GEMC: Basics of Toxicology: Resident Training
•Download as PPT, PDF•
2 likes•1,027 views

This document provides an overview of toxicology basics for medical students. It discusses approaches to toxicology patients including decontamination techniques, common toxidromes like narcotic, sympathomimetic, anticholinergic, and cholinergic. It also reviews substances that cause each toxidrome and their treatments, emphasizing supportive care and specific antidotes when available. The goal is to recognize toxidromes, identify substances, and initiate appropriate emergency management of overdose patients.

Recommended
Recommended
More Related Content
Similar to GEMC: Basics of Toxicology: Resident Training
Similar to GEMC: Basics of Toxicology: Resident Training (18)
More from Open.Michigan
More from Open.Michigan (20)
Recently uploaded
Recently uploaded (20)
GEMC: Basics of Toxicology: Resident Training
- 1. Project: Ghana Emergency Medicine Collaborative Document Title: Basics of Toxicology Author(s): Patrick Carter, MD, University of Michigan Medical School License: Unless otherwise noted, this material is made available under the terms of the Creative Commons Attribution Share Alike-3.0 License: http://creativecommons.org/licenses/by-sa/3.0/ We have reviewed this material in accordance with U.S. Copyright Law and have tried to maximize your ability to use, share, and adapt it. These lectures have been modified in the process of making a publicly shareable version. The citation key on the following slide provides information about how you may share and adapt this material. Copyright holders of content included in this material should contact open.michigan@umich.edu with any questions, corrections, or clarification regarding the use of content. For more information about how to cite these materials visit http://open.umich.edu/privacy-and-terms-use. Any medical information in this material is intended to inform and educate and is not a tool for self-diagnosis or a replacement for medical evaluation, advice, diagnosis or treatment by a healthcare professional. Please speak to your physician if you have questions about your medical condition. Viewer discretion is advised: Some medical content is graphic and may not be suitable for all viewers. 1
- 2. Attribution Key for more information see: http://open.umich.edu/wiki/AttributionPolicy Use + Share + Adapt Make Your Own Assessment Creative Commons – Attribution License Creative Commons – Attribution Share Alike License Creative Commons – Attribution Noncommercial License Creative Commons – Attribution Noncommercial Share Alike License GNU – Free Documentation License Creative Commons – Zero Waiver Public Domain – Ineligible: Works that are ineligible for copyright protection in the U.S. (17 USC § 102(b)) *laws in your jurisdiction may differ Public Domain – Expired: Works that are no longer protected due to an expired copyright term. Public Domain – Government: Works that are produced by the U.S. Government. (17 USC § 105) Public Domain – Self Dedicated: Works that a copyright holder has dedicated to the public domain. Fair Use: Use of works that is determined to be Fair consistent with the U.S. Copyright Act. (17 USC § 107) *laws in your jurisdiction may differ Our determination DOES NOT mean that all uses of this 3rd-party content are Fair Uses and we DO NOT guarantee that your use of the content is Fair. To use this content you should do your own independent analysis to determine whether or not your use will be Fair. { Content the copyright holder, author, or law permits you to use, share and adapt. } { Content Open.Michigan believes can be used, shared, and adapted because it is ineligible for copyright. } { Content Open.Michigan has used under a Fair Use determination. } 2
- 3. Basics of ToxicologyBasics of Toxicology Medical Student LectureMedical Student Lecture SeriesSeries Emergency MedicineEmergency Medicine revised 6/2009 3
- 4. ObjectivesObjectives Describe the role of GI decontaminationDescribe the role of GI decontamination Recognize common toxidromesRecognize common toxidromes Recognize substances for whichRecognize substances for which specific antidotes existspecific antidotes exist Initiate ED management of a patientInitiate ED management of a patient with an overdosewith an overdose 4
