Tef ppt new
•Download as PPTX, PDF•
47 likes•33,042 views

A Tracheoesophageal fistula is a congenital disease. It is a acquired communication between the trachea and esophagus. Most of the patient with TEF are diagnosed immediately following after birth.TEF are often associated with life threatening complications.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Tef ppt new
Similar to Tef ppt new (20)
More from Shivangi sharma
More from Shivangi sharma (20)
Recently uploaded
Recently uploaded (20)
Tef ppt new
- 1. PRESENTATION ON TRACHEAOESOPHAGEAL FISTULA Presented by: SHIVANGI SHARMA M.Sc Nursing Final Year
- 2. OVERVIEW • A fistula is an abnormal communication between two epithelial-lined surfaces. • An atresia refers to complete obliteration or absence of an orifice of a hollow organ. • A stenosis is change in diameter of a hollow organ to become narrower. It can also be called stricture.
- 3. INTRODUCTION • A Tracheoesophageal fistula is a congenital disease. It is a acquired communication between the trachea and esophagus. Most of the patient with TEF are diagnosed immediately following after birth.TEF are often associated with life threatening complications.
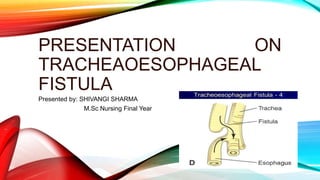
- 4. DEFINITION • A tracheoesophageal fistula, as the name implies, is an abnormal communication between the trachea and esophagus. Congenital tracheoesophageal fistulas are usually diagnosed at birth or soon thereafter.
- 6. INCIDENCE • Approximate 17-70% of children with TEFs have associated development anomalies . These anomalies include Down syndrome, duodenal Artesia and cardiovascular defect. • TEFs are a common congenital anomaly with an incidence of 1 case in 2000-4000 live births
- 7. ETIOLOGICAL FACTORS • Maternal alcohol and smoking • Exogenous sex hormones • Exposure to methimazole • Prolonged mechanical ventilation via Endotracheal or tracheotomy tube • Maternal polyhydamnious • In first trimester exposure to Diabetes mellitus
- 8. CLASSIFICATION • Esophageal atresia with distal tracheoesophageal fistula • Isolated esophageal atresia without a tracheoesophageal fistula. • Isolated tracheoesophageal fistulas • Esophageal atresia with a proximal communication • Esophageal atresia with proximal and distal communications
- 10. PATHOPHYSIOLOGY Upper part of esophagus is developed from retropharyngeal segment and the lower part of the first part of primitive gut. At 4-5 weeks of gestation the laryngeal-tracheal groove is formed. Two longitudinal furrows develop and separate the respiratory tract permordium from esophagus. Deviation cellular growth of the septum results in formation of fistula between esophagus and trachea.
- 12. OTHER… • Excessive secretion • Intermittent, unexplained cyanosis and laryngospasm • Abdominal distention • Violent response after first or second swallow of feeding such as infant cough and chokes fluid returns through nose and mouth • Poor feeding • Inability to pass catheter
- 13. DIAGNOSTIC EVALUATION• Ultrasound scanning • Failure to pass 10F into the stomach through nose or mouth • Catheter left in situ while an x- ray • diagnosis • PH of tracheal secretions in acidic • Flat plate x-ray of abdomen and chest • Barium x-ray • Electrocardiogram
- 15. PHARMOLOGIC MANAGEMENT • Propping infant at 30 degree angle • Nasogastric tube remains in the esophagus and it is aspirated frequently • Nothing by mouth • Supportive therapy include meeting nutritional requirements IV fluid, antibiotics , respiratory support and maintaining neutral environment
- 16. SURGICAL MANAGEMENT Prompt primary repair: fistula found by bronchoscopy is divided, followed by esophageal anastomosis of proximal and distal segments if infant weight permit and is with out pneumonia. Staging: Initially fistula division gastrostomy are performed with later secondary esophageal anastomosis or colonic transposition performed approximately 1 year later to effect total repair
- 17. CONT… Circular esophagotomy: It may be performed on proximal pouch to gain length and allow foe primary anastomosis at initial surgery. Cervical esophagotomy : When ends of esophagus are too widely separated ,esophagus replacement with segment of intestine (colonic transposition ) is done at ages 18 to 24 months.
- 19. CONT… Fiberoptic Tracheoscopy: Repair of trachesophageal fistula can expedite and facilitate surgery on ventilated patient. COMPLICATIONS; Esophagitis Esophageal strictures Recurrent fistula Death from asphyxia Pneumonitis Dehydration
- 20. NURSING DIGNOSIS • Risk for aspiration related to structural abnormalities as evidence by neonate is not able to swallow. • Fluid volume deficit related to inability to take oral fluids as evidence by nil per oral status. • Ineffective airway clearance related to • surgical intervention. • Fear and anxiety of the parents related to critical situation of neonate as evidence by parents look anxious.
- 21. CONT… • Acute pain related to surgical procedure as evidence by child is continuously crying. • Ineffective infant feeding pattern related to congenital defect. • Impaired tissue integrity related to post operative defect. • Knowledge defect related to home base care as evidence by parents asking so many question regarding disease