This document provides an agenda for a webinar hosted by the Khazanah Research Institute (KRI) on Malaysia's health system. The webinar will include a presentation of KRI research findings on Malaysia's health system by panelists from KRI, followed by commentary from Dato' Prof. Dr Adeeba Kamarulzaman of Universiti Malaya. Tan Sri Nor Mohamed Yakcop, Chairman of KRI, will then give a speech and there will be a question and answer session, concluding the webinar at 3:30pm.







![Khazanah
Research
Institute
14
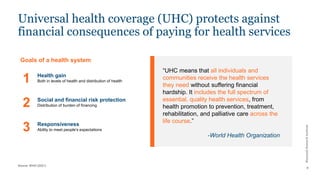
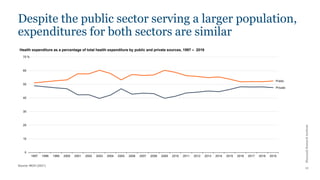
The government has repeatedly indicated that it
intends to reduce public financing for healthcare
“With increasing demand by the
population for healthcare, coupled with
rising public expectations the real
challenge will, therefore, be to find
ways and means to meet the rising cost
of providing healthcare. In view of this,
new sources of finance must be
identified.”
—5th Malaysia Plan
“Rising healthcare costs have
threatened the financial sustainability of
the Government in providing quality
public healthcare.”
“A comprehensive revitalisation of the
country’s healthcare system aims…[to]
Reduce the high level of subsidies,
unsustainable healthcare
financing…”
—12th Malaysia Plan](https://image.slidesharecdn.com/20211215healthwebinarv1-231106104118-4ce555c2/85/20211215_Health-Webinar_v1-pdf-14-320.jpg)