- 5. The undifferentiated patientThe undifferentiated patient A patient is dropped off at the ED door.A patient is dropped off at the ED door. He is minimally responsive. His friendsHe is minimally responsive. His friends say they think he took something andsay they think he took something and drive off…drive off… Where do we start?Where do we start? 5
- 6. Approach toApproach to (possible)(possible) Tox patientTox patient Simultaneous treatment & diagnosisSimultaneous treatment & diagnosis Immediate action:Immediate action: ABC(D) , IV / O2 / monitorABC(D) , IV / O2 / monitor Thinking:Thinking: Is this a tox problem?Is this a tox problem? If yes, are there complicating factors?If yes, are there complicating factors? Got drunk and fell down, now with head injury?Got drunk and fell down, now with head injury? Resources to get a history?Resources to get a history? 6
- 7. Approach toApproach to (likely)(likely) Tox patientTox patient YouYou’ve considered a differential and you think’ve considered a differential and you think it is a toxicologic issueit is a toxicologic issue Immediate action:Immediate action: Supportive therapy (airway etc)Supportive therapy (airway etc) DecontaminationDecontamination Thinking:Thinking: Toxidrome present?Toxidrome present? What more information do I need?What more information do I need? Definitive ManagementDefinitive Management Is there an antidote or specific treatment?Is there an antidote or specific treatment? 7
- 8. Overdose HistoryOverdose History Time of ingestionTime of ingestion Talk to witnessesTalk to witnesses Get pill bottles &Get pill bottles & count!count! Assume commonAssume common co-ingestantsco-ingestants AlcoholAlcohol AcetaminophenAcetaminophen AspirinAspirin Jmh649, Wikimedia Commons 8
- 9. DecontaminationDecontamination GI exposureGI exposure Most common route (75% of toxic exposures)Most common route (75% of toxic exposures) Prevent absorptionPrevent absorption Topical exposuresTopical exposures Remove clothingRemove clothing Wash skinWash skin Enhance eliminationEnhance elimination Whole bowel irrigationWhole bowel irrigation SorbitolSorbitol Diuresis / ion trappingDiuresis / ion trapping HemodialysisHemodialysis 9
- 10. GI DecontaminationGI Decontamination ***Activated Charcoal******Activated Charcoal*** Absorbs up to 60% of ingestantAbsorbs up to 60% of ingestant 1 gm/kg +/- Sorbitol1 gm/kg +/- Sorbitol Maximal effect if given early (<1 hr)Maximal effect if given early (<1 hr) Will not bind – metals, electrolytes, acidsWill not bind – metals, electrolytes, acids ContraindicationsContraindications Depressed MS – Intubate to avoid aspirationDepressed MS – Intubate to avoid aspiration Bowel obstruction / perforationBowel obstruction / perforation Acid/ alkali ingestionAcid/ alkali ingestion 10
- 11. GI Decontamination –GI Decontamination – Rare interventionsRare interventions Gastric lavageGastric lavage Early presentation of potentially lethal ODEarly presentation of potentially lethal OD – e.g. tricyclics, iron, CCBs, B-blockerse.g. tricyclics, iron, CCBs, B-blockers High Risk – aspiration / perforation / airway compromiseHigh Risk – aspiration / perforation / airway compromise Syrup of Ipecac – Rarely used nowSyrup of Ipecac – Rarely used now Induces vomiting & eliminates less than charcoalInduces vomiting & eliminates less than charcoal Cardiomyopathy riskCardiomyopathy risk Whole bowel irrigationWhole bowel irrigation Sustained release preparationsSustained release preparations Body packersBody packers 11
- 12. 2 am Toxicology Resources2 am Toxicology Resources Poison ControlPoison Control 1-800-POISON11-800-POISON1 MicromedexMicromedex General drug infoGeneral drug info PoisindexPoisindex OverdoseOverdose managementmanagement IdentidexIdentidex Imprint identificationImprint identification Parhamr, Wikimedia Commons 12
- 13. Treatment Goals with ODTreatment Goals with OD ABCABC’s’s Identify (if possible) substancesIdentify (if possible) substances Reduce absorptionReduce absorption Enhance eliminationEnhance elimination Specific antidotes (if possible)Specific antidotes (if possible) Relatively few but important to knowRelatively few but important to know Supportive careSupportive care 13
