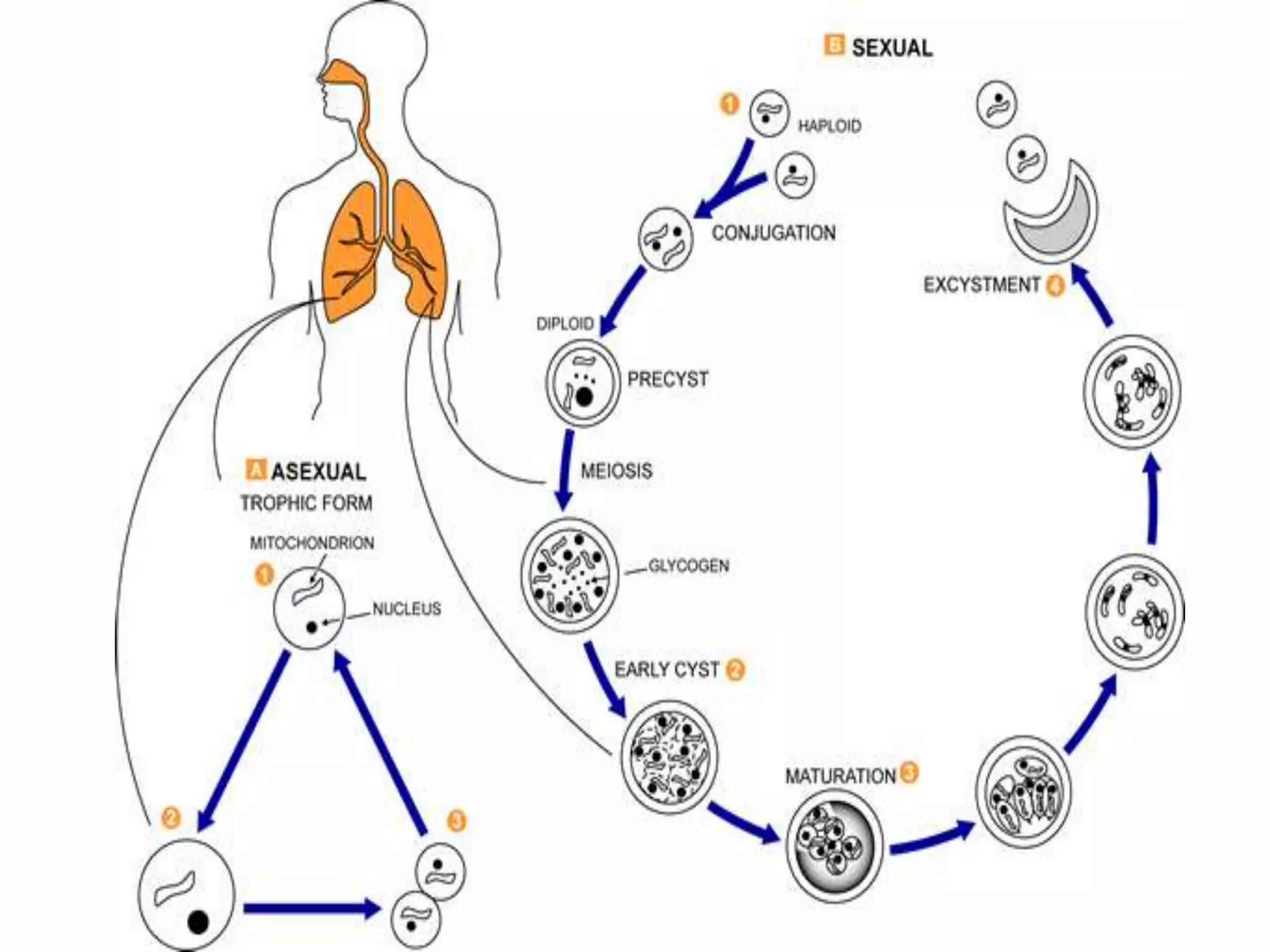
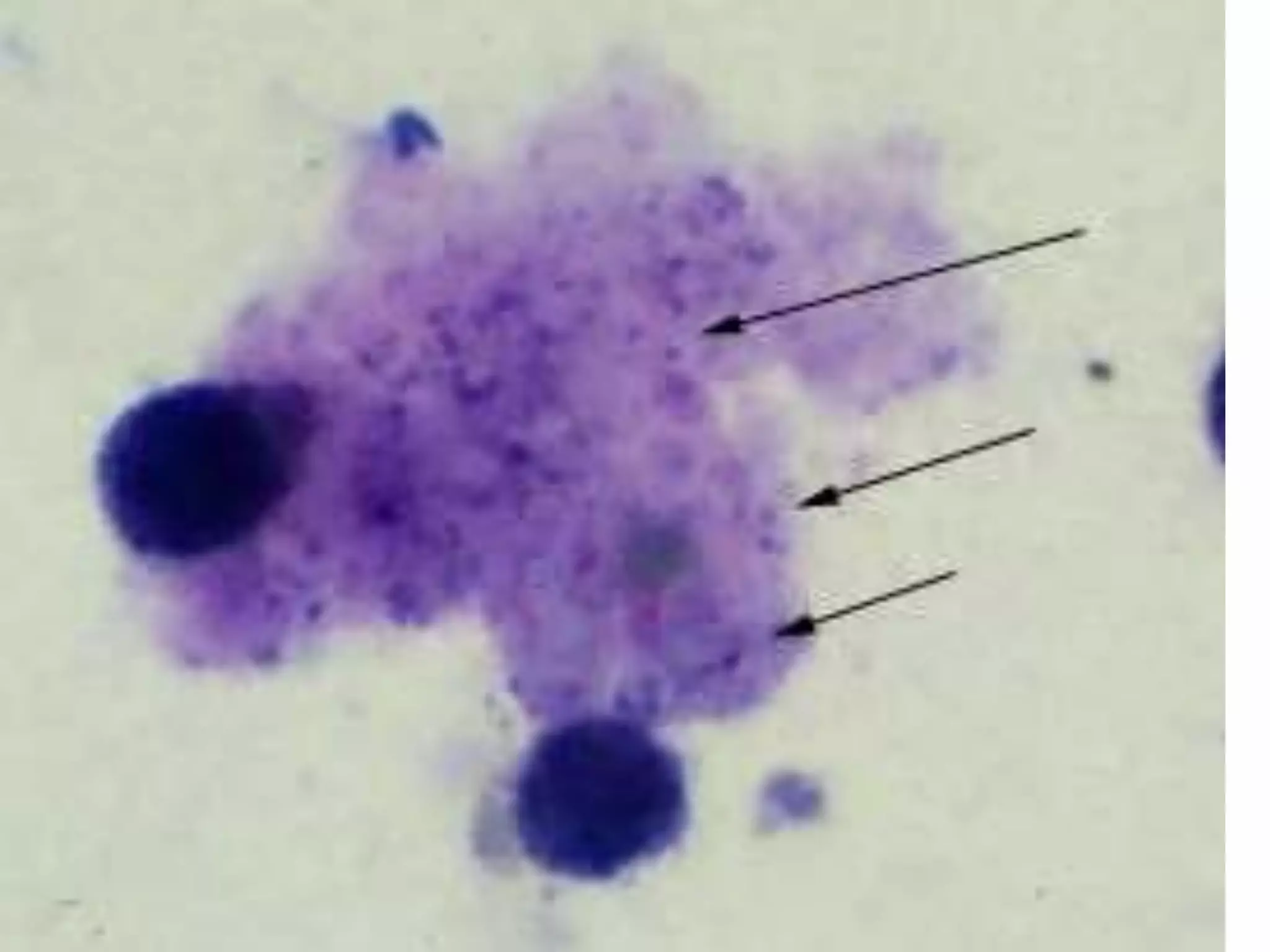
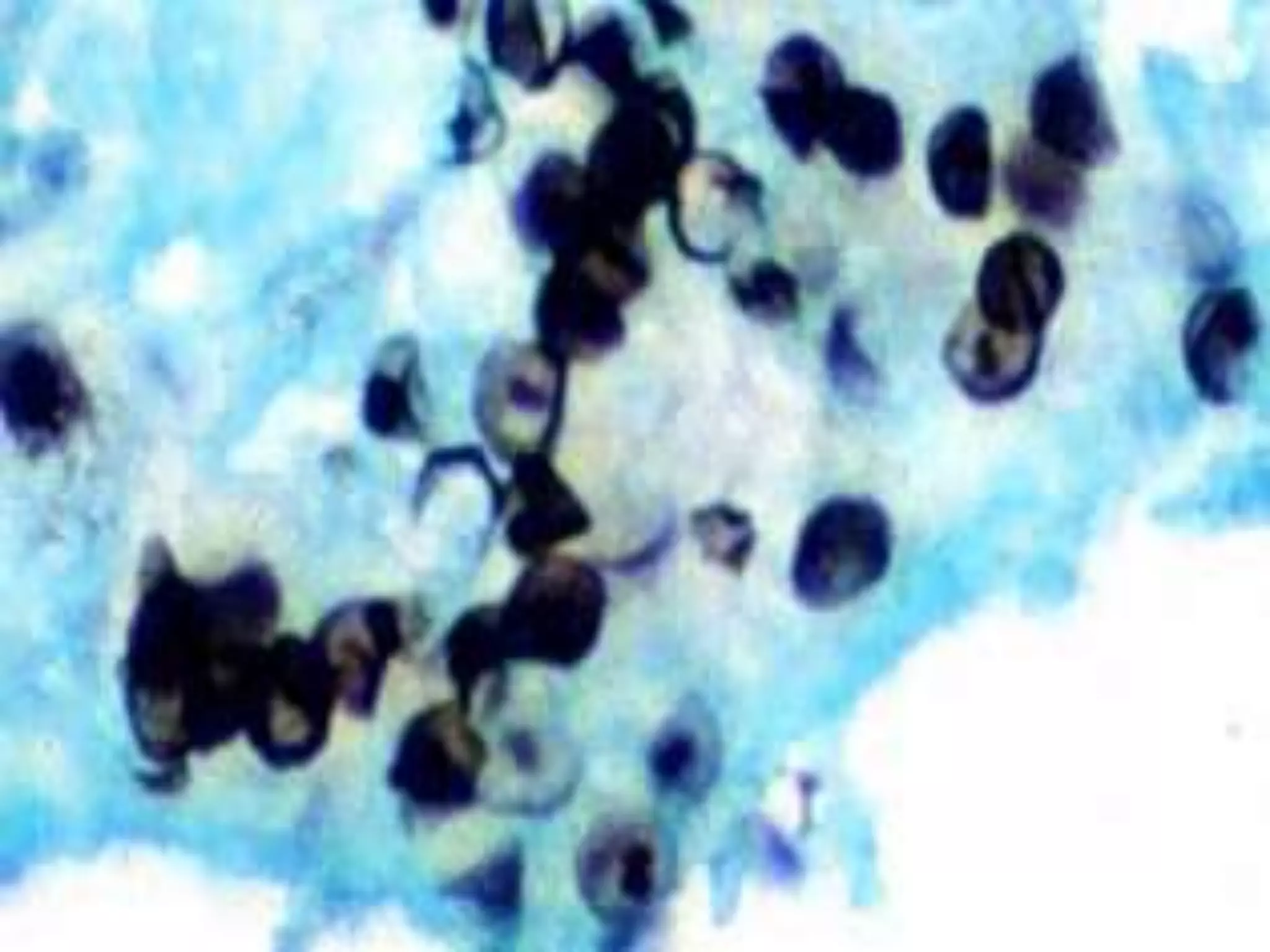
