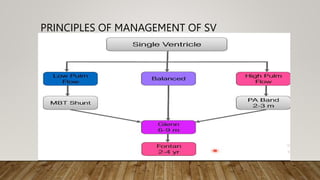
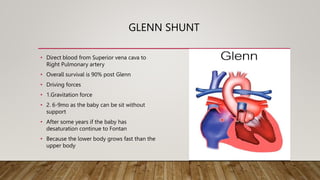
The document provides an overview of the Fontan procedure, a palliative treatment for univentricular congenital heart disease, detailing its significance, indications, and complications. It highlights the steps leading up to the Fontan procedure, principles of management, driving forces, and potential complications such as cyanosis and arrhythmias. Additionally, it discusses the impact of Fontan circulation on systemic venous pressure and associated long-term health considerations.
















































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
