18. • One of the toughest challenge for vascular
specialists
• Diagnosis and initial assessment –clinical.
• Diagnostic errors --amputation or even death.
• Multiple comorbidities
19. Aetiology & Pathology
• Sudden deterioration in the arterial supply to
the limb
• Embolism
• Thrombosis
• Trauma
• Iatrogenic
20. • Differentiation of embolism and thrombosis –for
diagnosis and prognosis
• Embolism –cardiac /proximal artery with
atherosclerotic plaque
• Common sites:
• Common femoral and popliteal arteries--LL
• Brachial artery bifurcation & brachial artery at the
takeoff of the profunda brachialis artery—upper
limb
• Saddle emboli –aortic bifurcation
21. • Emboli –plug
• Catastrophic–due to occurrence in otherwise
normal arteries
• Acute white leg, including a complete
neurosensory deficit
• Progressive --–secondary thrombus on both
sides—difficult to remove
22. Cardiac embolism
• Platelet rich thrombus
• Atrial fibrillation
• Mural thrombus in MI
• Left ventricular aneurysm
• Cardiac valvular disease
23. Paradoxical embolism
• DVT –PFO—Arterial embolism
• ALI with DVT in young patient
Cardiac tumour—Myxoma
Endocarditis
• IV drug users
• Indwelling catheters
• Immunocompromised
25. Thrombosis
• Blood clotting within an artery
• Progressive atherosclerotic obstruction ---less
severe than embolism; Plaque disruption
• Hypotension with atherosclerotic disease
• Hypercoagulability---Malignancy and
thrombocythemia/ HIT
• Arterial dissection—Aortic dissection –
Trauma/SHT
26. • Vasospasm –Raynauds –vasodilators
/prostanoids
• Inadvertent injection of drugs
• Bypass graft occlusion –due to thrombosis
27.
28. Clinical presentation
• Depends on size of the occluded artery and
collaterals status
• Loss of sensation is one of the earliest signs of
acute leg ischemia
• Motor nerves --muscle weakness.
• skin and finally muscles --reduction in arterial
perfusion. M
• Muscle tenderness -end-stage signs of acute
leg ischemia.
30. Clinical assessment
History
• Etiology and duration
• 6-8 hours severe/complete occlusion --
necrosis
• Risk factors: smoking, hypertension,
hyperlipidemia and family history.
31. Physical findings
-Fundamental in assessing the severity
-6 P’s
Pain, pallor, paresis, pulse deficit, paresthesia,
and perishing with cold
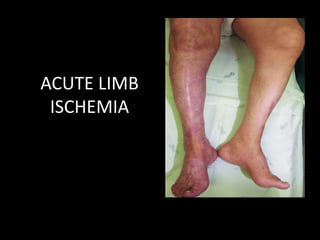
32. • Marble-white skin - acute total ischemia.
• Slow capillary refill -small degree of distal flow
and probable patent runoff vessels.
• Sensory –fine touch and proprioception
• Muscle tenderness in calf with weakness –
advanced ischemia
• Palpation of peripheral pulses ---level of occlusion
• Full physical examination
33. Hand held doppler
• Pedal arterial signals – absent /reduced.
• Biphasic signals excludes the diagnosis.
• Soft monophasic signals - patent distal vessels but proximal arterial occlusion.
• Absent Doppler signals in the ankle arteries - poor prognostic sign.
• Severe ischemia--ankle Doppler pressures are impossible to measure--owing
to the lack of signal /muscle tenderness.
• Less severe ischemia, an ankle pressure of 30 to 50 mm Hg and an ankle-
brachial index of about 0.3 --subcritical acute ischemia.
• Doppler can also be used to examine the extremity veins.
