 Sociological
37.
3. Martha Roger’sScience of Unitary Human
Beings
> Considers man as a unitary human being co-existing with in
the universe, views nursing primarily as a science and is
committed to nursing research.
> Five assumptions about human beings:
1. Is an irreducible, four-dimensional energy field identified by
pattern.
2. Manifests characteristics different from the sum of the parts.
3. Interacts continuously and creatively with the environment.
4. Behaves as a totality.
5. As a sentient being, participates creatively in change.
38.
4. Dorothea Orem’sSelf-Care Deficit
Theory
> emphasizes the client’s self-care needs, nursing care
becomes necessary when client is unable to fulfill
biological, psychological, developmental or social
needs.
> she defined self-care as “ the practice of activities that
individuals initiate to perform on their own behalf in
maintaining life, health well-being.
> conceptualized 3 Nursing Systems:
1. Wholly compensatory
2. Partially compensatory
3. Supportive-Educative
39.
3 NURSING SYSTEMS:
WHOLLYCOMPENSATORY
- nurse acts for the patient; patient has no active role.
PARTIALLY COMPENSATORY
- both nurse and patient perform care measures.
SUPPORTIVE -EDUCATIVE
- patient is able to perform.
- patient only needs health teaching.
40.
5. Sister CallistaRoy’s Adaption Model
> views client as an adaptive system.
> She viewed each person as a unified biopsychosocial
system in constant interaction with a changing
environment.
> goal of nursing is to enhance life processes through
adaptation in four (4) adaptive modes.
1. Physiologic mode
2. Self-concept mode
a. physical self
b. personal self
3. Role function mode
4. Interdependence mode
41.
6. Imogene M.King’s Goal Attainment
Theory
> Nursing process is defined as a dynamic interpersonal
process between nurse, client and health care system.
> She described nursing as a helping profession that
assists individuals and groups in society to attain,
maintain and restore health, If is this not possible,
nurses help individuals die with dignity.
42.
7. Betty Neuman’sHealth Care System’s
Model
> based on two components - STRESS and REACTION
TO STRESS
FOUR CONCEPTS:
A.CLIENT
1. FLEXIBLE LINE OF DEFENSE - keeps system free from
stressor reactions or symptomatology; expands in the presence
of stressors to protect the core.
2. LINES OF RESISTANCE - consist of internal defensive
processes.
3. NORMAL LINE OF DEFENSE - usual level of wellness;
standard used to measure deviation from health.
43.
B. ENVIRONMENT
- haspotential to alter system stability due to internal and
external stressors; also provides resources for managing
stressors - ex. Immune system, good coping skills, family
support, community health center.
STRESSORS CAN BE:
1. EXTRAPERSONAL -
ex. unemployment, microorganisms, peer pressure
2. INTERPERSONAL - between 2 or more individuals;
ex. parent-child expectations, conflict among
colleagues
3. INTRAPERSONAL –
ex. anger, physical abilities, financial condition
44.
C. HEALTH
- conditionin which all parts and subparts are in
harmony with the whole client.
RECONSTITUTION
- process by which a person progresses from his normal line of
defense to a higher or lower state of wellness.
WELLNESS
- occurs after adaptation to stressors.
45.
D. NURSING
NURSING INTERVENTIONMODALITIES OF PREVENTION:
1. Primary Prevention
- promotion of client wellness and protection of normal line of
defense by strengthening flexible line of defense through the
reduction of risk factors and stress prevention.
2. Secondary Prevention
- protection of basic structure by strengthening internal line of
resistance.
3. Tertiary prevention
- promotion of existing reconstitution by supporting existing
strengths and resource.
46.
8. Dorothy Johnson’sBehavioral System
Model
> focuses on how the client adapts to illness; the goal of
nursing is to reduce stress so that the client can move
more easily through recovery.
> Viewed the patient’s behavior as a system, which is a
whole with interacting parts.
7 Subsystems of Behavior:
1. Ingestive
- taking in nourishment in socially and culturally
acceptable ways.
2. Eliminative
- ridding the body of waste in socially and culturally
acceptable ways.
47.
3. Affiliative
- securityseeking behavior.
4. Aggressive
- self-protective behavior.
5. Dependence
- nurturance-seeking behavior.
6. Achievement
- master of oneself and one’s environment
according to internalized standards of excellence.
7. Sexual and Role Identity behavior
48.
9. Hildegard Peplau’sInterpersonal Relations
in Nursing
> defined nursing as a therapeutic, interpersonal process which
strives to develop a nurse-patient relationship in which the nurse
serves as a resource person, counselor and surrogate.
Peplau’s Phases of Nurse-Patient Relationship:
1. Orientation Phase - leveling off between nurse and client in
terms of expectations
2. Identification Phase - selective response of the client to those
who can meet his/her needs; affected by client’s beliefs
3. Exploitation Phase - client takes control of the situation by
extracting help from the nurse
4. Resolution Phase - evaluation of care and discharge of client
49.
10. Madeleine Leininger’sTranscultural
Care and Universality Theory
Transcultural Nursing
- is culturally competent nursing care focused on
differences and similarities among cultures, with respect
to caring, health and illness, based on the client’s cultural
values, beliefs, and practices.
> she advocated that nursing is a humanistic and scientific
mode of helping a client through specific cultural caring
processes (cultural values, beliefs and practices) to
improve or maintain a health condition.
50.
11. Ida JeanOrlando’s Dynamic-Nurse
Relationship
> NURSING is a disciplined professional response
> Types of Nursing response:
a. deliberate
- (based on correct identification of patient needs)
b. automatic action
> Nursing function is concerned with providing direct
assistance to individuals in whatever setting to avoid,
diminish, relieve, or sure individual’s sense of helplessness
51.
12. Jean Watson’sPhilosophy and Science of
Caring
> Nursing is the science of caring
> Caring is more “healthogenic” than curing
> Main focus of nursing is on carative factors that
are derived from humanistic perspectives
combined with a scientific base
TEN CARATIVE FACTORS:
1. Formation of a humanistic-altruistic value system.
2. Faith-hope.
3. Cultivation of sensitivity to self and others.
52.
4. Establishing ahelping-trust relationship.
5. Expression of feelings, both positive and negative.
6. Research and systematic problem-solving.
7. Promotion of interpersonal teaching-learning.
8. Provisions for a supportive, protective and corrective
mental, physical, socio-cultural and spiritual environment
9. Assistance with the gratification of human needs.
10. Allowance for existential-phenomenological factors.
53.
13. Faye GlennAbdellah’s 21 Nursing
Problems
> defined nursing as having a problem-solving approach,
with key nursing problems related to health needs of
people.
> She also defined nursing as a service to individual and
families; therefore the society.
***Crucial in nursing practice is the correct identification of
nursing problems:
a. OVERT: apparent conditions
b. COVERT: hidden conditions
54.
Abdellah’s 21 NURSINGPROBLEMS:
1. To maintain good hygiene and physical comfort.
2. To promote optimal activity; exercise, rest and sleep
3. To promote safety through the prevention of accidents,
injury or other trauma and through the prevention and
spread of infection.
4. To maintain good body mechanics and prevent and
correct deformities.
5. To facilitate the maintenance of a supply of oxygen to all
body cells.
6. To facilitate the maintenance of nutrition of all body cells
7. To facilitate the maintenance of elimination.
55.
8. To facilitatethe maintenance of fluid and electrolyte
balance.
9. To recognize the physiological responses of the body to
disease conditions- pathological, psychological and
compensatory.
10. To facilitate the maintenance of regulatory mechanisms
and functions..
11. To facilitate the maintenance of sensory function
12. To identify and accept positive and negative
expressions, feelings and reactions.
13. To identify and accept the interrelatedness of
emotions and organic illness.
14. To facilitate the maintenance of effective verbal and
nonverbal communication.
56.
15. To promotethe development of productive
interpersonal relationships.
16. To facilitate progress toward achievement of
personal spiritual goals.
17. To create and/or maintain therapeutic environment.
18. To facilitate awareness of self as an individual with
varying physical, emotional and developmental
needs.
19. To accept the optimum possible goals in the light of
limitations, physical and emotional.
20. To use community resources as an aid in resolving
problems arising from illness.
21. To understand the social problems as influencing factors
in the case of illness.
57.
14. Nola J.Pender’s Health Promotion
Model
Health Promotion:
- directed towards increasing the level of well-being and
self-actualization of a given individual or group.
ex. maintaining 6 to 8 hours of daily sleep
Disease prevention or Health Protection:
- activities directed towards decreasing the probability of
experiencing illness by active protection of the body
against pathological stressors.
ex. BCG vaccination
58.
15. Lydia E.Hall Theory of Care, Core and
Cure
> patient is composed of three elements: the Body (care),
Pathology (cure), and the Person (core).
> nursing operates in ALL three elements.
**Care
- represents nurturance and is exclusive to nursing.
**Core
- involves the therapeutic use of self and emphasizes the
use of reflection.
**Cure
- focuses on nursing related to the physician’s orders.
59.
16. Myra EstrinLevine’s Four
Conservation Principles of Nursing
> She advocated that nursing is a human interaction and
proposed four conservation principles of nursing which are
concerned with the unity and integrity of the individual.
> The Four Conservation Principles are as follows:
1. Conservation of Energy
2. Conservation of Structural Integrity
3. Conservation of Personal Integrity
4. Conservation of Social Integrity
CONCEPT OF MAN
A.ATOMISTIC APPROACH
The atomistic study of man views man as an organism
composed of different organ systems where each
system is composed of organs and ear organ is
composed of tissues and cells.
