Dr Mekuanint D.(OBGY year II Resident )
Modulator: Dr Tizita (OBGY Consultant)
Yekatit 12 HMC/Abebech Gobena /
April,2021
Management of preeclampsia and
Eclampsia
INTRODUCTION
Preeclampsia isa multisystem, progressive disorder
characterized by
new onset of hypertension and proteinuria or
hypertension and end-organ dysfunction with or without
proteinuria in the last half of pregnancy
A key focus of routine prenatal care is monitoring
pregnancies for signs and symptoms of preeclampsia.
3
4.
Incidence
Most commonmedical complications of pregnancy
5% and 10%
5 percent in white, 9 percent in Hispanic, and 11 percent in
African-American women
4
5.
Classification
Preeclampsia andeclampsia syndrome
Chronic hypertension of any etiology
Preeclampsia superimposed on chronic hypertension
Gestational hypertension
5
ETIOPATHOGENESIS
Develop in womenwith the following characteristics:
exposed to chorionic villi for the first time
exposed to a superabundance of chorionic villi, as with twins or hydatidiform
mole
preexisting conditions associated with endothelial cell activation or
inflammation,
diabetes,
obesity,
cardiovascular or renal disease,
immunological disorders, or
hereditary influences
genetically predisposed to hypertension developing during pregnancy.
11
12.
A fetusis not a requisite for preeclampsia to develop.
although chorionic villi are essential, they need not be
intrauterine.
12
13.
…Etiology
Placental implantationwith abnormal trophoblastic invasion of
uterine vessels
Immunological maladaptive tolerance between maternal,
paternal (placental), and fetal tissues
Maternal maladaptation to cardiovascular or inflammatory
changes of normal pregnancy
Genetic factors including inherited predisposing genes and
epigenetic influences.
13
…Pathogenesis
Regardless ofprecipitating etiology,
cascade,
systemic vascular endothelial damage with resultant
vasospasm,
transudation of plasma,and
ischemic and
thrombotic sequelae
15
16.
Management
Management variesdepending
gestational age
severity
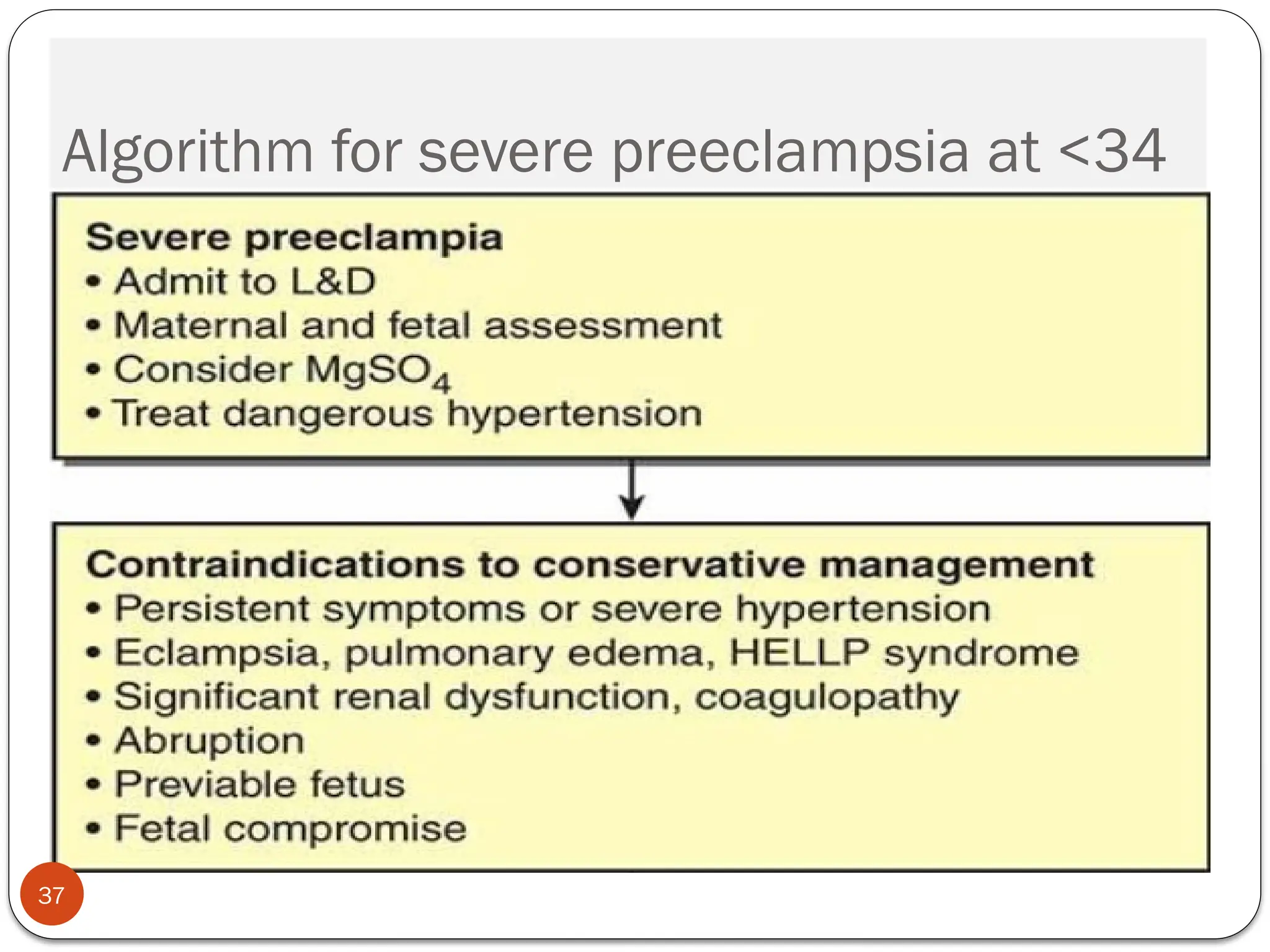
Preeclampsia with features of severe disease
<28 week –Termination
28-34 week-expectant management is recommended
34-37 week--expectant management may be recommended
16
Treatment of hypertension
Severe hypertension should be treated to prevent maternal
vascular complications (eg, stroke, heart failure)
systolic pressure is ≥160 mmHg or diastolic pressure is ≥105
to 110 mmHg
18
19.