• Popliteal venous occlusion--poor prognostic sign in a patient with acute
arterial ischemia
35. Classification
• More valuable method of classification - based
on the severity of the arterial ischemia-
determining the urgency of intervention and
has implications for outcome
• Acute ischemia - sudden decrease in limb
perfusion causing a potential threat to limb
viability
37. • Class I –Conservative
• Class III—Amputation
• Class II –Requires intervention
• Differentiation of II a/II b important – pain at
rest, sensory loss, and muscle weakness
40. Initial Management
Anticoagulation:
• UFH : 70-100 U/Kg –bolus ---1000u/hr infusion
• Allergic to heparin –direct thrombin inhibitors
• Target aPPT 50-80 sec or 2-3 times of normal
41. Supportive measures
• O2 by face mask –improves skin perfusion
• Hydration –to avoid renal dysfunction –to
titrate with urine out put
• Foot end down
• IV analgesia
• Avoid IM injections
42. LAB investigations
• Renal function tests
• CBC
• Coagulation profile
• Work up for thrombophilia
• CPK level
• Fibrinogen level
43. Treatment
• Class I—anticoagulation –Elective
• Class III—Anticoagulation with stabilisation of
patient –amputation
• Class II a—Urgent revascularization after
proper assessment (<14 days –EV/>14 days –
Surgical)
• Class II b—Immediate revascularization –
Surgical/ EV /Hybrid
46. Contraindications
Absolute:
• Active internal bleeding
• Irreversible limb ischemia (severe sensory
deficits, muscle rigor)
• Recent stroke (arbitrary guidelines: TIA within 2
months or CVA within 6–12 months)
• Intracranial neoplasm or recent (2 months)
craniotomy
• Protruding mobile left-sided heart thrombus
47. Relative contraindications
• History of gastrointestinal bleeding
• Recent (10–14 days) major surgery, including biopsy
• Recent trauma
• Recent CPR
• Severe uncontrolled high blood pressure
• Emboli from a cardiac source
• Subacute bacterial endocarditis
• Coagulopathy
• Pregnancy and the postpartum period
• Severe cerebrovascular disease
• Diabetic retinopathy
48. Preprocedural evaluation
• Non invasive imaging
• Lab investigations
• Access site selection
--Ipsilateral /Contralateral
--Brachial artery –iliac occlusion
--USG guided, micro puncture
--Direct puncture of graft (axillo-femoral bypass:
two sheaths)
--Avoid axillary artery puncture
49. Procedure
• Arterial access
• Initial angiogram—5F sheath
• 6F cross over
• Traverse occlusion with 0.035 guide wire and
periodic angiography
• Oblique views –Grafts
• GWTT
• Total length of occlusion –infusion catheter
52. Infusion techniques
Stepwise infusion
• The tip of the catheter is placed in the proximal aspect
of the thrombus, and a fixed amount of lyric agent is
infused. As the thrombus dissolves, the catheter is
advanced and the process is repeated.
Continuous infusion
• Steady infusion of the lytic agent, with or without
lacing the thrombus.
Graded infusion
• Periodic tapering of infusion rates, with the highest
rates given initially.
53. Accelerated thrombolysis
• Lacing the thrombus with a high-dose lytic agent initially
to bathe the thrombus.
Pulse-spray infusion
• Forceful injection of the lytic agent into the thrombus to
fragment it and increases the surface area exposed to
the lytic enzyme.
54. Pulse-spray pharmacomechanical thrombolysis
• Mechanical thrombus disruption and infusion of lytic
agents. The mechanical effect can be achieved with the
use of pulse-spray catheters, microporous infusion
balloons, or mechanical thrombectomy devices.
Enclosed thrombolysis
• Infusion of a lytic agent between two balloons spaced
across the length of the thrombus.
55. • Thrombolysis with UK/rt-PA/SK
• Novel thrombolytic regimen :Abiciximab
/Alfimeprase
• Intra thrombotic lacing: depositing the
concentrated drug within the thrombus –
decrease dose/duration /complication of
treatment
• From distal to proximal lacing
• Concomitant IV anticoagulation with heparin
• Avoid mixing of heparin with lytic agent
56. Infusion systems
• Cragg Mc-namara valved infusion catheter
• Prostream infusion wire
• Micromevi multiple side hole infusion catheter
• Fountain Infusion Catheter With Squirt Fluid
Dispensing System
• Mistique Infusion Catheter
• Fountain Occluding Wire
58. Cragg Mc-namara
• Valved-tip single
lumen catheter with
side holes
• 4-5 F, 40,65,100 , 135
cm length, 5,10,
20,30,40 &50 cm
length holes
59.