- 14. ClassicClassic ToxidromesToxidromes Hint for exam:Hint for exam: Know theseKnow these 14
- 15. NarcoticNarcotic SympathomimeticSympathomimetic AnticholinergicAnticholinergic CholinergicCholinergic 15
- 16. NarcoticsNarcotics Natural & synthetic compounds whichNatural & synthetic compounds which mimic endogenous endorphinsmimic endogenous endorphins Heroin, Morphine, Dilaudid, Demerol,Heroin, Morphine, Dilaudid, Demerol, Vicodin, Methadone, Fentanyl (ChinaVicodin, Methadone, Fentanyl (China White), OxycontinWhite), Oxycontin Different pharmacologic parametersDifferent pharmacologic parameters Common drugs of abuseCommon drugs of abuse Street drugs – adulterated (mixed OD)Street drugs – adulterated (mixed OD) 16
- 17. Narcotics – Clinical pictureNarcotics – Clinical picture TempTemp HRHR RRRR PupilsPupils BSBS’s’s SkinSkin NarcoticNarcotic SympathomimeticSympathomimetic Anti-cholinergicAnti-cholinergic CholinergicCholinergic --- ↓ ↓↓ ↓↓ ↓↓ --- 17
- 18. Narcotics - treatmentNarcotics - treatment Support ABCsSupport ABCs Narcan 2mg IV q2min until effectNarcan 2mg IV q2min until effect Comes in 0.4mg vials!Comes in 0.4mg vials! Can require massive dosesCan require massive doses IV / IM / SQ / ET routesIV / IM / SQ / ET routes Short acting & may require repeatShort acting & may require repeat doses or IV dripdoses or IV drip 18
- 19. SympathomimeticsSympathomimetics Fight or flight systemFight or flight system Drug activate adrenergic nervousDrug activate adrenergic nervous systemsystem Cross-activation of dopaminergicCross-activation of dopaminergic euphoria & hallucinationseuphoria & hallucinations 19
- 20. TempTemp HRHR RRRR PupilsPupils BSBS’s’s SkinSkin NarcoticNarcotic ------ ↓↓ ↓↓↓↓ ↓↓↓↓ ↓↓↓↓ ------ SympathomimeticSympathomimetic Anti-cholinergicAnti-cholinergic CholinergicCholinergic ↑ ↑↑ --- --- sweaty↑ Sympathomimetics – clinicalSympathomimetics – clinical picturepicture 20
- 21. Common sympathomimeticsCommon sympathomimetics CocaineCocaine CaffeineCaffeine EphedrineEphedrine MDMA (ecstasy)MDMA (ecstasy) LSD (prominent hallucinations)LSD (prominent hallucinations) Pseudephedrine (Sudafed)Pseudephedrine (Sudafed) 21
- 22. Sympathomimetics - treatmentSympathomimetics - treatment ABCsABCs Supportive care / timeSupportive care / time Cocaine – avoid B-blockersCocaine – avoid B-blockers 22
- 23. Anticholinergic ToxidromeAnticholinergic Toxidrome Antagonism of the cholinergic nervousAntagonism of the cholinergic nervous system (parasympathetic)system (parasympathetic) Sympathetic disinhibition & loss ofSympathetic disinhibition & loss of parasympathetic functionsparasympathetic functions Common medication side-effectCommon medication side-effect Less commonly abused class of drugsLess commonly abused class of drugs 23
- 24. Anticholinergics - clinicalAnticholinergics - clinical picturepicture TempTemp HRHR RRRR PupilsPupils BSBS’s’s SkinSkin NarcoticNarcotic ------ ↓↓ ↓↓↓↓ ↓↓↓↓ ↓↓↓↓ ------ SympathomimeticSympathomimetic ↑↑ ↑↑↑↑ ------ ↑↑ ------ sweatysweaty Anti-cholinergicAnti-cholinergic CholinergicCholinergic ↑ ↑ --- ↓↓↓↓ dry↑ 24
- 25. AnticholinergicsAnticholinergics Blind as a bat (mydriasis)Blind as a bat (mydriasis) Hot as hare (flushed & warm)Hot as hare (flushed & warm) Mad as a hatter (delirium)Mad as a hatter (delirium) Dry as a bone (membranes & axillae)Dry as a bone (membranes & axillae) ““Can’t see, can’t pee, can’t s—t, can’tCan’t see, can’t pee, can’t s—t, can’t spit”spit” 25
- 26. Common anticholinergicsCommon anticholinergics AtropineAtropine AntihistaminesAntihistamines (Benadryl)(Benadryl) PhenothiazinesPhenothiazines (antiemetics)(antiemetics) TricyclicTricyclic antidepressantsantidepressants JimsonweedJimsonweed (Datura)(Datura) Denniss, Wikimedia Commons 26
- 27. Anticholinergics - TreatmentAnticholinergics - Treatment ABCsABCs DecontaminationDecontamination Supportive / timeSupportive / time Urinary drainageUrinary drainage 27
- 28. Cholinergic ToxidromeCholinergic Toxidrome Increased acetylcholine activityIncreased acetylcholine activity Nicotinic NS: increased nerveNicotinic NS: increased nerve transmission and muscle activationtransmission and muscle activation Muscarinic NS: liquid managementMuscarinic NS: liquid management Rarely abusedRarely abused Occupational exposures - insecticidesOccupational exposures - insecticides 28
