Download to read offline
![NY Times article 12/22/09The Obama Administration’s former director of the Office of Management and Budget, Peter Orzag, attacked the fact that the Ronald Reagan University of California at Los Angelos [UCLA] Medical Center spends more than Rochester, Minnesota's Mayo Clinic.](https://image.slidesharecdn.com/2011obamacarerepealconvgensess-110628154542-phpapp01/85/Denial-of-Life-Saving-Medical-Treatment-in-the-Obama-Health-Care-Law-38-320.jpg)
![NY Times article 12/22/09BUT: “[T]he hospital that spent the most on heart failure patients had one-third fewer deaths after six months of an initial hospital stay.”Difference between looking forward and looking back](https://image.slidesharecdn.com/2011obamacarerepealconvgensess-110628154542-phpapp01/85/Denial-of-Life-Saving-Medical-Treatment-in-the-Obama-Health-Care-Law-40-320.jpg)


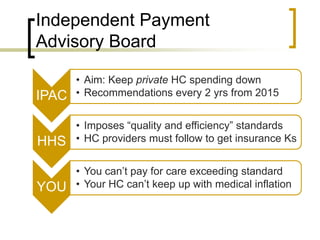



The document discusses rationing in the Obama health care law through several mechanisms: 1. The Independent Payment Advisory Board will limit Medicare funding growth and empower HHS to impose uniform standards of care. Doctors who exceed these standards risk losing insurance contracts. 2. Medicare limits and restrictions on supplemental private insurance will constrain health care options for seniors. 3. Insurance exchange limits will exclude plans deemed to allow "excessive" private spending on health care. 4. "Shared decisionmaking" groups receiving federal funds will influence treatment choices through decision aids emphasizing less or more conservative care. The document argues these constitute involuntary rationing and constraints on individual choices, despite claims greater efficiency can avoid rationing












































