B. HOLISTIC APPROACH
This view traces man’s relationship with other human
beings in the suprasystem of society. This approach
views man as a whole organism with interrelated and
interdependent parts functioning to produce behavior.
Man as a whole therefore is different from and more than
the sum of his component parts. The dimensions of man
include the physical, social, spiritual, cognitive and
psychological aspects.
62.
- Man asa social being is capable of relating with others.
His first agent of socialization is the family where he is
nurtured, where he learns his first language and where
he first learns to socialize.
- Man as a spiritual being is capable of such virtues as
faith, hope and charity. Faith is the unquestioning belief
in someone or something. It is the foundation where
hope rests. Charity means the love of man for his
fellowmen. Man as a spiritual being believes in a power
beyond himself and of transcending one’s limitations.
63.
- Man asa thinking being is capable of perception,
cognition, and communication. He is also capable of
logical thinking and reasoning.
- Man as a psychological being is capable of rationality.
His rational side makes him merciful, kind and
compassionate.
- Man as a physical being has such characteristics as
genetic endowment, sex, other physical attributes,
physical structure and functions.
64.
Abraham Maslow’s
Hierarchy ofBasic Human Needs
NEED
- is something that is essential to the survival of humans.
A basic need is something whose:
1. Absence may lead to illness
2. Presence may signal health or prevent illness
3. If unmet needs are met or fulfilled, health may be
restored
65.
FIRST LEVEL: PhysiologicalNeeds
a. Oxygen e. Elimination
b. Fluids f. Shelter
c. Nutrition g. Rest
d. Temperature H. Sex
SECOND LEVEL: Safety and Security Needs
1. Physical Safety:
- involves reducing or eliminating threats to the
body such as illness, accident and environmental
exposure.
2. Psychological Safety:
- understanding and the appropriateness of what
to expect from others, from new experiences and from
encounters with the environment.
66.
THIRD LEVEL: Loveand Belonging Needs
- need to establish social relationships and to
experience emotional nurturance and care to and from
others.
FOURTH LEVEL: Esteem and Self-Esteem Needs
- linked with the desire for strength, achievement,
adequacy, competence, confidence, and independence.
FIFTH LEVEL: Need for Self-Actualization
- highest level of all needs.
67.
Characteristics of aself-actualized individual:
1. Solves own problems.
2. Assists others in problem-solving.
3. Accepts suggestions of others.
4. Has broad interest in work and social topics.
5. Possesses good communication skills as a listener
and communicator.
6. Manages stress and assists others in managing stress.
7. Enjoys privacy.
8. Seeks new experiences and knowledge.
9. Shows confidence in abilities and decisions.
10. Anticipates problems and successes.
11. Likes self.
68.
Characteristics of BasicHuman Needs:
1. Needs are universal
2. Needs may be met in different ways.
3. Needs may be stimulated by external and internal
factors.
4. Priorities may be altered.
5. Needs may be deferred.
6. Needs are interrelated.
CONCEPT OF HEALTH,WELLNESS,
WELL-BEING AND ILLNESS
HEALTH
> is the fundamental right of every human being. It
is the state of integration of the body and mind.
- is a state of complete physical, mental, and social
well-being, and not merely the absence of disease or
infirmity. (WHO)
- is the ability to maintain the internal milieu. Illness
is the result of failure to maintain the internal environment.
(Claude Bernard)
71.
> is beingwell and using one’s power to the fullest extent.
Health is maintained through the prevention of diseases via
environmental health factors. (Florence Nightingale)
> is the ability to maintain homeostasis or dynamic equilibrium.
(Walter Cannon)
> is a dynamic state in the life cycle. Illness is an interference in
the life cycle. (Imogene King)
> is a state of a process of being becoming an integrated and a
whole as a person. (Sister Calista Roy)
72.
WELLNESS AND WELL-BEING
>Wellness is a state of well-being.
> Well-Being is a subjective perception of balance, harmony and vitality.
> Wellness has different dimensions:
1. Physical
- the ability to carry-out daily tasks (grooming, mobility, etc.) and to
achieve fitness of the different organ systems of the body.
2. Emotional
- the ability to manage stress and to express emotions
appropriately.
73.
3. Social
- abilityto interact successfully with people and
within the environment of which each person is a part, to
develop and maintain intimacy with significant others and
to develop respect and tolerance for those with different
beliefs.
4. Intellectual
- the ability to learn and use information effectively
for personal, family, and career development.
5. Spiritual
- the belief in some force (nature, science, religion,
or a higher power) that serves to unite human beings and
provide meaning and purpose of life.
6. Occupational
- ability to achieve balance between work and
leisure time.
74.
MODELS OF HEALTHAND WELLNESS
1. LEAVELL & CLARK’S AGENT-HOST-ENVIRONMENT
MODEL or ECOLOGICAL MODEL
This model has three dynamic interactive elements:
1. Agent: any environmental factor or stressor (biologic,
chemical, mechanical, physical, and psychological) whose
presence or absence can lead to illness or death
2. Host: person(s) who may or may not be at risk of acquiring a
disease based on family history of disease, lifestyle habits and
age
3. Environment: all factors external to the host that may or
may not predispose the person to the development of disease
75.
HEALTH-ILLNESS CONTINUA
DUNN’S HIGH-LEVELWELLNESS GRID
- A health grid in which the health axis and the
environment axis intersect to demonstrate interaction. The
health axis extends from peak wellness to death and the
environmental axis extends from very favorable to very
unfavorable. The intersection forms four health/wellness
quadrants:
76.
1. High-level wellnessin a favorable environment:
- example is a person who implements healthy
lifestyle behaviors and has economic resources to support
this lifestyle and a family or social environment who also
practices or encourages the practice of healthy lifestyle.
2. Emergent high-level wellness in an unfavorable
environmental
- example is a person who knows the importance of
implementing a healthy lifestyle but could not do so
because of family responsibilities, job demands or lacks the
resources to do so.
77.
3. Protected poorhealth in a favorable environment
- example is an ill person confined in a hospital and
whose needs are met by the hospital personnel, who can
afford appropriate medication, proper diet and other
treatments needed.
4. Poor health in an unfavorable environment
- example is a starving young child in a refugee
camp in Mindanao.
78.
HEALTH BELIEF MODEL(HBM)
Becker, 1975
> describes the relationship between a person’s belief and
behavior.
> individual perceptions and modifying factors may
influence health beliefs and preventive health behavior.
79.
Individual perceptions includesthe ff:
1. Perceived susceptibility to an illness.
2. Perceived seriousness of an illness.
3. Perceived threat of an illness.
Modifying factors include the ff:
1. Demographic variables
2. Sociopsychologic variables
3. Structural variables
4. Cues to action
80.
TRAVIS’ ILLNESS-WELLNESS CONTINUUM
-The model illustrates that movement to the right of
the neutral point indicates increasing levels of health and
well-being for an individual. This is achieved through
awareness, education and growth. In contrast, movement
to the left of the neutral point indicates a progressively
decreasing state of health.
81.
SMITH’S MODEL OFHEALTH
1. Clinical Model
- absence of signs and symptoms of disease.
2. Role Performance Model
- ability to fulfill societal roles.
3. Adaptive Model
- views health as a creative process and disease as
a failure in adaptation or mal-adaptation.
4. Eudaemonistic Model
- health is a condition of actualization or realization
of a person’s potential.
82.
Disease and Illness
Disease
–alteration in the body functioning which results
in the reduction of capacities and shortening of life span.
Illness
– a personal state in which the person feels
unhealthy.
In other words:
Disease is an illness with objective facts while Illness is a
subjective perception of not being well.
83.
Stages of Illness:
Stage1. Symptoms Experience
- experience some symptoms, persons believes something is
wrong. 3 aspects – physical, cognitive and emotional.
Stage 2. Assumption of the Sick Role
- acceptance of illness, seeks advice.
Stage 3. Medical Care Contact
- seeks advice to professionals for validation of real illness,
explanation of symptoms, reassurance or predict of outcome.
84.
Stage 4. DependentPatient Role
- the person becomes a client dependent on the
health professional for help; accepts or rejects health
professional’s suggestions; becomes more passive and
accepting.
Stage 5. Recovery/Rehabilitation
- gives up the sick role and returns to former roles
and functions.
85.
Classification of Diseases:
1.According to Etiologic Factors:
A. Hereditary – due to defect in the genes of one or other
parent which is transmitted to the offspring.
B. Congenital – due to defect in the development,
hereditary factors or prenatal infection
C. Metabolic – due to disturbance or abnormality in the
intricate processes of metabolism
D. Deficiency – results from inadequate intake or
absorption of essential dietary factor
E. Traumatic – due to injury
86.
F. Allergic –due to abnormal response of the body to
chemical and protein substances or to physical stimuli
G. Neoplastic – due to abnormal or uncontrolled growth of
cell
H. Idiopathic – cause is unknown; self-originated; of
spontaneous origin
I. Degenerative – results from the degenerative changes
that occur in the tissues and organs
J. Iatrogenic – result from the treatment of the disease
87.
2. According toDuration or Onset:
A. Acute Illness – has short duration and is severe. Signs
and symptoms appear abruptly, intense, and often
subside after a relatively short period.
B. Chronic Illness – usually longer than 6 months, and can
also affects functioning in any dimension. Is
characterized by:
> Remission – periods during which the disease is
controlled and symptoms are not obvious.
> Exacerbations – disease becomes more active given
at a future time, with recurrence of pronounced
symptoms.
C. Sub-Acute – symptoms are pronounced but more
prolonged than the acute disease.
