Downloaded 17 times










![catalyst.nejm.org
10 Paths to Innovation in Health Care Delivery 13
Return to TOCReturn to TOC
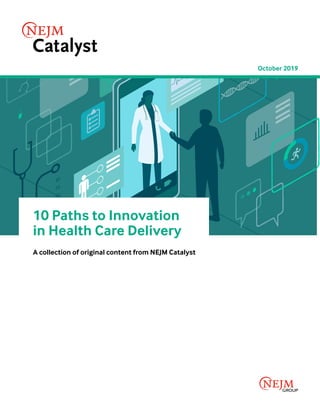
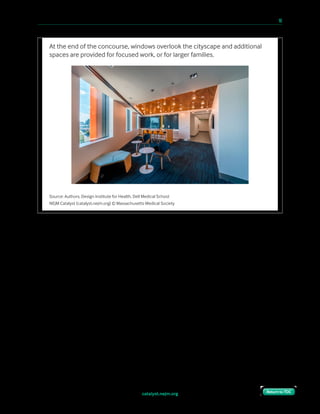
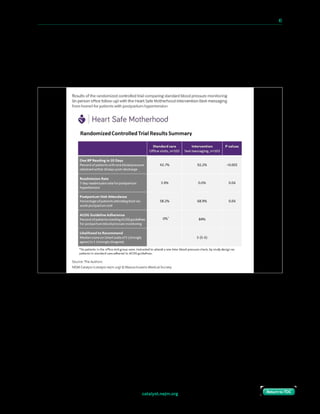
“What if we lose the patient?”
We had always planned to greet patients as soon as they arrived in the building (at the garage
or pedestrian entrance), do a lightweight check-in (name and appointment), and then
immediately assign them to a room. Not unlike in a hotel or other hospitality experience, we
expected they would have no issue taking the elevator to the right floor, and then finding
their way to their room.
As we developed the check-in protocol, members of the operations staff raised a concern:
What if patients got lost on the way to their room? We couldn’t track them in between check-
in and arrival, so there was a chance they might fall off our radar. Wouldn’t a waiting room
model work better, because we’d always know where they were?
We believed that the options under consideration represented
a false choice between “enforce sequestration” or “leave them
to unguided autonomy.” A third option, guided autonomy,
could get them where they needed to go through the use of
thoughtful design.
The building was set up for real-time location services using
RFID technology. Eventually, we planned to give each patient a
tag to track their progress through the building, but we had to
delay the deployment of that capability in order to focus on
other priorities more critical to the clinic launch.
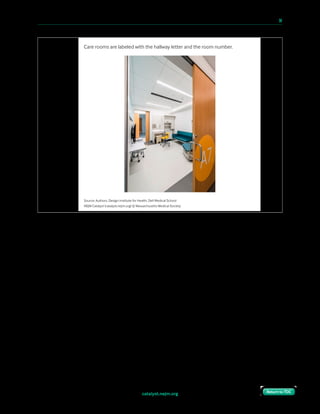
In the interim, we developed a paper-based protocol, with
human backup. We had already developed a straightforward
wayfinding scheme: Floors were labeled with numbers,
hallways with letters, and then rooms with a second number. At arrival, each patient was
given a “boarding pass” with their room assignment.
We believed that
the options under
consideration represented
a false choice between
‘enforce sequestration’
or ‘leave [patients] to
unguided autonomy.’
A third option, guided
autonomy, could get
them where they needed
to go through the use of
thoughtful design.”](https://image.slidesharecdn.com/10-paths-to-innovation-in-health-care-delivery-190918125717/85/10-Innovation-Pathways-Care-Delivery-16-320.jpg)


























![10 Paths to Innovation in Health Care Delivery 49
An example of a well-designed health care delivery process at your organization.
“Screening all aspects of patient factors (physical, psychological,
financial, social, cultural) and building it to a support system. Assign
experts as a care team to work with all issues and communicate well.
Build a system for appropriate referrals to utilize resources.”
— Clinician at a large nonprofit community hospital
in the South
“Electronic tracking systems (home grown) to identify, track, and
communicate to patients with incidental lung nodules on CT scan
who need to return for follow up scans. Similar system is in place for
patients in the lung cancer screening program. The systems are driven
by the radiologists, who systematically apply the Fleischner guidelines
(or L-RADs for cancer screens) for follow up imaging based on nodule
size and quality.”
Department chief at a midsized nonprofit teaching hospital
in the West
“Color coded system in computer for nurses and physicians so we
both can see where the patient is regarding the visit. In room, needs
labs, needs vaccines, awaiting paperwork, signing out, etc…”
— Director of a large nonprofit health system in the Midwest
“Following 3 inpatient patient deaths involving root causes of poor
communication, silo’d cultures of practice and accountability, a formal
patient safety program was designed that delineated responsibility and
chain of command. A great deal [of] systems level thinking occurred
by hospital leadership and frontline clinical/ operational staff to link
departments, develop processes to empower personnel and reward
successful improvements.”
— Clinician at a small nonprofit teaching hospital in the Northeast
VERBATIM COMMENTS FROM SURVEY RESPONDENTS
Return to TOCReturn to TOC
(CONTINUED ON NEXT PAGE)](https://image.slidesharecdn.com/10-paths-to-innovation-in-health-care-delivery-190918125717/85/10-Innovation-Pathways-Care-Delivery-52-320.jpg)



