This document provides information on arterial blood gas (ABG) analysis, including indications, contraindications, sampling procedures, normal values, terminology, and how to interpret ABG results. It discusses assessing adequacy of oxygenation, classifying acid-base disturbances as metabolic or respiratory, evaluating compensation and identifying mixed acid-base abnormalities. Key steps in ABG interpretation are outlined, such as using the anion gap and osmolal gap to identify causes of metabolic acidosis.

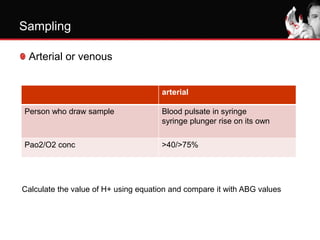
![Sampling
Steady state of oxygenation
10 min (healthy)
20 min (COPD)
Site (order of choice) (Don’t forget to apply LA)
Radial (check for collateral)
Dorsalis pedis
Bracheal
Femoral
Arterialized ear lobe samples: in neonate/small children
AARC Clinical Practice Guideline. RESPIRATORY CARE [Respir Care 1992(8);37:891–897]](https://image.slidesharecdn.com/abganalysis3-230327111153-f7ccbee5/85/ABG-Analysis-3-pptx-4-320.jpg)



![Volume of blood requirement: a
blood sample of 2-4 mL be drawn
After drawing the sample firm
pressure must be applied for at
least 2 min
Sampling
AARC Clinical Practice Guideline. RESPIRATORY CARE [Respir Care 1992(8);37:891–897]](https://image.slidesharecdn.com/abganalysis3-230327111153-f7ccbee5/85/ABG-Analysis-3-pptx-9-320.jpg)
![FREQUENCY:
depend on the clinical status of the
patient and the indication for
performing the procedure
Arterial line placed if>4 sample
drawn/day
not on an arbitrarily designated time
or frequency.
Sampling
AARC Clinical Practice Guideline. RESPIRATORY CARE [Respir Care 1992(8);37:891–897]
Browning JA, Kaiser DL, Durbin CG. The effect of guidelines on the appropriate use of arterial blood gas analysis in the intensive
care unit. Respir Care 1989; 34:269-276.](https://image.slidesharecdn.com/abganalysis3-230327111153-f7ccbee5/85/ABG-Analysis-3-pptx-10-320.jpg)




![Metabolic acidosis (high/normal AG)(step 6)
Anion gap or UA-UC = Na- Cl + HCO3
Normal range= 12±2 meq/l
Influence of albumin= for each gm decrease in albumin
AG decreases by 2.5
Adjusted AG= observed AG+2.5[4.5-albumin]](https://image.slidesharecdn.com/abganalysis3-230327111153-f7ccbee5/85/ABG-Analysis-3-pptx-25-320.jpg)