Choice of drugand dose
two settings
Acute management of severe hypertension, which may require
parenteral therapy, and
Longer-term blood pressure control during expectant
management of severe preeclampsia
19
Labetalol
effective, hasa rapid onset of action, and a good safety
profile.
Begin with 20 mg intravenously over 2 minutes followed at
10-minute intervals by doses of 20 to 80 mg up to a
maximum total cumulative dose of 300 mg, if blood pressure
remains above target level
A constant infusion of 1 to 2 mg/min can be used
The fall in blood pressure begins within 5 to 10 minutes and
lasts from 3 to 6 hours
21
22.
Hydralazine
5 mgintravenously over 1 to 2 minutes
If a total dose of 30 mg does not achieve optimal blood
pressure control, another agent should be used.
The fall in blood pressure begins within 10 to 30 minutes and
lasts from 2 to 4 hours.
22
23.
Calcium channelblockers
Nifedipine
30 mg sustained release tablet
Nitroglycerin
hypertension associated with pulmonary edema
It is given as an intravenous infusion of 5 mcg/min and
gradually increased every 3 to 5 minutes to a maximum dose of
100 mcg/min.
23
24.
Long-term oral therapy
Nifedipine
Alpha methyldopa
•Administer 250-750 mg every six to eight hours.
The maximum dose is 3000 mg per 24 hours
24
25.
Seizure prophylaxis
Candidatesfor seizure prophylaxis
Intrapartum and postpartum seizure prophylaxis to all women
with preeclampsia,
Drug of choice:
Magnesium sulfate
25
26.
Dosing
loading doseof 6 g of a 10 percent solution intravenously
over 15 to 20 minutes followed by 2 g/hour as a continuous
infusion
5 g of a 50 percent solution intramuscularly into each
buttock (total of 10 g) followed by 5 g intramuscularly every
four hours
therapeutic range of 4.8 to 8.4 mg/dL (2.0 to 3.5 mmol/L)
26
27.
Renal insufficiency
Magnesium sulfate is excreted by the kidneys.
Women with renal insufficiency should receive a standard
loading dose
Reduced maintenance dose.
1 g/hour if the serum creatinine is >1.2 and <2.5 mg/dL
no maintenance dose if the serum creatinine is ≥2.5 mg/dL or
magnesium toxicity is suspected
27
28.
Timing of Magnesiumsulfate
at the onset of labor or induction, or prior to a cesarean
delivery
while they are being considered for conservative
management.
Prolonged antepartum therapy??
28
29.
Side effects
Rapidinfusion of magnesium sulfate causes peripheral
vasodilation and a drop in blood pressure.
diaphoresis
flushing, and
warmth
Nausea
vomiting
29
headache
muscle weakness
visual disturbances, and
palpitations
30.
Transient reductionof total and ionized serum calcium
concentration due to rapid suppression of parathyroid
hormone release
30
31.
Toxicity
Magnesium toxicityis uncommon in women with good renal
function
loss of deep tendon reflexes occurs at 7 to 10 mEq/L
respiratory paralysis at 10 to 13 mEq/L
cardiac conduction is altered at >15 mEq/L
cardiac arrest occurs at >25 mEq/L
31
32.
When to checkmagnesium levels
every six hours
A seizure while receiving magnesium sulfate
Clinical signs/symptoms suggestive of magnesium toxicity
Renal insufficiency (creatinine >1.2 mg/dL [106 micromol/L)
32
Preterm pregnancies:
Conservativemanagement
the risks of serious sequelae from disease progression need to
be balanced with the risks of preterm birth
34
35.
Indications for Deliveryin Women <34
Weeks
Uncontrolled severe hypertension
Eclampsia
Pulmonary edema
Disseminated intravascular coagulation
Placental abruption
Nonreassuring fetal status
Fetal demise
35
36.
Corticosteroid—Delay Delivery 48hr
Preterm ruptured membranes or labor
Thrombocytopenia <100,000/μL
Hepatic transaminase levels twice upper limit of normal
Fetal-growth restriction
Oligohydramnios
Reversed end-diastolic Doppler flow in umbilical artery
Worsening renal dysfunction
36
Eclampsia :
40
Developmentof convulsions or unexplained
coma during pregnancy or postpartum in
patients with signs and symptoms of PE.