![catalyst.nejm.org
10 Paths to Innovation in Health Care Delivery 55
Return to TOCReturn to TOC
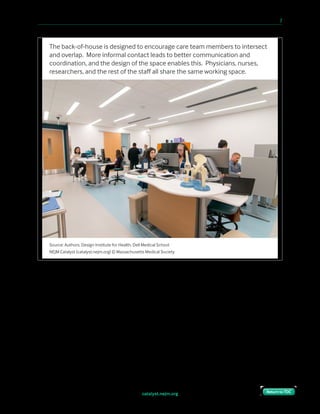
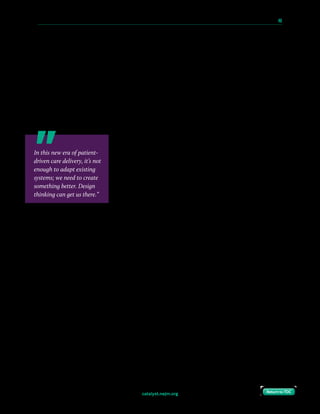
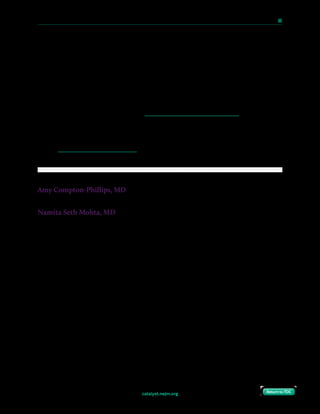
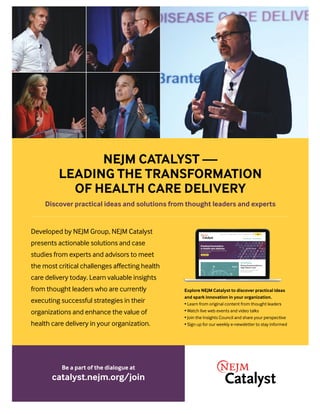
While respondents are nearly unanimous about the usefulness of design thinking in health
care, the frequency of using design principles and techniques does not reflect this. Two-
thirds of Council members say their organizations employ design principles occasionally,
seldom, or never. One clinical leader says family medicine is resistant to design thinking and
“stuck in the old model because clinicians don’t trust that a different model won’t decrease
their income.” Another clinical leader is more positive, saying, “We had an excellent design
period that focused on patient intake and flow [in the emergency department] with attention
to flow to CT, ICU, and surgery.”
Health Care Organizations Only Occasionally Apply Design Thinking
How oen does your organization actively employ principles/techniques of design thinking?
Base = 625
NEJM Catalyst (catalyst.nejm.org) © Massachusetts Medical Society
Always
Mostly
Occasionally
Seldom
Never
Not sure
4%
20%
39%
21%
7%
9%
Consensus That Design Thinking Is Useful in Health Care
How useful is design thinking for your organization? For health care delivery in general?
Base = 625
NEJM Catalyst (catalyst.nejm.org) © Massachusetts Medical Society
Organization
Extremely useful Very useful Useful Not very useful Not at all useful
Health care
industry
36%
44%
29%
29%
26%
22%
91%
95%
6%
4%](https://image.slidesharecdn.com/10-paths-to-innovation-in-health-care-delivery-190918125717/85/10-Innovation-Pathways-Care-Delivery-58-320.jpg)








![catalyst.nejm.org
10 Paths to Innovation in Health Care Delivery 66
Return to TOCReturn to TOC
Still, this change is by no means universal and significant
variation exists. Some of these programs are embedded in a
specific residency program (e.g., internal medicine). Some are
part of an institutional program offered to all residency
programs. Some require an additional year of training; some
are only available to residents, not fellows; some are available
only to individuals with previous formal business training.
Several of these programs pair trainees with a leader-mentor,
who can help the trainee learn how best to present new ideas
to health system leaders. Leaders can encourage participation
in these tracks by portraying them as equally valuable as more
traditional pathways (such as basic science or translational
research), and by designing a clear pathway for advancement within the organization
following completion of training.
Collaborate with a Health Care Start-Up
Physicians-in-training can learn much from collaboration with a start-up, and leaders need
to facilitate such relationships. Start-ups offer agile and innovative approaches to issues of
care delivery, cost reduction, and patient engagement. Start-ups rapidly and repeatedly
modify products and methods in response to input from individuals in the target field with
the goal of defining utility early. Start-ups can expose postgraduate trainees to principles of
leadership that may be directly applicable to leading ward teams and teams of health care
providers in organizations after training.
A key feature shared by great leaders is having a diverse personal and professional stakeholder
network, as this enables leaders to engage people who think differently than their typical
associates. In a complex world with increasing transparency, relying on traditional
development practices will stunt a leader’s growth. Furthermore, changes in health care
systems often impact stakeholders in the three major sectors of health care (private, public,
and nonprofit) — an understanding of the private sector through collaboration with a start-
up can foster an understanding of different frameworks for innovation and different
stakeholder objectives. By collaborating with physicians-in-training, start-ups gain diversity
of thought and insight into the workings of a field that they might otherwise lack. Compared
to established faculty, trainees are still relative outsiders, and can offer fresh perspectives.
Trainees may see start-up work as part of their future career, and thus may have more
motivation to contribute.
[Physicians-in-training]
have great potential to
drive improvement in
the health care system.
However, established
pathways for fostering the
frameworks necessary to
utilize these talents remain
uncommon, and may be
ill-defined or circuitous.”](https://image.slidesharecdn.com/10-paths-to-innovation-in-health-care-delivery-190918125717/85/10-Innovation-Pathways-Care-Delivery-69-320.jpg)








This document discusses innovative approaches to health care delivery, focusing on how health care leaders can generate innovation internally rather than relying exclusively on external sources. It emphasizes the importance of redesigning patient experiences, such as eliminating waiting rooms and implementing integrated practice units for improved outcomes and patient satisfaction. The collection includes case studies and insights on applying design thinking and technology to enhance care delivery across various health care settings.



















































