60. USG enhanced thrombolysis
• Microstreaming –enhances the transport
/dissemination of lytic agent
• Accelerating the contact of thrombus with
drug
• Separates /loosens fibrins strands, increase
surface area
• EKOS infusion catheter
61.
62.
63. Post procedure management
• Pressure bandage
• Puncture site –checked every 30 min for 4hrs
then every 2 hrs during infusion
• ICU/step down unit as per institution
• Extremity pulses –every 4 hrs
• Lab: Hct, PT, aPTT/ACT every 2hrs twice then
needed
• Desired aPTT :2-3 times ; ACT: 300
64. • Fluid input/output
• Serum creatinine
• Avoid IM injections
• Hep.Saline infusion in coaxial catheter
• Recheck angiogram
• Termination—successful recanalization
/complication or failure
• Underlying lesion to be treated
• Sheath removed after ACT <160
• IV anticoagulation restarted after 4-6 hrs oof
sheath removal
84. Thrombo-aspiration In Peripheral
Ischaemia (TIPI)
• No recanalisation of the thrombotic occlusion : 0
• Incomplete or partial recanalisation of the
thrombotic occlusion with no distal flow :1
• Incomplete or partial recanalisation of the
thrombotic occlusion with any distal flow: 2
• Complete recanalisation of the thrombotic occlusion
with normal distal flow : 3
86. Upper limb ischemia
• Less common
• Mostly embolic (cardiac)
• Thrombosis is rare
• Surgical /endovascular methods
• Whirpool embolism
87. Acute limb ischemia in children
• Rare and catastrophic
• Mostly iatrogenic (<1 yr) followed by trauma
• Mostly due to trauma (>2 yrs)
• Conservative treatment
88. European Society for Vascular Surgery
(ESVS) 2020 Clinical Practice Guidelines on
the Management of Acute Limb Ischaemia
• Total 61 recommendations
• For patients presenting with a possible diagnosis of
acute limb ischaemia, it is recommended that clinical
assessment is performed urgently by a vascular
specialist, who should be responsible for planning
further investigation and management
89. • For patients presenting with acute limb ischaemia, the
Rutherford classification for acute limb ischaemia is
recommended for clinical evaluation.
• For patients presenting with acute limb ischaemia, diagnostic
imaging is recommended to guide treatment, provided it does
not delay treatment, or if the need for primary amputation is
obvious.
90. • For patients presenting with acute limb ischaemia, computed
tomography angiography is recommended as the first line
modality for anatomical imaging.
• For patients presenting with acute limb ischaemia, it is not
recommended to use results of myoglobin and creatine kinase
on admission to base the decision to offer revascularisation or
primary amputation.
91. • For patients with acute limb ischaemia awaiting
revascularisation, heparin, supplemental oxygen, adequate
analgesia and intravenous rehydration are recommended
• For patients with acute limb ischaemia, treated by open
surgery, prostacyclin analogues may be considered during and
after revascularisation.
• It is recommended that patients diagnosed with acute limb
ischaemia referred to vascular center and treatment in hybrid
center
92. • For patients requiring surgical thrombo-embolectomy for acute
limb ischaemia, regional or local anaesthesia may be considered,
but always with an anaesthetist present.
• For patients requiring an infrainguinal bypass procedure for acute
limb ischaemia, the preferential use of a vein graft should be
considered.
• For patients undergoing open and endovascular surgery for acute
limb ischaemia, completion angiography is recommended.
93. • For patients with residual thrombus after open surgery for acute
limb ischaemia, intra-operative local thrombolysis may be
considered.
• For patients with acute limb ischaemia caused by graft occlusion,
identification and treatment of the cause of graft occlusion is
recommended.
• After open revascularisation for acute limb ischaemia, simultaneous
endovascular treatment addressing inflow or outflow stenosis
should be considered
94. • For patients with acute limb ischaemia, intravenous
thrombolysis is not recommended
• For patients with acute onset claudication (Rutherford grade I)
that does not threaten the limb, (percutaneous)
catheterdirected thrombolysis is not recommended.
