
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Class first molar pregnancy
Similar to Class first molar pregnancy (20)
Recently uploaded
Recently uploaded (20)
Class first molar pregnancy
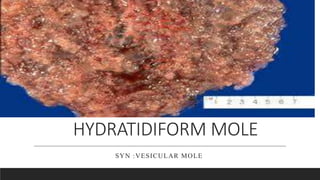
- 2. Introduction It is an abnormal condition of the placenta where they are partly degenerative and partly proliferative changes in the young chorionic villi. These result in the formation of the clusters of the small cysts of varying size.
- 3. Introduction contd…… Because of its superficial resemblance to hydratid cyst, it is named as hydratidiform mole. It is best regardes as a benign neoplasia of the chorion with malignant potential.
- 4. Incidence There is a wide range of geographical and ethnic variation of the prevalence of the condition . It is more common in China, Indonesia ,Japan. Highest in philippines-1 in 100 pregnancy Lowest in European countries(USA)-1in 2000 Incidence in India –1 in 400
- 6. Classification Partial mole • Some fetal tissue ,blood vessels and villi present Complete mole • No fetal tissue , blood vessels and villi formation
- 7. Etiology The cause is not definitely known ,but it appears to be related to the ovular defect as it sometimes affects one ovum of a twin pregnancy .however, the following faactors and hypothesis have been forwarded:
- 8. Etiology contd.. Its prevalence is higher in teenagers and in women aged beyond 35 years. The prevalence appears to vary with race and ethnic group Inadequate intake of protein , carotene and high intake of animal fat specially in oriental countries. Imbalance immune mechanism eg in hepatic disease rise in gamaglobuline ,AB blood group.
- 9. Etiology contd..... Cytogenetic abnormalities The higher the ratio of paternal :maternal chromosomes, the greater is the molar change . Complete mole show 2:1 ratio History of prior hydratidiform mole increases the chance of recurrence(1 to 4%).
- 10. pathophysiology This Photo by Unknown author is licensed under CC BY.
- 11. Pathophysiology contd….. Death of the ovum or failure of the embryo to grow is essential to develop complete hydratidiform mole The secretion from hyperplastic cells and transferred substances from the maternal blood accumulate in the stroma of the villi Results in the distension of the villi to form vessicles
- 12. Pathophysiology contd…… The distension may also due to the edema and liquification of the stroma Vesicle fluid contain excessive hCH
- 13. Clinical feature SYMPTOMS Vaginal bleeding Varying degree of lower abdominal pain Constitutional symptoms: a.patien become sick without any apparent reason
- 14. b. vomitting become excessive c.breathlessness due to pulmonary embolism of trophoblastic cell Expulsion of grapes like vesicles per vagina is diagnose of vesicle mole History of quickening is absent
- 15. Sign Feature suggestive of early months of pregnancy are evident The patient look more ill than can be accounted for. Pallor is usually prominent ,out of the proportion of the visible blood loss
- 16. Feature of preeclampsia due to the hyperactivity of the trophoblastic cells Per abdomen : The size of the uterus : larger The feel of the uterus : firm elastic Fetal parts: not palpable Absence of fetal heart sound
- 17. Vaginal examination Internal ballottement can not be elicited Finding of the vesicles in the vaginal discharge If cervical os is open, instead of membranes,blood clot or the vesicles may be felt.
- 18. Investigations Full blood count ,ABO and Rh typing Hepatic ,renal and thyroid function are carried out Sonography: Qualitative estimation of chorionic gonadotrophin Straight X- ray abdomen CT and MRI Beta –hCG estimation
- 19. Differential diagnosis Threatened abortion Fibroid or ovarian tumor with pregnancy Multiple pregnancy
- 20. Complication Haemorrhage and shock due to vaginal bleeding over a time Sepsis – inccrease the chances of ascending infection due to blood clot ,vaginal bleeding and absence of fetal membrane Uterine perforation – due to invasive mole or surgical procedure
- 21. Complication contd….. Gestational trophoblastic disease – it may develop persistently elevated beta –hCG and may lead to choriiocarcinoma Recurrence – there are chances of recurrence of the mole in subsequent pregnancies.
- 22. Management The principle of management are : Supportive therapy to restore the blood pressure and infection Evacuation of the uterus as soon as diagnosis is made Counselling for regular follow up to detect the persistent trophoblastic disease
- 23. Management Contd… 1.supportive management Group A – the patient usually presents with various amount of bleeding : to starts a ringers solution I.V. infusion Arrangement is made for blood transfusion
- 24. Management contd… Group B- blood should also be kept ready prior to elective evacuation of the uterus.
- 25. Management contd…... 2. Definitive management : Suction evacuation (it is the treatment of choice irrespective of the uterine size) suctioning with manual vacuum aspiration is safe, which should be done rapidly. The risk of perforation is high in using metal curettage.
- 26. Management contd… digital exploration and removal of the mole by ovum forceps may helpful to evacuate the content of the uterus. Infuse oxytocin 20 unit in 1 liter IV fluids (NS or RL) at 60 drops per minute to prevent hemorrhage once evacuation is under way. Administration of Rh ( D) immunoglobulin to women who are Rh negative to prevent isoimmunization
- 27. Management contd…… Hysterotomy : the procedure are rarely done. The indications are; Profuse vaginal bleeding Cervix unfavourable for immediate vaginal evacuation
- 28. Management contd… Hysterectomy :this is indicated in; Patient with age over 35 High risk patient with development of future malignancy Female has completed her family irrespective of age Perforating mole Placental site trophoblastic tumor
- 29. Management contd…. 2. Follow up management: Routine follow up is mandatory for all cases for at least 6 months following molar pregnancy. first B- hCG level is obtained 48 hours after evacuation Then monitor serum hCG levels every weekly till they become normal for three consecutive weeks.
- 30. Management contd…. Once the hCG levels falls to a normal level for 3 weeks, test the patient monthly for 6 months; then follow- up is discontinued and pregnancy allowed. During the 6 month surveillance period, patient is advised not to become pregnant.
- 31. Contraceptive advice Contractive of choice being combined oral pills IUD is contraindicated, because of its frequence association of the irregular bleeding Inj. DMPA can be used safely surgical sterilization is another alternative when family size is complete