Excluding other posible cause of convulsion
41.
Incidence
41
1 in2000 to 1 in 3448 pregnancies.
2-3 % in PE with SF
0.6% in PE without SF
higher in
tertiary referral centers
Multifetal gestation
in those without prenatal care
42.
Pathophysiology
42
The precisecause of seizures in preeclamptic women is not
clearly understood.
1. hypertension causes a breakdown of the autoregulatory
system of the cerebral circulation,
hyperperfusion,
endothelial dysfunction, and
vasogenic and/or cytotoxic edema.
43.
Pathophysiology…
43
2. hypertension causesactivation of the autoregulatory system,
leading to vasoconstriction of cerebral vessels
hypoperfusion,
localized ischemia,
endothelial dysfunction, and
vasogenic and/or cytotoxic edema
44.
CLINICAL PRESENTATION ANDFINDINGS
44
generalized tonic-clonic seizure or coma
premonitory signs/symptoms
Hypertension (75 percent)
Headache
Visual disturbances (27 percent)
Right upper quadrant or epigastric pain (25 percent)
Asymptomatic (25 percent)
Diagnosis …
46
Severalclinical symptoms are potentially helpful
persistent occipital or frontal headaches,
blurred vision,
photophobia,
epigastric or right upper quadrant pain, and
altered mental status.
47.
Time of Onset
47
Antepartum …
Intrapartum
postpartum period.
first 48 hours
beyond 48 hours
extensive neurologic evaluation may be required to rule out the
presence of other cerebral pathology
48.
Time of Onset…
48
Almost all cases of eclampsia (91%) develop in the third
trimester (≥28 weeks).
21 and 27 weeks’ gestation (7.5%)
before 20 weeks’ gestation (1.5%)
49.
MANAGEMENT
49
maintaining airwaypatency and preventing
aspiration
The woman should be rolled onto her left side.
Prevention of maternal hypoxia and trauma
Treatment of severe hypertension
Prevention of recurrent seizures
Evaluation for prompt delivery
50.
Treatment of hypertension
50
To prevent stroke, which accounts for 15 to 20 percent of
deaths from eclampsia.
diastolic pressures greater than 105 to 110 mmHg or
systolic blood pressures ≥160 mmHg
Drugs
Hydralazine
Labetalol
Nifidipine
51.
51
Diuretics
Potent loopdiuretics can further compromise placental
perfusion.
before delivery, diuretics are not used to lower blood
pressure
52.
Prevention of recurrentseizures
52
Treatment is primarily directed at prevention of recurrent
seizures and the possible complications
10 percent of eclamptic women will have repeated seizures
The anticonvulsive drug of choice is magnesium sulfate.
53.
53
Loading dose
4to 6 g intravenously are commonly used
5 g intramuscularly into each buttock for a total of 10 g;
the onset of a therapeutic effect will be slower and
intramuscular injection is painful.
These loading doses may be given safely to patients with
renal insufficiency.
54.
54
Maintenance dose
1to 3 g/hour are commonly used.
5 g can be given intramuscularly every four hours;
a lower dose maintenance regimen (2.5 g intramuscularly
every four hours)
The maintenance phase is given only if a
patellar reflex
respirations are greater than 12 per minute, and
urine output is over 100 mL in four hours
55.
Management of persistentseizures
55
Additional bolus of 2 g magnesium sulfate over 5 to 10
minutes
Frequent monitoring for signs of magnesium toxicity
If two such boluses do not control seizures, then other drugs
should be given.
Diazepam or lorazepam is a common choice
56.
Response to therapy
56
Women who do not improve within 10 to 20 minutes
following control of hypertension and seizures and
those with neurologic deficits
should be evaluated by a neurologist
may have ongoing nonconvulsive seizures or
underlying structural pathology,
such as hemorrhage
57.
Evaluation for promptdelivery
57
Contraindication to expectant management
The definitive treatment for eclampsia
prompt delivery;After maternal stabilization,
58.
58
mode ofdelivery
gestational age
cervical status
whether the patient is in labor, and
fetal condition and position
Prevention
60
use ofantihypertensive
timely delivery, and
prophylactic use of magnesium sulfate during labor and
immediately postpartum in those considered to have PE
61.
Reference
61
William’s obstetrics,25th
ed.
Gabbe obstetrics, 7th
ed.
Up to date 2018
ACOG PRACTICE BULLETIN
MANAGEMENT PROTOCOL ON
SELECTED OBSTETRICSTOPICS FOR
HOSPITALS, Ministry of Health Ethiopia,2020


















































































![9_hypertension_(1)_(3)[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/9hypertension131-230607084247-9b815ae1-thumbnail.jpg?width=640&height=640&fit=bounds)
