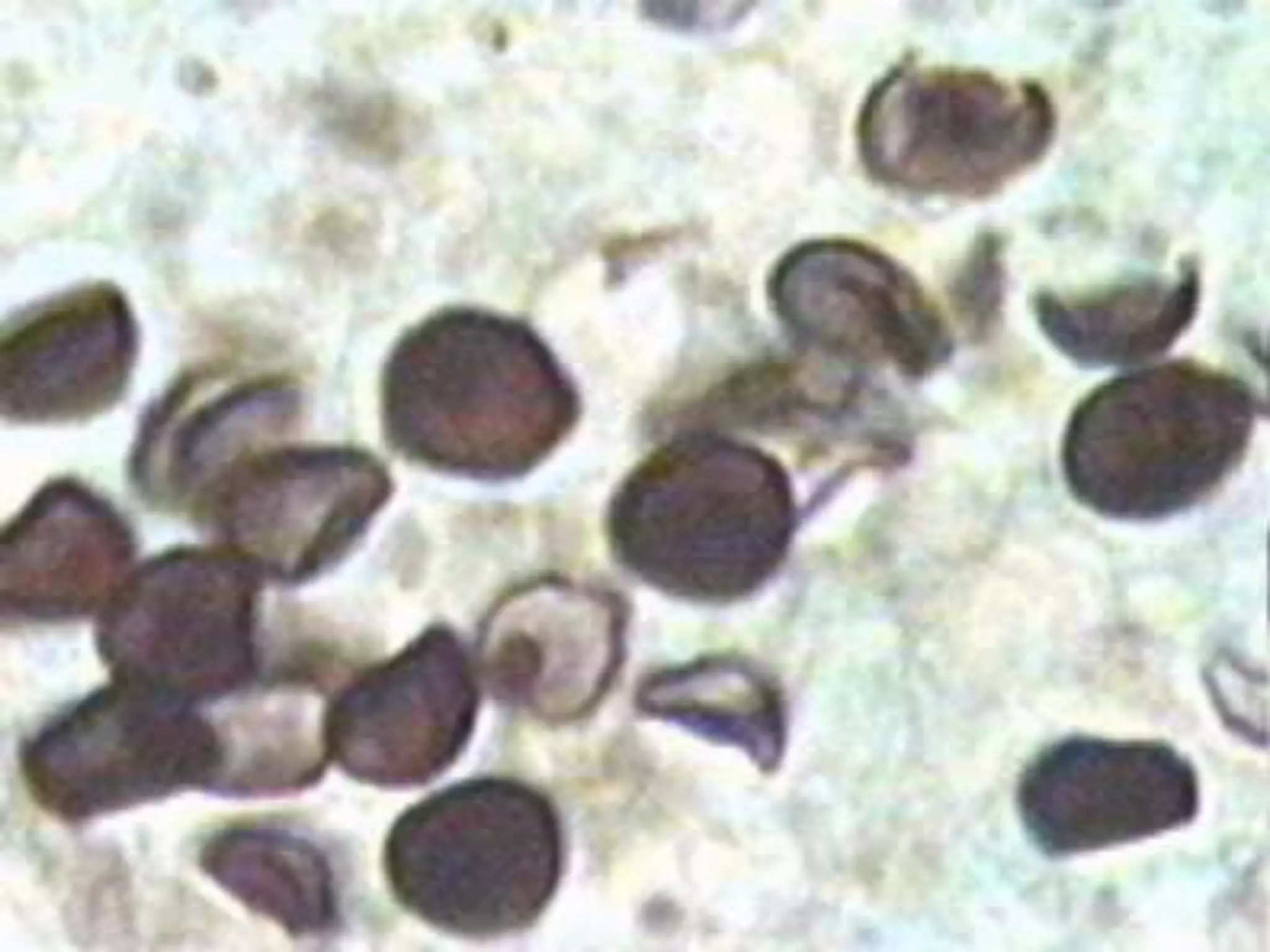
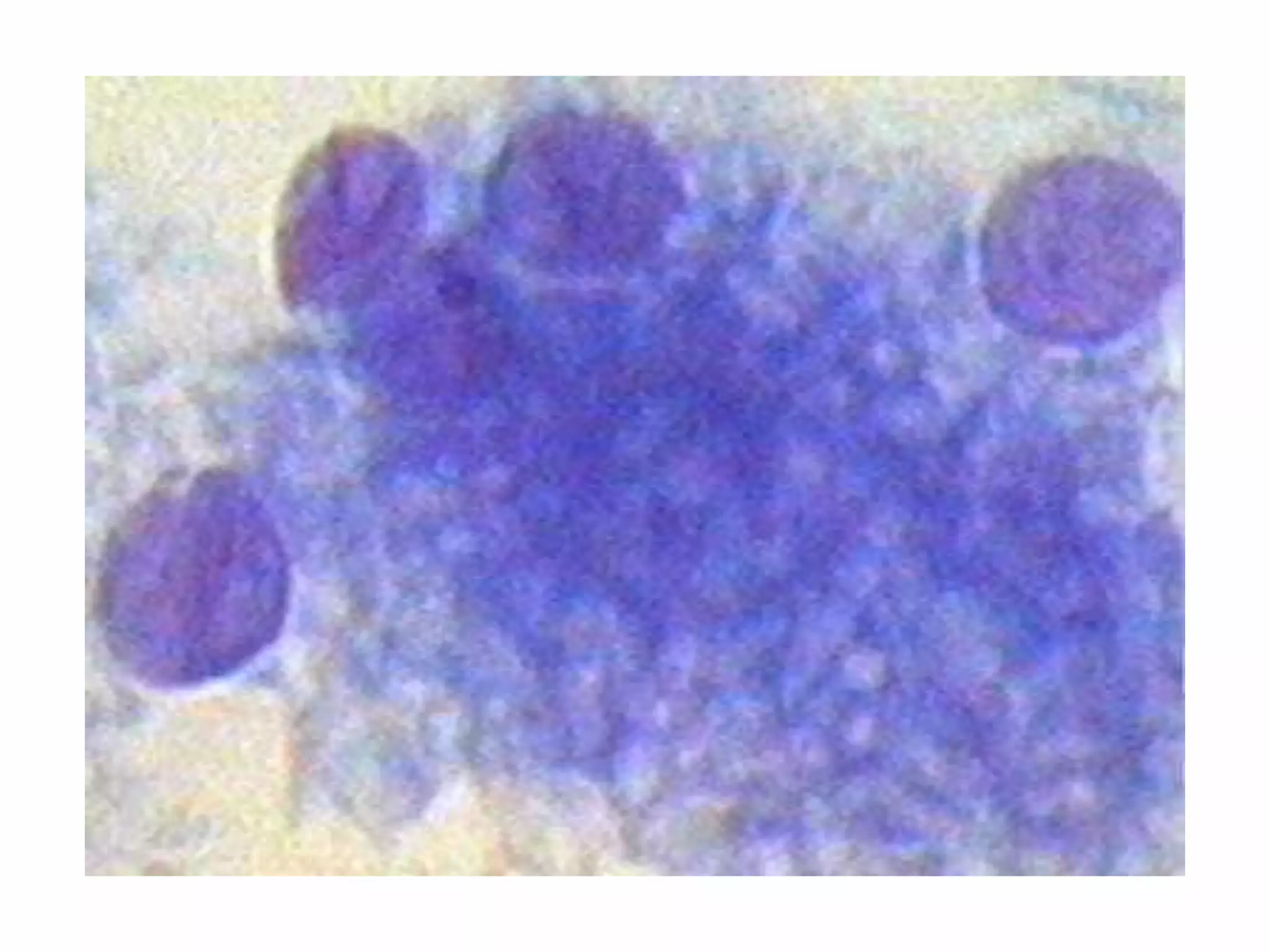
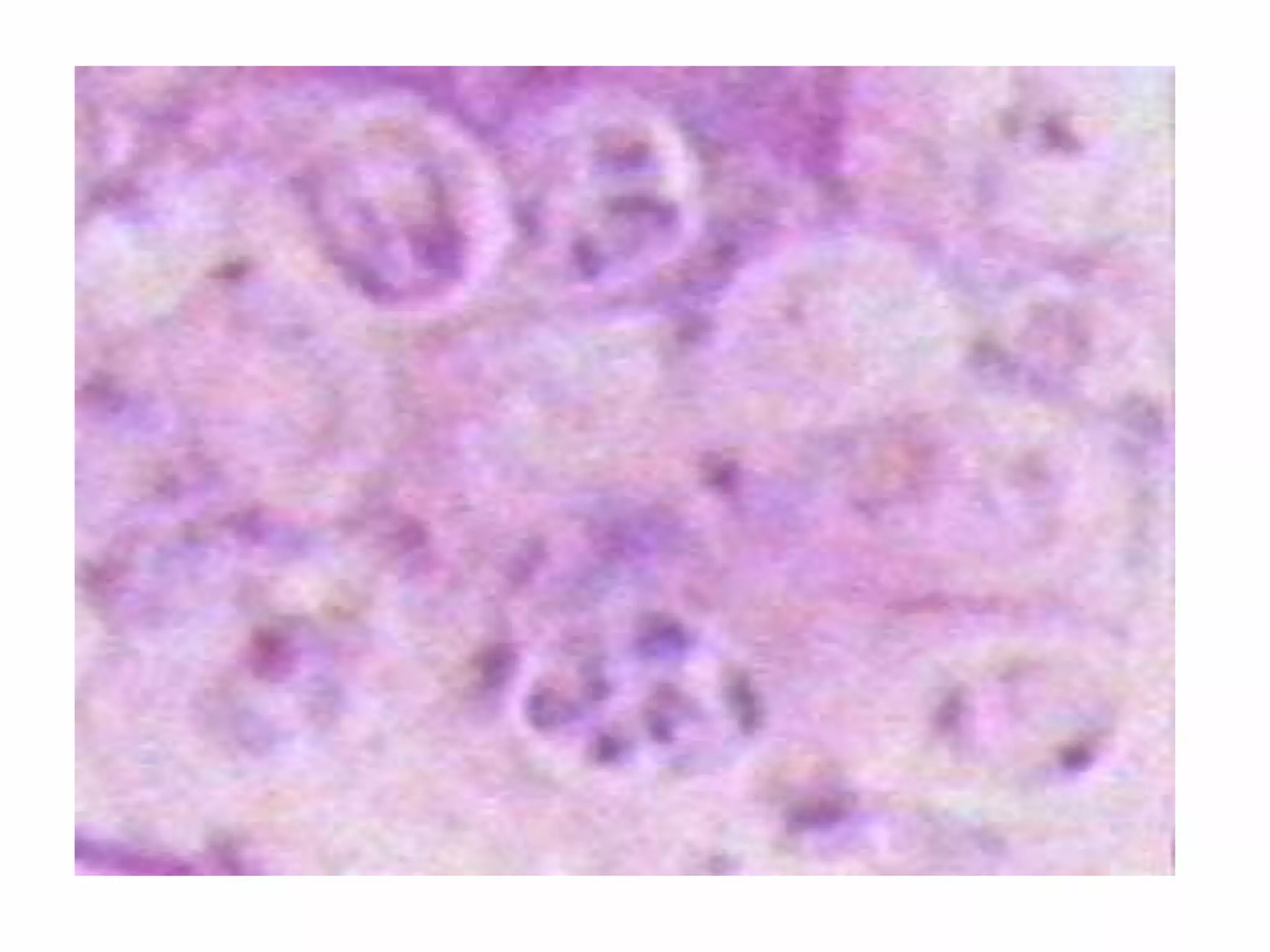
Pneumocystis carinii pneumonia (PCP) is an opportunistic lung infection caused by the fungus Pneumocystis that primarily affects those with weakened immune systems, especially those with advanced HIV/AIDS. It presents with cough, shortness of breath, fever, and lung infiltrates. Before the 1980s AIDS epidemic, it was rare and mainly affected those with malnutrition, leukemia, or on corticosteroids. Diagnosis involves staining sputum or bronchoalveolar lavage samples to identify the characteristic cysts and trophozoites of Pneumocystis under a microscope.