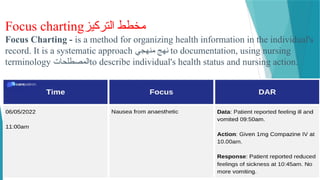
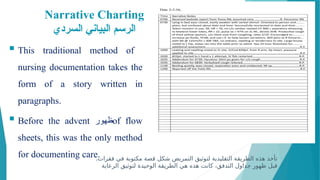
The document discusses the importance of documentation in therapeutic communication within nursing practice, highlighting its role in professional responsibility, communication, education, and legal standards. It covers various aspects of documentation, including its use in client care, research, informed consent, and advanced directives, while also outlining effective documentation practices and methods. Additionally, the document emphasizes the significance of accurate record-keeping for reimbursement and accreditation, detailing different documentation methods such as narrative and focus charting.

















![Director of Nursing (DON)]د حاتم البيطار زويل اكاديمي.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/directorofnursingdon-240225223408-af5cc019-thumbnail.jpg?width=640&height=640&fit=bounds)





















