88.
3. Disease mayalso be described as:
A. Organic
B. Functional
C. Occupational
D. Venereal
E. Familial
F. Epidemic
G. Endemic
H. Pandemic
I. Sporadic
89.
Risk Factors ofa Disease:
1. Genetic or Physiologic
- genetic predisposition.
2. Age
- increase or decrease client’s susceptibility to
acquire disease.
3. Environment
- surroundings that can affect the person.
4. Lifestyle
- habits that increases the chance of acquiring a
disease.
5. Sex
- gender.
90.
Levels of Prevention:
1.Primary Prevention
- applied on healthy individual.
focus: health promotion, disease prevention
2. Secondary Prevention
- applied on patient’s with signs and symptoms.
focus: screening, diagnosing, case-finding, early
detection, prompt treatment
3. Tertiary Prevention
- applied on patients with chronic and debilitative
disease.
focus: rehabilitation
91.
STRESS MANAGEMENT
1. Massage– manipulation of the client’s skin to promote
blood circulation.
2. Guided Imagery – suggestion of images which helps
reduce anxiety.
3. Mediation – relaxation of the mind, body and soul.
4. Relaxation Technique – quite environment, passive
attitude, comfortable position, comfortable
clothing.
5. Autogenic Training – teaching the mind and body to
follow verbal commands.
6. Therapeutic Touch – used to manage anxiety, relief
from pain.
92.
7. Yoga –combination of exercise and meditation.
8. Progressive Muscle Relaxation – series of tensing
and relaxing group of muscles
systematically.
9. Thought Stopping – stopping the negative thoughts.
10. Abdominal Breathing – breathing with the use of the
diaphragm.
11. Distraction – diverting one’s attention from one
thought to another.
12. Pharmacotherapy – the use of medication.
Communication
- exchange ofideas, feelings, and information
from one person to another.
1. Is the means to establish a helping-healing
relationships. All behavior communication influences
behavior.
2. Communication is essential to the nurse-patient
relationship.
3. Is the vehicle for establishing a therapeutic relationship.
4. Is the means by which an individual influences the
behavior of another, which leads to the successful
outcome of nursing intervention.
95.
Components of CommunicationProcess:
1. Sender
– is the person who encodes and delivers the
message.
2. Message
– is the content of the communication.
3. Channel
– is the medium used to convey the message.
4. Receiver
– is the person who receives the message.
5. Response/Feedback
– is the message returned by the receiver. It
indicates whether the meaning of the sender’s message
was understood.
96.
Modes/Types of Communication:
1.Verbal
- use of spoken or written words.
2. Nonverbal
- use of gestures, facial expressions, posture/gait,
body movements, physical appearance and body
language.
97.
Characteristics of Communication:
1.Simplicity
- the use of commonly understood words.
2. Clarity
- saying what is actually meant.
- speak slowly and enunciate words.
3. Timing and Relevance
- appropriate time.
- consider client’s concerns and interests.
4. Adaptability
- ability to adjust.
- consider circumstances and behavior
5. Credibility
- pertains to worthiness of words and reliability
Record
- a formaland legal document that provides
evidence of the client’s care.
Purposes:
1. Communication
2. Planning client care
3. Audit and quality assurance
4. Research
5. Education
6. Reimbursement
7. Legal documentation
8. Statistics
100.
Responsible for thedisposal of medical records in
government hospital:
- DOH
Criteria for disposal:
- DOH accredited
DOH Records Mgt & Archive Office
Where to get the chart of a pt who has been discharged:
- Medical Records Section
Where to obtain the client’s chart during period of
hospitalization :
- Nurse’ Station
101.
2 Types ofRecords
1. Problem Oriented Medical Record
- data are arranged based on the client’s problem rather
than the source of information.
Basic Components:
A. Database
- primary information about the client.
B. Problem List
- involves all aspects of the person’s life that requires
health care.
C. Initial Orders and Health Care Plans
D. Progress Notes
- SOAPIE, Graphic Flow Sheet, Discharge Notes
102.
2. Source OrientedMedical Record
- chart is divided & organized according to the
different sources of data.
Basic Components:
A. Admission Sheet
B. Physician’s Order
C. Medical History
D. Nurse’s Notes
E. Special Records and Reports
103.
REPORTING:
- either oral,taped or written exchanges of
information between nurses or other members of the
health care team.
Purpose: To promote continuity of care.
KINDS:
I. Change of Shift Reports
- exchange of information from the nurse of the
previous shift to the next shift.
A. Oral
B. Audiotape recording
C. Nursing Rounds
104.
II. Telephone Orders& Reports
- reports and orders via telephone.
Physician: capable of ordering the medication
RN: receives the medication order from the doctor
Important:
1. It must be countersigned by the physician within 24 hrs.
2. If it was not signed within 24 hours, notify the Head
Nurse.
3. Ideally, 2 nurses must receive the telephone order.
105.
III. Incidence Reports
-record of accidents or unusual events that occurs
in the agency.
Purpose: To prevent future harm/accidents.
Data Included:
1. Client’s name and ID number
2. Date, time and place of the incidence
3. Facts of the incidence
4. Client’s account of the incident
5. Witnesses of the incident
6. Equipments and medications involved
Facts to Remember:
1. It must be filed within 24 hours.
2. It should be submitted to the Risk Manager.
3. It should not be included in the patient’s chart.
DOCUMENTATION
- is anythingwritten or printed that is relied on as record or
proof for authorized person.
Nursing documentation must be:
Accurate.
Comprehensive.
Flexible enough to retrieve critical data, maintain continuity of care,
track client outcomes, and reflects current standards of nursing
practice.
As members of the health care team, nurses need to communicate
information about clients accurately and in timely manner.
Effective documentation ensures continuity of care, saves time and
minimizes the risk of error.
Data recorded, reported, or communicated to other health care
professionals are CONFIDENTIAL and must be practiced.
108.
Different Sheets:
1. NursingHealth History and Assessment Worksheet
- completed upon admission.
> Biographic data
> Age, sex and address
> Method of admission
2. Graphic Flowsheet
- it allows the nurse to record specific measurements on a
repeated basis.
> Vital signs
> Intake and Output
3. Medicine & Treatment record
- allows for the repeated recording of medication and
treatment of the patient on a repeated basis.
109.
4. Nursing Kardex
R– Readily accessible.
E – Ensure continuity of care.
S – Series of flips cards kept at a portable index file at the nurse’s
station.
T – Tool for communication.
2 Parts:
1. Activity and Treatment Section
2. Nursing Care Plan
110.
5. Discharge Summary
-helps ensure that the client’s condition during discharge is in
desirable outcome.
F – Final physical assessment.
I – Instructions about medications and treatment regimen.
R – Record pertinent data.
A – Assess the client support system.
H – Health teaching.
111.
Guidelines of QualityDocumentation and Reporting:
1. Factual
> A record must contain descriptive, objective information
about what a nurses sees, hears, feels and smells.
> The use of vague terms such as appears, seems and
apparently, is not acceptable because these words
suggest that the nurse is stating an opinion.
2. Accurate
> The use of exact measurements establish accuracy .
> Documentation of concise data is clear and easy to
understand.
> It is essential to avoid the use of unnecessary words
and irrelevant details.
112.
3. Complete
> Theinformation within a recorded entry or a report
needs to be complete, containing appropriate and
essential information.
4. Current
> Timely entries are essential in the clients ongoing care.
To increase accuracy and decrease unnecessary
duplication, many healthcare agencies use records kept
near the client’s bedside which facilitate immediate
documentation of information as it is collected from a
client.
5. Organized
> The nurse communicates information in a logical order.
113.
Legal Guidelines forRecording:
Draw single line through error, write word error above it
and sign your name or initials. Then record note correctly.
Do not write retaliatory or critical comments about the
client care by other health care professionals.
Enter only objective descriptions of client’s behavior;
client’s comments should be quoted.
Correct all errors promptly.
Errors in recording can lead to errors in treatment.
Avoid rushing to complete charting, be sure information
is accurate.
Do not leave blank spaces in nurse’s notes.
Chart consecutively, line by line; if space is left, draw
line horizontally through it and sign your name at end.
114.
Record allentries legibly and in blank ink.
Never use pencil, felt pen.
Black ink is more legible when records are photocopied
or transferred to microfilm.
If order is questioned, record that clarification was sought.
If you perform orders known to be incorrect, you are just
as liable for prosecution as the physician is.
Chart only for yourself.
Never chart for someone else.
You are accountable for information you enter into chart.
115.
Avoid usinggeneralized, empty phrases such as “status
unchanged” or ‘had good day”.
Begin each entry with time, and end with your signature
and title.
Do not wait until end of shift to record important
changes that occurred several hours earlier. Be sure to
sign each entry.
For computer documentation keep your password to
yourself.
Maintain security and confidentiality.
Once logged into the computer do not leave the
computer screen unattended.
Nursing Process
- providesthe framework in which nurses use their
knowledge and skills to express human caring and to help
clients meet their health needs.
- a systematic, rational method of planning and providing
care using the process of ADPIE.
Steps:
1. ASSESSMENT
2. DIANOSIS
3. PLANNING
4. IMPLEMENTATION
5. EVALUATION
118.
Characteristics of theNursing Process:
1. Systematic
2. Skills and Knowledge-based
3. Cyclical
4. Dynamic
5. Client-centered
6. Interpersonal and Collaborative
7. Universal
8. Goal-oriented
9. Priority-based
119.
PHASE I:
ASSESSMENT
- isCollecting, Organizing, Validating, and
Recording data about a client’s health status.
