Download to read offline

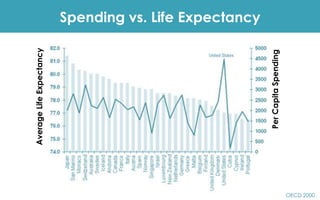

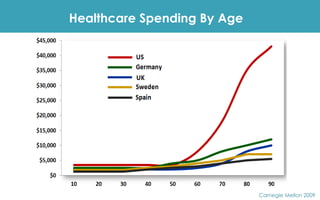

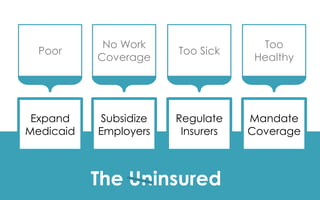


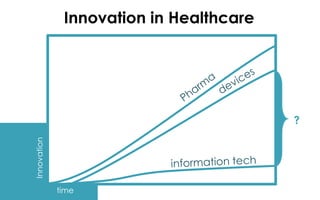


















The document discusses healthcare spending versus life expectancy, highlighting issues like wasteful spending and the challenges faced by uninsured populations. It mentions innovations in healthcare, such as technology adoption and initiatives to improve patient care while managing financial risk. Additionally, it outlines current projects aimed at creating healthier communities and improving healthcare access.



































































