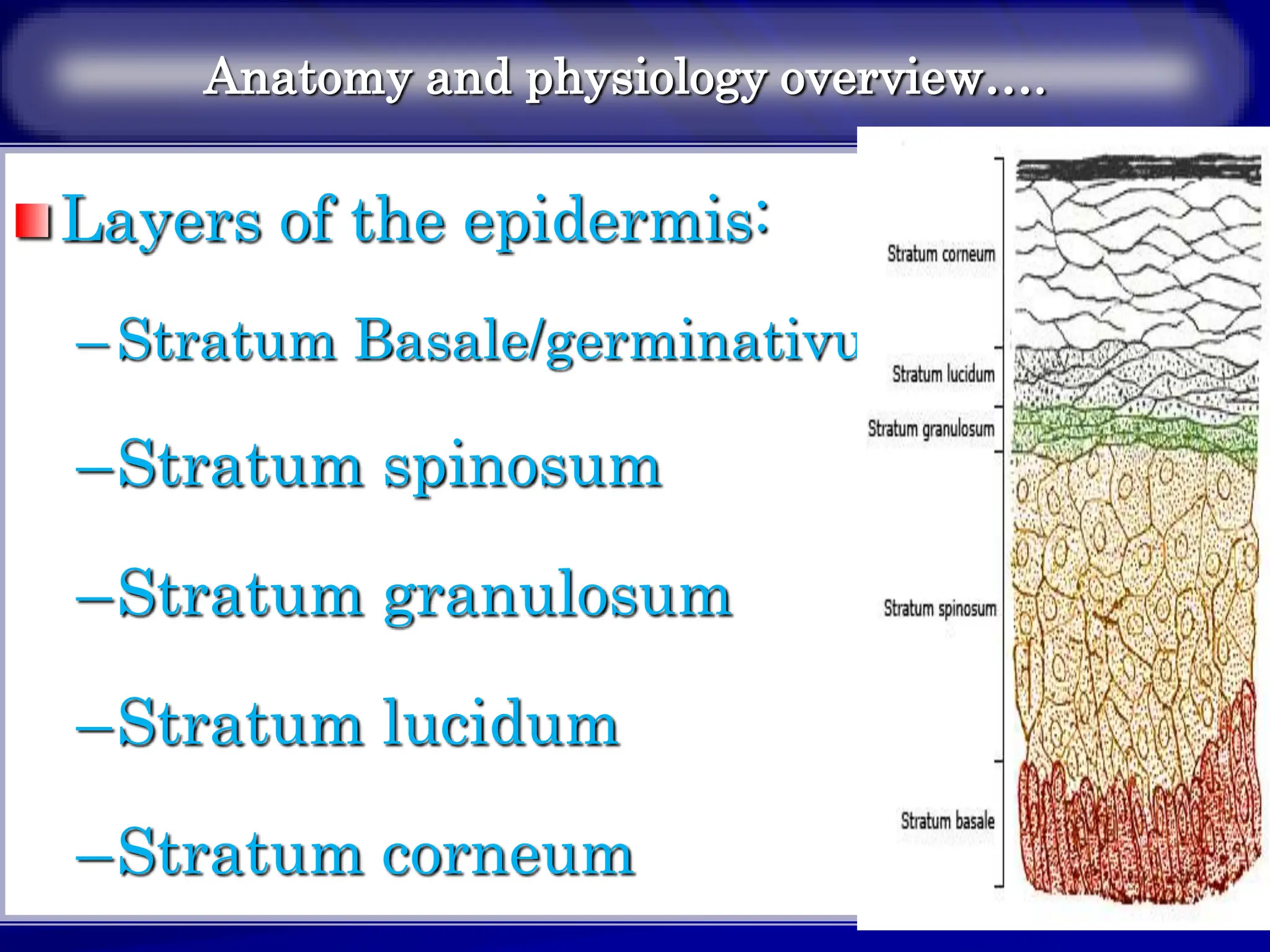
The document provides an overview of the anatomy and physiology of the integumentary system. It describes the three layers of the skin - the epidermis, dermis and subcutaneous tissue. The epidermis is made up of keratinocytes and melanocytes. The dermis contains collagen, fibroblasts and appendages. Skin appendages include hair, nails and glands. Physical examination of the skin involves inspection, palpation and examination of primary and secondary lesions.









































































































































































































































































![Chapter_01_Anatomy_of_Skin[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/chapter01anatomyofskin1-230409112654-4252e8d1-thumbnail.jpg?width=640&height=640&fit=bounds)