• For patients with Rutherford grade IIa acute limb ischaemia, it
is recommended that (percutaneous) catheter-directed
thrombolysis is considered as an alternative to surgery.
95. • For patients with Rutherford grade IIb acute limb ischaemia,
(percutaneous) catheter-directed thrombolysis may be considered
if initiated promptly, and may be combined with percutaneous
aspiration or thrombectomy.
• For patients with acute limb ischaemia undergoing endovascular
therapy, ultrasound guidance for arterial access is recommended.
• For patients with acute limb ischaemia undergoing thrombolysis, it
is recommended that recombinant tissue plasminogen activator or
urokinase is used
96. • For patients undergoing thrombolytic therapy for acute limb
ischaemia, routine monitoring of plasma fibrinogen is not
recommended
• For patients undergoing thrombolysis for acute limb ischaemia,
continuous systemic therapeutic heparinisation is not
recommended.
• It is recommended that patients undergoing thrombolytic
treatment for acute limb ischaemia should be monitored for vital
signs, access site complications, and the condition of the limb.
97. • For patients treated for acute limb ischaemia, it is
recommended that thrombolysis be stopped if major
bleeding occurs during treatment.
• For patients treated for acute limb ischaemia who have minor
bleeding during thrombolysis, continued treatment should be
considered, after evaluation of the risk and benefit of
stopping or continuing.
• For patients with acute limb ischaemia, aspiration and
mechanical thrombectomy should be considered.
98. • For patients with acute limb ischaemia secondary to
thrombosis of a popliteal artery aneurysm, repair of
the aneurysm with a saphenous vein bypass should
be considered with pre /intraoperative thrombolysis;
stent graft should not be used
• For patients who have had revascularisation for acute limb ischaemia, clinical examination is
recommended to diagnose post-reperfusion compartment syndrome.
99. • Compartment pressure measurement may be considered to
diagnose post-reperfusion compartment syndrome, when the
clinical diagnosis is uncertain
• For patients who have had revascularisation for acute limb
ischaemia, routine prophylactic fasciotomy is not
recommended, as it is associated with prolonged hospital
stay, local infection, and development of late deep venous
insufficiency
100. • Prophylactic four compartment fasciotomy should be
considered if ischaemia before revascularisation has
been profound or prolonged
• Emergency four compartment fasciotomy is
recommended to treat post-ischaemic compartment
syndrome (within 2 hrs); Delaying more than 6 hrs is
not recommended
101. • After revascularization for acute limb ischaemia, follow up
should be considered, including the patient’s cardiovascular
condition and functional status of the limb.
• For patients revascularised for acute limb ischaemia of
embolic origin, it is recommended that, whenever possible,
the source of the embolus be investigated, to prevent
recurrence.
• After revascularisation for acute limb ischaemia caused by an
embolus secondary to atrial fibrillation or intracardiac
thrombus, long term anticoagulation is recommended.
102. • Long term anticoagulation may be considered after
thrombectomy or endovascular treatment of a prosthetic
bypass graft occlusion.
• Antiplatelet therapy or anticoagulation and statins are
recommended long term to reduce cardiovascular events
following acute limb ischaemia revascularisation caused by
native artery thrombosis, thrombosis of a popliteal artery
aneurysm, or failure of previous revascularisation.
103. • For patients treated by open or endovascular
surgery for thrombosed popliteal artery
aneurysm, duplex ultrasound imaging of the
treated and contralateral arteries, as well as of
the aorta, iliac, and femoral arteries, every
three years should be considered.
104. • For patients who have undergone
revascularisation for acute limb ischaemia
secondary to acute aortic occlusion, close
collaboration is recommended with
anaesthetists and intensivists to reduce the
complications of ischaemia reperfusion injury.
105. • For a patient with acute ischaemia of the
upper limb, conservative treatment with
anticoagulation alone is not recommended if
the arm is threatened, or if limb function is
important to quality of life.
106. • For infants and children younger than 2 years
of age with acute limb ischaemia, initial
conservative management with heparin is
recommended.
107. • For infants and children with acute limb ischaemia
without improvement after conservative therapy
with heparin, thrombolysis, or open surgical
revascularisation may be considered.