Purpose:
- To establish a data base.
120.
4 Types ofAssessment:
1. Initial Assessment
- completed upon admission.
- Ex. Nursing History, Assessment Worksheet
2. Problem-Focused/Ongoing Assessment
- on-going assessment performed during nursing
care.
- Hourly Assessment of Intake and Output
121.
3. Emergency Assessment
-rapid assessment of the patient’s ABC during any
physiologic and psychologic crisis.
- Cardiac Arrest, Suicidal Ideation
4. Time-Lapse Reassessment
- assessment performed in two periods of time.
- Operation Timbang, Assessment for Hypertension
122.
Different Methods ofAssessment:
1. Observation
- gathering data using the 5 senses.
2. Interview
- a planned and purposive conversation between the
nurse and the client.
A. Directive interview:
- “highly structured”
- elicits specific information.
B. Nondirective interview:
- “less structured”
- allows the client to verbalize his thoughts and
feelings.
123.
3 Types ofInterview Questions:
1. Closed-ended
2. Open-ended
3. Leading questions
3. Physical Examination
- systematic data collection method using the
techniques of IPPA.
- objective data are collected.
2 Types of Data:
1. Subjective
- data that are apparent only to the person affected.
2. Objective
- data that can be seen, heard, felt, smelled, or even
tasted.
124.
PHASE II:
NURSING DIAGNOSIS
-is a clinical judgment about individual, family, or
community responses to actual and potential health
problems/life processes.
C – clustering
A – analysis
N – nursing diagnosis formulation
125.
TYPES OF NURSINGDIAGNOSIS:
1. ACTUAL DIAGNOSIS
- judgment about a client’s response to a health problem at the
time of assessment and signified by the presence of associated
signs of symptoms.
Examples:
Fluid volume deficit
Ineffective airway clearance
2. RISK NURSING DIAGNOSIS
- a clinical judgment that a client is more vulnerable to develop the
problem than others in the same situation.
Examples:
Risk for injury
Risk for infection
126.
3. POSSIBLE NURSINGDIAGNOSIS
- evidence about a certain health problem is unclear or the
causative factors are unknown; needs collection of more data
either to support or refute it; not a real type or nursing diagnosis.
Examples:
Possible social isolation
Possible ineffective coping
4. WELLNESS DIAGNOSIS
- is a clinical judgment about an individual, family, or community in
transition from a specific level of wellness to a higher level of
wellness.
Example:
Readiness for enhanced spiritual well-being
127.
COMPONENTS OF ANURSING DIAGNOSIS:
1. Problem
- client’s response to his/her illness.
- ex. Elimination, Breathing pattern, airway clearance
* Qualifiers – words added to give meaning to the
diagnostic statement.
- ex. Decreased, Ineffective, Impaired
2. Etiology
- related factor/probable cause.
3. Signs and symptoms
- defining characteristics.
- evidences or manifestations.
128.
Guidelines for WritingNursing Diagnosis…
1. Word the statement so that is legally advisable.
Example:
Impaired skin integrity related to improper positioning…
2. Make sure that both elements of the statement do not say
the same thing.
Example:
Impaired skin integrity related to skin ulceration.
3. Make sure to use universally accepted abbreviations.
Example:
Ineffective airway clearance related to accu. of secre’ns…
129.
4. Use nursingterminology rather than medical term to describe the
client’s response.
Example:
Ineffective airway clearance related to pneumonia.
5. Use non-judgmental statements.
Example:
Ineffective sexuality pattern related to sexual role confusion.
6. Word the diagnosis specifically and precisely to provide direction
for planning nursing intervention.
Example:
Impaired oral mucous membrane related to noxious
agent.
130.
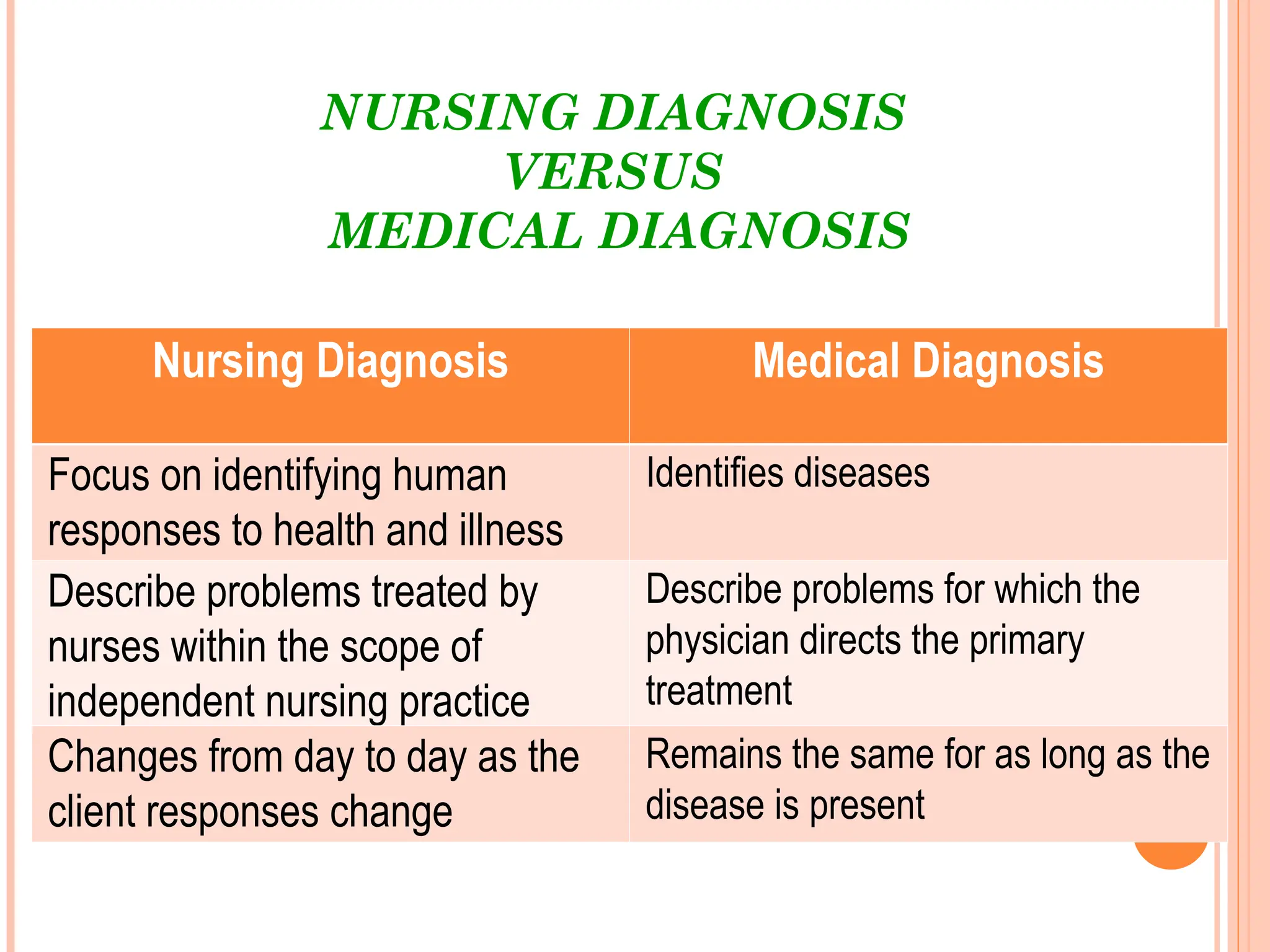
NURSING DIAGNOSIS
VERSUS
MEDICAL DIAGNOSIS
NursingDiagnosis Medical Diagnosis
Focus on identifying human
responses to health and illness
Identifies diseases
Describe problems treated by
nurses within the scope of
independent nursing practice
Describe problems for which the
physician directs the primary
treatment
Changes from day to day as the
client responses change
Remains the same for as long as the
disease is present
131.
PHASE III:
PLANNING
- adeliberative, systematic phase of the nursing
process that involves decision making and problem
solving.
- the nurse refers to the assessment data and the
diagnostic statement.
- the end product is the creation of NCP.
- begins upon the admission and ends when
nurse-patient relationships ends.
132.
PLANNING involves thefollowing activities:
Establishing priorities.
Writing goals/outcomes and developing an evaluate
strategy.
Selecting nursing strategies/interventions.
Developing nursing care plans
Communicate the plan of nursing care.
133.
Types of Planning:
1.INITIAL PLANNING
- the nurse who performs the initial admission assessment
develops the initial comprehensive plan of care; needs
refinements when missing data becomes available.
2. ONGOING PLANNING
- using ingoing assessment data, the nurse carries out
daily planning for the following purposes:
a. to determine whether the client’s health status has
changed
b. to set the priorities for the client’s care during the shift
c. to decide which problems to focus on during the shift
d. to coordinate the nurses’ activities so that more than one
problem can be addressed at each client contact
134.
3. DISCHARGE PLANNING
-the process of anticipating and planning for needs
after discharge; is becoming a crucial part of
comprehensive healthcare. Effective discharge planning
begins at the time of admission where each client is
assessed for:
a. potential health needs
b. availability and ability of the client’s support network to
assist with these needs
c. how the home environment supports the client, and
d. client, family, and community resources
135.
Types of DischargePlanning:
A. Simple/Basic
- patient has been discharged from the agency and
proceeded directly into his/her home.
B. Complex
- patient is discharged from the agency and
returned
to another health care institution.
