1. Toni Anne Alvarez, Andrew Antonio, Katie
Case, Jana Tsuruda, & Kari Wathen
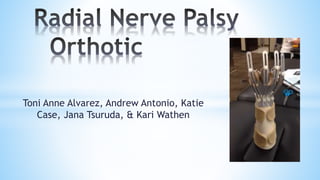
2. Radial Nerve Palsy
● “Wrist drop”
● Radial nerve innervates the distal musculature for
extension of the wrist and digits
● Caused by a high laceration from a traumatic injury
or midshaft humerus fracture
3. ● 23 y.o. Filipino female
● Referred to outpatient orthopedic occupational
therapy
● Bar fight 8 weeks ago
● Enjoys dancing, cooking, going to the beach,
going to the gym, boxing
● Provided sling for shoulder from doctor resulting
in UE guarding and decreased overhead reach
5. ● Colditz, J.C. (2011). Splinting the hand with a
peripheral nerve injury.
o Radial nerve injury is more commonly injured at the higher level
around the humerus
o Splint must be appropriately designed to harness wrist motion while
allowing finger flexion - vital to normal grasp-and-release pattern
o Advantages of this splint:
Allows partial wrist motion and full finger motion
Maintain the normal hand arches
Thumb and CMC joints are unimpeded
Absence of material on palmar surface - allows normal grasp
As function returns, facilitates strengthening of wrist extensors
6. ● McKee, P., Nguyen, C. (2007). Customized dynamic splinting:
orthoses that promote optimal function and recovery after radial
nerve injury: a case report.
o Orthotic intervention addresss both functional needs and biological needs of
the tissues.
o A static volar wrist-hand splint is commonly provided for night use for
positioning the wrist, thumb, and fingers to prevent contractures.
o Tenodesis splints harness active wrist flexion to produce passive finger MCP
extension and conversely harness active MCP flexion to produce passive wrist
extension.
o An advantage over dynamic splints is that tenodesis metal components
closely follow the contours of the hand, thus taking up less space.
8. Name: Radial Nerve Palsy Splint
Purpose: Allowing motion while providing support
● Passive wrist and MCP extension
● Allows active wrist and digit flexion
● Position of wrist extension facilitates power of finger flexion
● Prevent overstretching of denervated muscle
Why chosen:
● Allows functional use of hand through flexion for ADLs, IADLs,
leisure
● Enables FMC
9. Day
● All day (within patient comfort)
● Radial nerve palsy splint
Night
● Consider client sleep schedule
● D- ring splint
Care
● Clean with soap and lukewarm water. Scrub with small brush.
● Rub inside of splint with alcohol to reduce odor.
(www.zmescience.com)
10. S: Pt. reports 4/10 pain in right shoulder. “I cannot get pots and pans
when I cook dinner”.
O: Pt. seen for 45’ OT session. MH right shoulder x 10 min. STM x 5
min. Ther ex x 10 min. Pt education on splint and compensatory
strategies x 10 min. Ther act x 10 min. Wrist ext 20 degrees.
Shoulder flexion 150 degrees.
A: Good increase wrist extension (10 degrees) past week. Limited
shoulder flexion continues to limit household activities.
P: Increase wrist ROM. Decrease pain. Increase overhead reach.
11. Short-Term Goal 1:
Within 2 weeks, pt. will be independent with donning/
doffing splint on ⅘ trials.
Short-Term Goal 2:
Within 2 weeks, pt. will be independent with
compensatory strategies to promote household
activities.
12. ● Axons in the peripheral nervous system have the ability to
regenerate
● Motor supply is restored
● Sensory and sympathetic innervations are restored
● The prognosis for recovery also depends on the extent of
connective tissue damage.
o 1st and 2nd degree injuries have good prognosis
o 3rd-6th degree injuries typically result in incomplete
or failed reinnervation
(www.wikipedia.org)
(Skirven, Osterman, Fedorczyk & Amadio, 2011).
13. Stage One
● Fingers and wrist need to be supported to prevent
shortening of the flexors and overstretching the
extensors
Stage Two
● Motor supply is restored proximal to distal
● Wrist and digit extension remain weak
(Skirven, Osterman, Fedorczyk & Amadio, 2011)
14. WHAT YOU SHOULD KNOW
EBR: Colditz, J.C. (2011). Splintingthehandwitha peripheral nerveinjury.
· Radial nerveinjuryismorecommonlyinjuredat thehigher level aroundthehumerus
· Splint must beappropriatelydesignedtoharnesswrist motionwhileallowingfinger
flexion- vital tonormal grasp-and-releasepattern
Radial NervePalsy Orthotic
Radial NervePalsy
· Alsoknownas
“Wrist drop”
· TheRadial nerve
helpstoextend
(bendback) your
wrist andfingers
· Causescouldbe
fromatraumatic
injurytothe
upper extremity
or fracture.
Radial NervePalsy
Splint
Purpose:
· Allowsmotion
whileproviding
support
· Allowsfunctional
useof thehandto
helpwithactivities
of dailyliving.
· Enablesfinemotor
control.
Splint Wear & Care
Wear:
· For daytimeuse
withinpatient
comfort
Care:
· Cleanwithsoap,
lukewarmwater &
small brush.
· Usealcohol to
helpreduceodor
15. Colditz, J.C. (2011). Splinting the hand with a peripheral nerve injury. In Skirven, T.M., Osterman,
A.L., Fedorczyk, J., & Amadio, P.C. (Eds.), Rehabilitation of the hand and upper extremity (622-
634). Philadelphia, PA: Elsevier, Inc.
McKee, P., & Nguyen, C. (2007). Customized dynamic splinting: orthoses that promote optimal
function and recovery after radial nerve injury: a case report.Journal of Hand Therapy, 20(1),
73-88.
Skirven, T. M., Osterman, A. L., Fedorczyk, J., & Amadio, P. C. (2011). Rehabilitation of the Hand
and Upper Extremity, 2-Volume Set: Expert Consult. Philadelphia, PA: Elsevier, Inc.
Editor's Notes
JT
JT
Bar fight 8 weeks ago where she was stabbed by a broken bottle to her right upper arm
AA also known as a tenodesis splint
KC
KW McKee, P., Nguyen, C. (2007). Customized dynamic splinting:orthoses that promote optimal function and recovery after radial nerve injury: a case report.
Orthotic intervention for radial nerve paralysis should address both functional needs and biological needs of the tissues.
A static volar wrist-hand splint is commonly provided for night use for positioning the wrist, thumb, and fingers to prevent contractures.
Tenodesis splints harness active wrist flexion to produce passive finger MCP extension and converssly harness active MCP flexion to produce passive wrist extension.
an advantage over dynamic splints is that tenodesis metal components closely follow the contours of the hand, thus taking up less space.
KW
AA
AA
KC
Ther ex: overhead pulleys, cleaning in large circles
Neuro re-ed: WB and bilateral activities
Pt. education: splint use and compensatory strategies, no sling
Ther act: household tasks using compensatory strategies
KC
TA
Axons in the peripheral nervous system have the ability to regenerate and under optimal circumstances reestablish contact with the appropriate end organs
regenerating axons grow at a rate about 1mm per day or 1 inch per month
Motor supply is restored from proximal to distal
sensory and sympathetic innervations are also restored to varying degrees
It depends how high the lesion is
The prognosis for recovery also depends on the extent of connective tissue damage.
1st and 2nd degree injuries have good prognosis
3rd-6th degree injuries typically result in incomplete or failed reinnervation due to connective tissue injury and internal nerve scarring.