Download to read offline
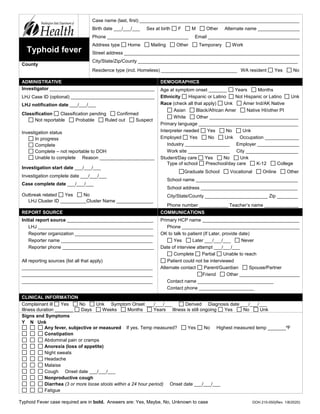
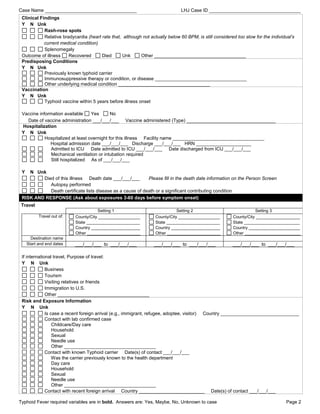





1. This document contains a case report form for investigating and reporting cases of typhoid fever. It requests demographic, clinical, and exposure information about a case. 2. The form includes sections on administrative details, clinical information, risk factors and exposures, and food and water sources. It asks about travel history, contacts with other cases or carriers, and food consumed both in and outside the home. 3. Key information requested includes symptoms, hospitalization details, vaccination history, potential exposures 3-60 days prior to onset, and sources of drinking water.



























