Setting Priorities
- the process of establishing the preferential
sequence or rank of interventions in accordance to the
client’s most immediate needs.
136.
Nursing Goal/Expected Outcome
-declaration of purposal intention which directs
interventions.
Types of Goals:
1. Short Term
- can be achieved in a short period of time.
2. Long Term
- requires longer period of time to be
accomplished.
137.
PURPOSE of GOALS/EXPECTEDOUTCOMES:
1. Provide direction for planning nursing interventions.
2. Provide a time span for planned activities.
3. Serve as a criteria for evaluation of client progress
4. Enable client and nurse to determine when the problem
has been resolved.
5. Help motivate client and nurse by providing a sense of
achievement.
138.
Guidelines in WritingGoals and Outcomes:
1. The goals must pertain to the client.
2. It should be realistic.
3. It should be compatible with the therapies of other health
professionals.
4. It must be specific.
5. It must be written in behavioral terms.
6. It should be measurable.
7. It should be time-bounded.
139.
Intervention Selection
1. Independent
-nurse-initiated.
Example: Health Teaching, Taking Vital Signs, Making NCP
2. Dependent
- physician-initiated.
- performed under the doctor’s order and
supervision.
Example: Medications, Blood Transfusion, Catheterization
3. Collaborative/Interdependent
- overlapping functions among health care team.
Example: Diet, Laboratory Exams
Nursing Care Plan – “blueprint of the nursing process”
140.
PHASE IV:
IMPLEMENTATION
- isputting the nursing care plan in action.
Activities:
1. Reassessing
2. Set priorities
3. Perform nursing intervention
4. Record actions
Composed of 3 D’s:
1. Doing
2. Delegating
3. Documenting
141.
Doing
* Cognitive Skills– “ intellectual skills”
* Technical Skills – “psychomotor skills”
* Interpersonal Skills – “communication skills”
Activities:
1. Reassessing the client.
2. Prepare the client physically and psychologically.
3. Prepare the equipment and supplies.
4. Implement the interventions.
5. Communicate the nursing actions.
142.
Delegation
- the transferof responsibility or task to a subordinate with
commensurate authority while retaining accountability for
the outcome.
5 Rights to Delegation
1. Right Task
2. Right Circumstance
3. Right Person
4. Right Direction/Communication
5. Right Supervision
143.
Activities that cannotbe delegated:
1. Initial and ongoing assessment.
2. Planning, nursing diagnosis formulation and evaluation.
3. Education and supervision of the nursing personnel.
4. Special activities – like Sterile procedures.
5. Speech and signing of names.
Activities that can be delegated:
1. Routine activities.
- Vital signs taking
- Bed bath
2. Clean procedure.
- Enema
- Ear irrigation
144.
PHASE V:
EVALUATION
- isassessing the client’s response to nursing
interventions and then comparing the response to
predetermined standards or outcome criteria.
Purpose:
To appraise the extent to which goals and
outcome criteria of nursing care have been
achieved.
145.
3 Types ofEvaluation:
1. Ongoing
2. Intermittent
3. Terminal
3 Possible Judgments during Evaluation:
1. Goal met
2. Goal partially met
3. Goal not met
4 Types of Outcome Evaluated:
1. Cognitive
2. Psychomotor
3. Affective
4. Physiologic
146.
Quality Assurance
1. StructureEvaluation
- physical settings, condition through which care is
given.
2. Process Evaluation
- pertains to the manner on how the care was
given.
3. Outcome Evaluation
- pertains to any changes in the client’s health
status
as a result of the nursing intervention.
Chest X-ray
- providesinformation regarding the anatomical
location and appearance of the lungs.
Before X-ray:
> Assess presence of pregnancy.
> Remove jewelries and metals on the client’s chest.
> Instruct the client to inhale and hold breath.
After X-ray:
> Assist the client to dress up.
149.
PULSE OXIMETER:
- devicethat measures O2 saturation level before signs and
symptoms of hypoxemia develops.
> level: 95-100%
> hypoxemia: ↓ O2 in the blood
> brain: most sensitive organ in hypoxia/hypoxemia
(1st
sign: restlessness)
N
150.
2 Types ofPulse Oximeter:
1. Adhesive
2. Clip
> if allergic to adhesive use clip pulse oximeter
> acetone: used to remove nail polish
>alcohol: used if there’s no nail polish
151.
Sites for pulseoximeter:
fingers, ear lobe, nose, and forehead
> how frequent is the changing of site:
● clip: q 2°
● adhesive: q 4-6°
> it is necessary to IMMOBILIZE THE SITE because movements
are detected as pulsation
> if the sun is shining over the pulse oximeter site cover the site.
152.
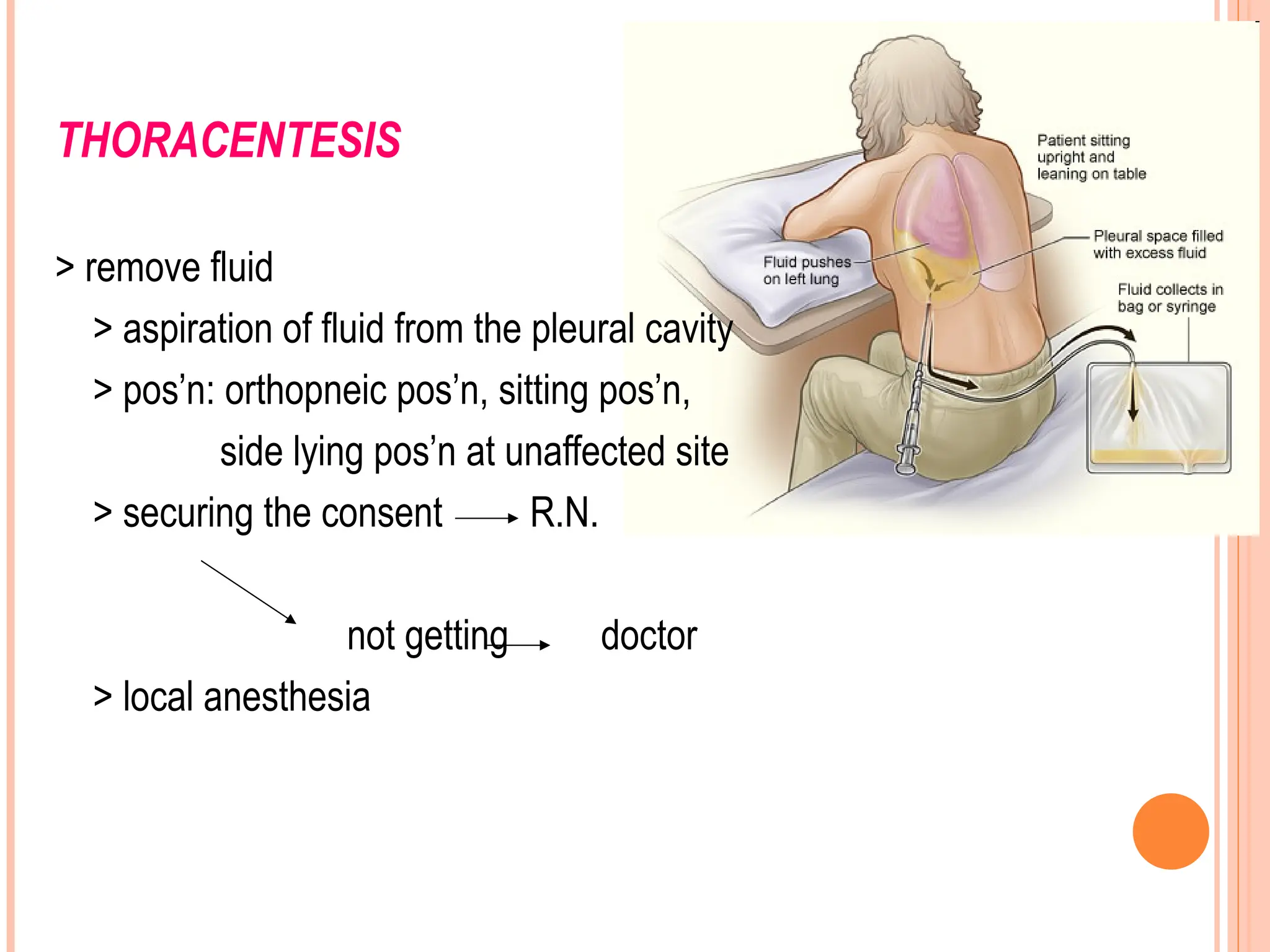
THORACENTESIS
> remove fluid
>aspiration of fluid from the pleural cavity
> pos’n: orthopneic pos’n, sitting pos’n,
side lying pos’n at unaffected site
> securing the consent R.N.
not getting doctor
> local anesthesia
153.
> instruction tothe client during needle insertion &
withdrawal exhale & stay still (take shallow breath)
> after thoracentesis:
position: side-lying (prevent leakage of pleural fluid)
> client coughing red sputum – red tinged saliva Ab
notify the physician ← lung perforation
> after thoracentesis, the doctor will order CXR to rule out
PNEUMOTHORAX
(deadliest complication)
N
154.
CHEST PHYSIOTHERAPY
- dependentnursing action of using positioning,
vibrating, and percussing to remove tenacious respiratory
secretions.
1. Dependent nursing action
- needs doctor’s order to know if the client can tolerate
the procedure.
2. Correct sequence of CPT
Positioning
Percussion
Vibrating
--- POPE VI
155.
