

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Similar to Colsed angle glaucoma
Similar to Colsed angle glaucoma (20)
Recently uploaded
Recently uploaded (20)
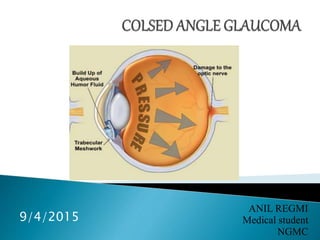
Colsed angle glaucoma
- 2. It is the chronic, progressive optic neuropathy caused by a group of ocular condition, which lead to damage of optic nerve with loss of visual function. Most common risk factor is raised IOP. September 5, 2015
- 3. 1. mechanical change due to raised IOP: Raised IOP ↓ Mechanical pressure to lamina cribrosa ↓ Backward displacement and compaction of laminar plates ↓ Narrows the opening through which axon passes ↓ Damage the nerve fibre bundle September 5, 2015
- 4. 2. Vascular perfusion: Raised IOP ↓ Mechanical pressure on lamina cribrosa ↓ Decrease capillary blood flow ↓ Decrease perfusion to the optic nerve head September 5, 2015
- 5. It includes the spectrum of condition in which peripheral iris moves forward to block the openings of the trabecular meshwork in an occludable angle causing rise in intra ocular pressure. September 5, 2015
- 7. Common in Asians and Eskimos Uncommon in African and Caucasians Age: 4th to 5th decade Sex: female: male = 4: 1 First degree relative are at increased risk September 5, 2015
- 8. 1. Anatomical: Short eye Smaller corneal diameter Shallow anterior chamber Relative anterior positioning of lens-iris and diaphragm. 2. Physiological: Dim illumination Emotional stress 3. Pharmacological : Use of mydriatic drug like atropine, tropicamide September 5, 2015
- 9. Generally bilateral though the involvement of two eye is often asymmetrical. Number of clinical subtypes have been described. September 5, 2015
- 10. Shallow anterior chamber with occludable angle (angle recess < 20’ ) No other gonioscopic abnormalities are present. Provocative test: dark room test : IOP rise by 8mm Hg. mydriatic provocative test : 2% pilocarpine No any clinical symptoms. September 5, 2015
- 11. Shallow anterior chamber with occludable angle (angle recess < 20’ ) IOP rise suddenly while reading in dim light, watching the film in darkened room for short period followed by spontaneous resolution of pupillary block, which is possible due to physiological myosis, which occur during sleep. September 5, 2015
- 12. Patient complains: Unilateral headache or brow ache. Blurring of vision Unbroken colored halos around light during episodes. Between the recurrent attacks, eyes are free of symptoms and only sign of narrow angle recess, clumping of pigment in angle, or occasional peripheral anterior synechiae. September 5, 2015
- 13. It is caused by sudden occlusion of entire angle with resultant acute rise in IOP to extremely high level. Patient complains: Severe unilateral headache. Diminution of vision in red eye. Nausea may be frequently associated. September 5, 2015
- 14. On examination: Corneal edema Shallow anterior chamber Iris bombe with vertically oval. Mid dilated pupil. After resolution of corneal edema, gonioscopically closed angle can be seen i.e. extensive irido-corneal synechiae and optic disc may be found to be either hyperemic or normal. September 5, 2015
- 15. It is said if IOP is chronically raised in eyes if synechial closure over at least 180 degree. Change in optic nerve head or visual field may or may not be present. Causes: a. repeated subacute attacks of primary angle- closure glaucoma ↓ Extensive synechial closure ↓ Chronoically elevated IOP September 5, 2015
- 16. b. acute primary angle closure glaucoma, which persists more than few hours ↓ Irreversible synechial closure of angle and permanent damage to trabecular meshwork. c. asymptomatic or ‘creeping’ angle closure ↓ Synechial closure occurs within depth of angle. ↓ Progressively involves the entire angle. September 5, 2015
- 17. Acute congestive glaucoma is the emergency condition and need to be controlled immediately. Management is essentially surgical. Medical therapy is given as an emergency and temporary measure in order to decrease IOP before ready for operation. September 5, 2015
- 18. 1. systemic hyperosmotics to decrease IOP given as soon as diagnosed. i.v. Mannitol (1gm/kg body wt) Oral glycerol (1.5gm/kg) 2. tab. Acetazolmide 3. Analgesics and antiemetics 4. Pilocarpine eyedrops – started after IOP is bit lowered by hyperosmolar agents. 5. Beta-blocker – 0.5% Timolol BD 6. Corticosteroid eyedrop. E.g. dexamethasone 3- 4times/day to reduce inflammation. September 5, 2015
- 19. 1. Peripheral laser iridotomy: Indications: Peripheral anterior synechiae: <50% of angle Prophylactic Bypass pupillary block A hole is made in peripheral iris allowing the aqueous to drain directly from posterior chamber to region of trabecular meshwork. Laser iridotomy : non invasive method September 5, 2015
- 21. 2. Trabeculectomy (filtration surgery) Indication: IOP not controlled within 12 hours of vigorous medical therapy Peripheral anterior synechiae: >50% of angle It provides an alternative to angle of drainage of aqueous from anterior chamber into subconjunctival space. September 5, 2015
- 23. 1. All of following anatomical change predispose to primary angle closure glaucoma expect? a. Small cornea b. Flat cornea c. Shallow anterior chamber d. Short axial length of eyeball September 5, 2015
- 24. 2. All are the feature of acute attack of primary narrow angle glaucoma expect? a. IOP raised up to 40-70mm Hg b. Eye red, painful, and tender c. Disc shows glaucomatous cupping d. Fellow eye also shows shallow anterior chamber September 5, 2015
- 25. 3. The most common provocative test for angle closure glaucoma is: a. Water drink test b. Dark room test c. Mydriatic-miotic test d. Homatropine mydriatic test September 5, 2015
- 26. 1. A 55 years old patient with moderate hypermetropia in both eyes presented in emergency department with sudden painful diminution of vision. O/E, her right eye was red with high IOP and shallow anterior chamber and her left eye also had shallow anterior chamber. a) What is your most likely diagnosis? b) Write about the treatment? c) Write briefly about the aqueous secretion and drainage? September 5, 2015
- 27. THANK YOU September 5, 2015