3. Gravitational force:force that drains the secretion
4. Positioning
> Orthopneic: to drain secretions from APEX POSTERIOR
SEGMENT
> Trendelenburg, leaning/lying on abd: to drain secretions from
lower lobe posterior segment
5. Position is around 10 mins.
6. Max. time of CPT: 30 mins.
7. Best time in performing postural drainage: early in the morning
upon waking up before meals
*risk for aspiration (same in general anesthesia)
156.
Percussing:
-- striking ofthe skin using a cupped hand like
scooping H2O to dislodge client’s tenacious secretions.
> prevention for reddening: put a layer of cloth
> force come from the wrist
> percuss for 10 mins. (1-2 mins./segment)
> to check if correct: popping/booming sound
157.
Vibration:
-- vigorous quiveringof the heel of the hand
> When to start vibrating using the hand?
- take deep breath then exhale
> Post procedure: cough
#1 Consideration: Toleration of patient to the procedure
Contraindication: Inability to tolerate the procedure
* If the upper lobe of the lungs is affected:
side lying with head ↑ to 30°
R
L
158.
SUCTIONING:
-- removal ofsecretion using a catheter connected to
a suctioning machine.
**suctioning is done as needed (PRN) because it is hassle
& can cause hypoxemia & stimulation of the vagus nerve
> positioning:
conscious: semi-fowler’s
unconscious: side-lying
>lubrication:
nose: sterile, water-based
mouth: PNSS
159.
Measurement for Suctioning:
>oropharyngeal:
- mouth to earlobe
> orotracheal:
- mouth to midsternum
> nasopharyngeal:
- nose to earlobe
> nasotracheal:
- nose to earlobe to neck
* hyperventilate the pt. with 100% O2 before suctioning
* apply suction only during the withdrawal
- to prevent trauma in the mucous membrane.
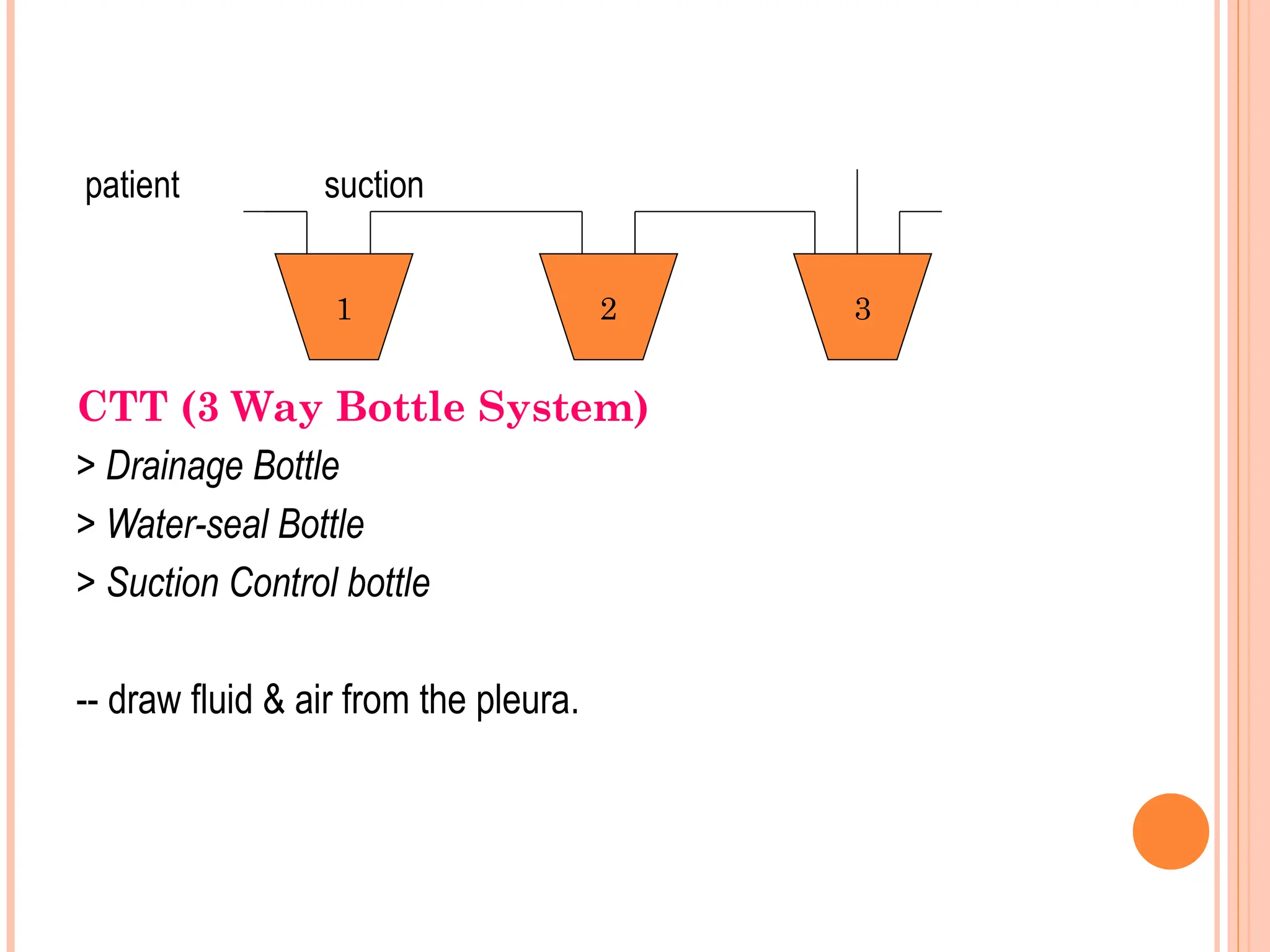
patient suction
CTT (3Way Bottle System)
> Drainage Bottle
> Water-seal Bottle
> Suction Control bottle
-- draw fluid & air from the pleura.
1 2 3
162.
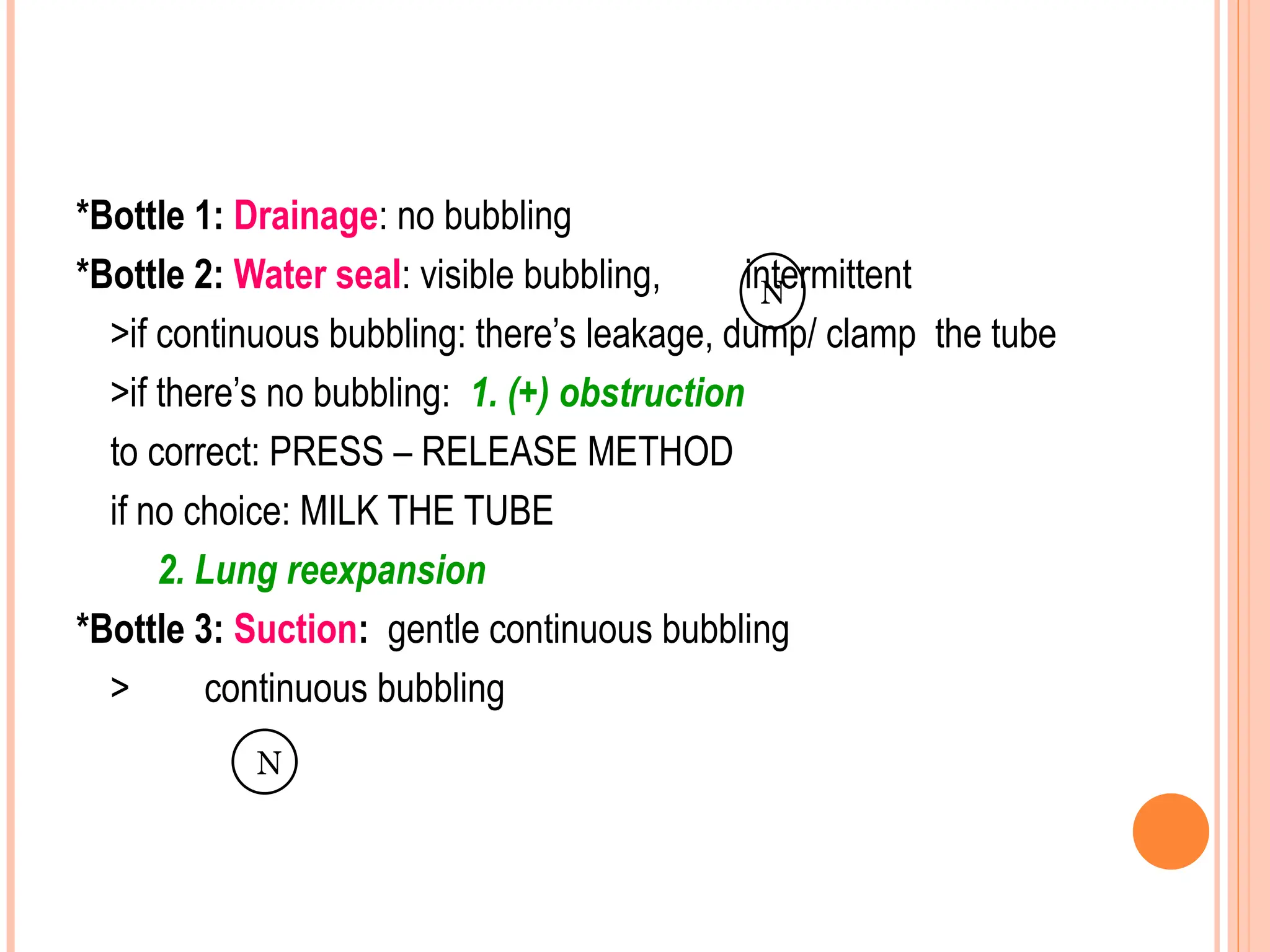
*Bottle 1: Drainage:no bubbling
*Bottle 2: Water seal: visible bubbling, intermittent
>if continuous bubbling: there’s leakage, dump/ clamp the tube
>if there’s no bubbling: 1. (+) obstruction
to correct: PRESS – RELEASE METHOD
if no choice: MILK THE TUBE
2. Lung reexpansion
*Bottle 3: Suction: gentle continuous bubbling
> continuous bubbling
N
N
163.
DISCONNECTION OF TUBE:
A.Chest:
> use vaso-occlusive dressing
> if vaso-occlusive dressing is not available
- use VASELINIZED DRESSING
B. Bottle:
> if still intact:
-- re-insert the tube into the bottle
> if broken:
-- immerse tube in PNSS
** If the tube disconnects : re-insert
164.
Nursing Considerations:
1. Maintainaseptic technique.
2. Palpate for crepitus.
Rationale: To determine presence of subcutaneous emphysema.
3. Minimize clamping and opening of the tube.
Rationale: To prevent pneumothorax.
4. Removal of the chest tube is done by the physician.
Position: Upright position
Instruction: Inhale and hold the breath and then do the
Valsalva maneuver.
N U TR I T I O N
Definition of Terms:
1. Digestion
- the process in which foods are broken down for the body to
use.
2. Absorption
- the process in which digested CHO, CHON, Fats, Water and
Minerals are transported into the blood circulation.
3. Metabolism
- complex chemical process that occurs in a cell in which
nutrients
are utilized for energy source, cell growth and cell repair.
167.
Measures to stimulateappetite:
1. Serve food in a pleasant and attractive manner.
2. Provide comfort.
3. Enhance food with colors.
4. Engage in pleasant conversation.
168.
COMMON THERAPEUTIC DIETS
Clear Liquid Diet
Purpose: Relieve thirst and help maintain fluid balance.
Use: Post-surgically and following acute vomiting of diarrhea.
Foods allowed: Carbonated beverages; coffee (caffeinated and
decaf), tea; fruit-flavored drinks, strained fruit juices,
clear, flavored gelatins; broth, popsicles,
commercially
prepared clear liquids and hard candy.
Foods avoided: Milk and milk products , fruit juices with pulp, and fruit.
169.
o Full LiquidDiet
Purpose: Provide an adequately nutritious diet for patients who
cannot chew or who are too ill to do so.
Use: Acute infection with fever , GI upsets, after surgery as a
progression from clear liquids
Foods allowed: clear liquids, milk drinks, cooked cereals, custard,
ice cream, sherbets, eggnog, all strained fruit juices,
creamed vegetables soups, puddings, mashed
potatoes, instant breakfast drinks, yogurt, mild
cheese sauce or pureed meat, and seasoning.
Foods avoided: nuts, seeds, coconuts, fruit jam and marmalade.
170.
Soft diet
Purpose: Provide adequate nutrition for those who have troubled
chewing.
Use: Patient with no teeth or ill-fitting dentures; transition from full
liquid to general diet and for those who cannot tolerate highly
seasoned, fried or raw foods following acute infections or
gastrointestinal disturbances such as gastric ulcer or
cholelithiasis.
Foods allowed: Very tender minced, ground, baked broiled, roasted,
stewed or creamed beef, lamb, veal, liver, poultry or
fish, crisp bacon or sweat bread; cooked vegetables;
pasta; all fruit juices; soft raw fruits; soft bread and
cereals, all desserts that are soft and cheeses.
171.
Foods avoided:coarse whole grain cereals and bread, nuts;
raisins; coconuts; fruits with small seeds; fried
foods; high fat gravies or sauces; spicy salad
dressings; pickled meat, fish or poultry; strong
cheeses; brown or wild rice; raw vegetables, as
well as lima beans and corns; spices such as
horseradish, mustard, and catsup; and popcorn.
172.
Sodium RestrictedDiet
Purpose: Reduce sodium content in the tissue and promote
excretion of water.
Use: Heart failure, hypertension, renal disease, cirrhosis, toxemia of
pregnancy and cortisone therapy.
Modifications: Mildly restrictive 2g sodium diet to extremely
restricted 200mg sodium diet
173.
Foods avoided:Table salt; all commercial soups, including
bouillon, gravy, catsup, mustard, meat sauces, and
soy sauce; buttermilk, ice cream, and sherbet;
sodas; beet greens, carrots, celery, and spinach; all
canned vegetables; frozen peas
: All baked products containing salt; baking powder, or
baking soda; potato chips and popcorn; fresh or
canned shellfish; all cheeses; smoked or commercially
prepared meats; salted butter or margarine; bacon,
olives and salad dressings.
174.
Renal Diet
Purpose: Control protein, potassium, sodium and fluid levels in the body.
Use: Acute and chronic renal failure, hemodialysis
Foods allowed: - High-biological proteins such as meat, fowl, fish,
cheese and dairy products- range between 20 and
60 mg/day
- Potassium is usually limited to 1500mg/day
- Vegetables such as cabbage, cucumber and peas
are lowest in potassium
- Sodium is restricted to 500 mg/day
- Fluid intake is restricted to the daily volume plus 500 ml, which
represents insensible water loss
- Fluid intake measures water in fruit, vegetables, milk and meat
175.
Foods avoided: Cereals,bread, macaroni, noodles, spaghetti,
avocados, kidney beans, potato chips, raw fruits,
yams, soy beans, nuts, gingerbread, apricots,
bananas, figs, grapefruit, oranges, percolated
coffee, coca-cola, orange crush, sport drinks and
breakfast drinks such as tang or awake.
176.
High Protein,High Carbohydrate Diet
Purpose: To correct large protein losses and raises the level of blood
albumin. May be modified to include low fat, low sodium and
low cholesterol diets.
Use: Burns, hepatitis, cirrhosis, pregnancy, hyperthyroidism,
mononucleosis, protein deficiency due to poor eating habits,
geriatric patient with poor intake, nephritis, nephrosis, and liver
and gall bladder disorder.
Foods allowed: General diet with added protein.
Foods avoided: Restrictions depend on modifications added to the
diet. The modifications are determined by the patient’s
condition.
177.
Purine -Restricted Diet
Purpose: Designed to reduce intake of uric acid- producing foods.
Use: High uric acid retention, uric acid renal stones and gout.
Foods allowed: General diet plus 2-3 quarts of liquid daily.
Foods avoided: Cheese containing spices or nuts, fried eggs, meat,
liver, seafood, lentils, dried peas and beans,
broth,
bouillon, gravies, oatmeal and whole wheat,
pasta,
noodles and alcoholic beverages. Limited
quantities
of meat, fish, and seafood allowed.
178.
Bland Diet
Purpose: Provision of a diet in low fiber, roughage, mechanical
irritants, and chemical stimulants.
Use: Gastritis, hyperchlorhydria (excess hydrochloric acid), functional
GI disorders, gastric atony, diarrhea, spastic constipation, biliary
indigestion and hiatus hernia.
Foods allowed: Varied to meet individual needs and food tolerance
179.
Foods avoided:Fresh foods including eggs, meat, fish, and seafood,
cheese with added nuts, or spices, commercially
prepared luncheon meats, cured meats such as
ham;
gravies; and sauces and raw vegetables
: Potato skins; fruit juices with pulp; figs; raisins; fresh fruits;
whole wheat; rye bread; bran cereals; rich pastries; pies;
chocolate; jams with seeds, nuts, seasoned dressings,
coffee, strong tea, cocoa, alcoholic and carbonated
beverages and pepper.
180.
Low-Fat, Cholesterol RestrictedDiet
Purpose: Reduce hyperlipedimia, provide dietary treatment for
malabsorption syndromes and patients having acute
intolerance for fats.
Use: Hyperlipedimia, atherosclerosis, pancreatitis, cystic fibrosis, sprue
(disease of intestinal tract characterized by malabsorption),
gastrectomy, massive resection of small intestine, and cholecystitis.
Foods allowed: Non-fat milk; low-carbohydrate, low-fat vegetables;
most fruits; breads; pastas; cornmeal; lean meats.
Foods avoided: Remember to avoid the five C’s of cholesterol –
cookies, cream, cake, coconut, chocolate; whole milk or cream
products, avocados, olives, commercially prepared baked
goods such as donuts and muffins, poultry skin, highly marbled meals.
181.
Diabetic Diet
Purpose: Maintain blood glucose as near as normal as possible;
prevent or delay onset of diabetic complications.
Use: Diabetes mellitus
Foods allowed: Choose foods with low glycemic index compose of:
- 45-55% carbohydrates
- 30-35% fats
- 10-25% protein
182.
:Coffee, tea, broth,spices and flavoring can be used as desired.
: Exchange groups include milk, vegetables, fruits, starch/bread,
meat (divided in lean, medium fat, and high fat), and fat exchanges.
:The number of exchanges allowed from each group is dependent on
the total number of calories allowed.
: Non-nutritive sweeteners (sorbitol) in moderation with controlled,
normal weight diabetics.
Foods avoided: concentrated sweets or regular soft drinks
183.
High- fiberDiet
Purpose: Soften the stool
: Exercise digestive tract muscles
: Speed passage of food through digestive tract to prevent
exposure to cancer-causing agents in food
: Lower blood lipids
: Prevent sharp rise in glucose after eating
Use: Diabetes, hyperlipedimia, constipation, diverticulitis,
anticarcinogenics (colon)
Foods allowed: Recommended intake about 6 gms crude
fiber dail : All bran cereal : Watermelon, prunes, dried
peaches, apple with skin, parsnip, peas, brussels sprout,
sunflower seeds.
184.
Low- ResidueDiet
Purpose: Reduce stool bulk and slow transit time.
Use: Bowel inflammation during acute diverculitis or ulcerative colitis,
preparation for bowel surgery, esophageal and intestinal
stenosis.
Foods allowed: Eggs; ground or well cooked tender meat, fish,
poultry; milk; cheeses; strained fruit juices ( except
prune); cooked or canned apples, apricots, peaches,
pears, ripe bananas; strained vegetable juice:
canned or cooked or strained asparagus, beets,
green beans, pumpkin, squash, spinach, white bread,
refine cereals (cream of wheat).
185.
Elimination: URINARY
* Assessingthe urine:
1. Amount per hour
30-60 cc/hr
>60 cc/hr: polyuria
<30 cc/hr: oliguria
anuria: “state of suspension” 0-10 cc/hr
2. Color
> straw, amber, yellow, clear
> hematuria: with blood
> tea colored: hepatitis/dehydration
N
N
186.
3. clarity: clear
>if turbid (cloudy): UTI
4. Odor: aromatic
5. Sterility: sterile
6. pH: acidic (6.0)
7. Specific gravity
> 1.01-1.025 or 1.030
> ↑ specific gravity: greater than 1.030
↑ in particles/solute: dark in color dehydrated
> ↓ specific gravity: less than 1.01
fluid with light: overdehydration, diabetes insipidus
N
N
187.
Collecting Urine Specimenfor C/S:
1. Clean catch: midstream clean catch
> cleaning the urinary meatus
a. Female: use povidone iodine
> wipe front to back
b. Male: use povidone iodine
> circular motion; inner to outer;
hold the penis firmly
2. Collect: 30cc
3. Contaminated after 30 mins.
4. Sterile technique
188.
Urinary Catheter
1. self-sealingrubber catheter:
type of catheter wherein collection can be done
2. wipe the collection part with alcohol
3. 30-45°: angle of needle insertion
4. 30cc of urine for urinalysis: 3cc of urine for C/S
5. if there’s no urine: clamp below the insertion point; 30 mins.
put the syringe above the clamp part
Position:
Female: dorsal recumbent
>knees are flexed & avoid extending knees
Male: supine
Lubricant: sterile water-based
> Female: until urine begins to flow; insert 1-2 inches
further/3-4 inches
> Male: 6-8 inches
During insertion & withdrawal:
> act as if voiding
> exhale
Male: hold the penis 90° against the body
191.
Position in taping:
Female:inner thigh
Male: inner thigh
> abdomen (prevent pressure at scrotum & erection)
*secure the bag at bed frame
*use 5-10cc distilled H2O:
-- pure PNSS can cause precipitate formation &
crystallization.
192.
Elimination: FECAL
*Assessing thestool: color (yellow, brown, greenish)
*For breastfeeding infants, expect a golden yellow stool
> Odor: aromatic
> Amount: 300g to 500g/day
> Frequency: 1-3x/day
1x/2 days
Hirchsprung: at birth, no defecation
> Shape: cylindrical
> Consistency: semi/formed
N
193.
ENEMA
>introduction of asolution to the client’s rectum for 3 purposes:
3 Types According to Purpose:
1. Cleansing enema (cleanse the bowel)
2. Retention (soften & lubricate)
3. Carminative (expel flatus)
2 Types of Cleansing Enema
1. High cleansing enema
> 18 inches (height)
> 1 liter of fluid
> indicated to clean the entire colon
2. Low cleansing enema
> 12 inches (height)
> 500ml of fluid
> from sigmoid to descending colon
194.
> Position:
left sidelying
> Use:
Medical / Cleaning
> Length:
should pass the internal sphincter; 3-4 inches
*if there’s any resistance, never force the obstruction
> to relax:
inhale
> If client experience cramping & pain:
clamp for 30 mins.
** rectal suppository: 3-4 inches
DRUGS
IV = mL/hrhours = mL
gtts/min
Drugs: > D x Q
S * “U 40” = 40 units/mL
> D = SxQ
> S = D/Q
Drop Factor:
IV= vol(mL) x drop factor > Adult: 15
hrs > Pedia: 60
ordered amount of drug = unknown quantity needed (X)
amount of drug on hand known quantity of drug
198.
Sample Computation:
Dosage calculationfor units (some medications such as heparin and
penicillin are ordered in units)
1. The order is penicillin 750,000 units. The vial reads 300,000
units/2mL. How many mL will be given?
2. Ordered amount of drug is 750,000 units;
amount of drug on hand is 300,000 units.
3. Unknown quantity is X; known quantity is 2 mL
199.
4. Calculations:
a. 750,000units = X
300,000 units 2mL
b. (300,000 units) (X) = (750,000 units) (2mL)
c. 300,000 X = 1,500,000
3,000,000 units 300,000
d. X = 150
30
e. X = 5 mL
200.
Administration of Medication:
Medication
-a substance administered for diagnosis, cure, treatment, relief or
prevention of disease.
- also called drug.
Effects of the Drug.
1. Therapeutic effect – primary effect/positive effect.
2. Side effect – secondary effect/negative effect/unintended effect.
3. Drug tolerance – usually low physiologic response to a drug which
requires additional dosage to achieve the desired effect.
4. Drug abuse – inapropriate use of the drug either continually or
habitually.
5. Drug dependence – client’s reliance on the drug.
201.
Principles in AdministeringMedications
1. Observe the 10 “rights” of drug administration.
1. Right Medication
2. Right Dosage
3. Right Client
4. Right Time
5. Right Route
6. Right Documentation
7.
8.
9.
10.
202.
2. Practice asepsis;wash hands before and after preparing medications.
3. Be knowledgeable and accountable about the medications that you
administer.
4. Before administering the medication, identify the client correctly.
5. Do not leave the medication at bedside.
6. The nurse who prepares the drug administers it.
7. If the client vomits, report this to the nurse in-charge or physicians.
8. When a medication error is made, assess the client and report it
immediately to the nurse in charge or physician.
203.
Routes of Drug
ORAL
Advantages:
1.Most accessible
2. Safe
3. Cost effective
Disadvantages:
1. Inappropriate for client with nausea and vomiting.
2. Inappropriate for client’s with difficulty of swallowing.
3. Inappropriate for patient’s with decrease gastric motility.
4. May have unpleasant taste or discolor the teeth.
5. May cause aspiration.
204.
Different Forms ofOral Medications:
1. Solid – tablet, capsule, pills, caplet, powdered
2. Liquid
> Syrup – sugar-based > Emulsion – oil-based
> Suspension – water-based > Elixir – alcohol-based
* Allow 30 minutes to elapse before giving a glass of water.
3. Sublingual
4. Buccal
5. Rectal
6. Vaginal
7. Topical
8. Transdermal
205.
Parenteral Routes
1. Intradermal
Advantage:slow absorption rate, used for drug testing.
Disadvantage: requires sterile technique, causes anxiety, can only
administer small amount of drug.
Sites: inner forearm, anterior chest, underneath of the scapula
Angle of needle: 10-15 angle, almost parallel to the skin
Gauge: 25, 26, 27
Length: 3/8, 5/8, ½ inch
Maximum cc: 0.1cc to 0.2cc
206.
2. Subcutaneous
Advantage: fasterthan oral routes.
Disadvantage: expensive, requires sterile technique, slower than IM
and IV, can cause anxiety, some drugs can cause pain and
irritation, breaks the client skin integrity.
Sites: upper arm, outer thigh, abdomen, ventrogluteal, dorsogluteal
Angle of needle: 45 angle; obese and insulin administration - 90 angle
Gauge: 25, 26, 27
Length: 3/8, 5/8, ½ inch
Maximum cc: 1-3 ml
207.
3. Intramuscular
Advantage: fasterabsorption, can reduce pain and irritation from
irritating drugs.
Disadvantage: requires sterile technique, can cause anxiety, it breaks
the client’s skin integrity
Sites: ventrogluteal, dorsogluteal, vastus lateralis, rectus femoris, deltoid
Angle of needle: 90 angle
208.
Z-track…
> retract theskin laterally away from the site
> pierce the skin quickly and smoothly at 90
> aspirate (5-10cc)
> inject the drug slowly and steadily (10 sec/ml)
> wait for 10 secs and allow the medication to disperse
> do not massage
209.
3. Intravenous
Advantage: rapideffect
Disadvantage: limited for highly soluble solutions only, poor circulation
can interfere absorption
** Intravascular
Gauge: 24, 23, 22, 21, 20
Length: 1, 1 ½, 2 inches
Maximum cc: IV push – 10 ml
IV infusion – 4L per day
> Unit ofblood = depends on agency
- 450 cc, 500 cc, 250 cc, 240 cc
> PNSS:
- only fluid compatible during BT
> gauge: 19, 18, 17, 16
> ↓ bacteria; administered within 30 mins.
> max. time: 4 hours
> RN to check: 2 RN
> if blood is too cold:
- cover the blood with a dry cloth
212.
> best wayto check client’s identity before transfusion
- through ID Band/bracelet
> mix the bag of blood by tilting the blood from side to side
> Adverse reaction: during the first 20 mins
(15 mins) at 20 gtts/min
> S/Sx of adverse rxn:
- itchiness, hives, ↑ temp., chills, fever, & pain.
1st
adverse rxn: dizziness/headache
IV: STOP, RUN PNSS, NOTIFY THE DOCTOR
- bring blood to the laboratory
- get a urine specimen