- 29. Cholinergics – clinical pictureCholinergics – clinical picture Nicotinic effectsNicotinic effects Tachycardia, muscle fasciculations, weaknessTachycardia, muscle fasciculations, weakness (nerve transmissions can(nerve transmissions can’t get through),’t get through), respiratory depression, paralysis,miosisrespiratory depression, paralysis,miosis Muscarinic effects - SLUDGEMuscarinic effects - SLUDGE SalivationSalivation LacrimationLacrimation UrinationUrination DefecationDefecation GI upsetGI upset EmesisEmesis 29
- 30. Cholinergics – clinical pictureCholinergics – clinical picture TempTemp HRHR RRRR PupilsPupils BSBS’s’s SkinSkin NarcoticNarcotic ------ ↓↓ ↓↓↓↓ ↓↓↓↓ ↓↓↓↓ ------ SympathomimeticSympathomimetic ↑↑ ↑↑↑↑ ------ ↑↑ ------ sweatysweaty Anti-cholinergicAnti-cholinergic ↑↑ ↑↑ ------ ↑↑ ↓↓ drydry CholinergicCholinergic --- ↓↓ --- ↑↑ sweaty↓↓ 30
- 31. Common CholinergicsCommon Cholinergics OrganophosphateOrganophosphate insecticidesinsecticides Nerve gas (i.e. Sarin,Nerve gas (i.e. Sarin, VX)VX) Myasthenia GravisMyasthenia Gravis medsmeds ““Green tobaccoGreen tobacco sickness”sickness” Nicotine poisoning duringNicotine poisoning during harvestharvest 31
- 32. Cholinergics - TreatmentCholinergics - Treatment ABCsABCs DecontaminationDecontamination Atropine 2 mg q 5 minutes untilAtropine 2 mg q 5 minutes until secretions dry (massive doses)secretions dry (massive doses) Pralidoxime (2PAM) ifPralidoxime (2PAM) if organophosphatesorganophosphates Supportive care / timeSupportive care / time 32
- 33. Case 1Case 1 2 yo M got into older sister2 yo M got into older sister’s medication.’s medication. Mother brings to ED stating he’s had anMother brings to ED stating he’s had an allergic reactionallergic reaction P145 R25 T100.1 Skin flushed but noP145 R25 T100.1 Skin flushed but no urticaria or rash. Seems to be picking at theurticaria or rash. Seems to be picking at the air. Pupils dilated. Dry diaper.air. Pupils dilated. Dry diaper. Nurses requesting Benadryl for his allergicNurses requesting Benadryl for his allergic reaction.reaction. Is this a good idea? WhatIs this a good idea? What’s going on?’s going on? 33
- 34. Case 1 contCase 1 cont Anticholinergic toxidromeAnticholinergic toxidrome SisterSister’s medication’s medication DetrolDetrol AnticholinergicAnticholinergic Benadryl also anticholinergic!Benadryl also anticholinergic! Treatment?Treatment? 34
- 35. Case 2Case 2 15 people from a local government15 people from a local government building with vomiting and weakness.building with vomiting and weakness. 2 patients with respiratory distress2 patients with respiratory distress require intubation. Copious oralrequire intubation. Copious oral secretions are noted.secretions are noted. WhatWhat’s going on?’s going on? 35
- 36. Case 2 contCase 2 cont Cholinergic toxidromeCholinergic toxidrome SLUDGESLUDGE Nerve gas / deliberate exposureNerve gas / deliberate exposure 1995 – Sarin in Tokyo subway1995 – Sarin in Tokyo subway Treatment?Treatment? 36
- 39. AcetaminophenAcetaminophen CommonCommon “cry for help”“cry for help” UbiquitousUbiquitous Accidental ODAccidental OD’s – “multi-symptom cold meds”’s – “multi-symptom cold meds” Common co-ingestantCommon co-ingestant Initially asymptomatic or mild GI upsetInitially asymptomatic or mild GI upset Quiescent period of a few days afterQuiescent period of a few days after intoxication (LFTs may be elevated)intoxication (LFTs may be elevated) Delayed & sometimes fatal liver toxicityDelayed & sometimes fatal liver toxicity 39
- 40. AcetaminophenAcetaminophen Metabolite toxic to hepatocytes causingMetabolite toxic to hepatocytes causing hepatic necrosishepatic necrosis At therapeutic doses, glutathioneAt therapeutic doses, glutathione neutralizes metabolite and preventsneutralizes metabolite and prevents toxicitytoxicity At high doses glutathione depleted andAt high doses glutathione depleted and toxicity resultstoxicity results 40
- 41. AcetaminophenAcetaminophen Rumack-MatthewsRumack-Matthews NomogramNomogram Predicts hepaticPredicts hepatic toxicity based ontoxicity based on level and time oflevel and time of overdoseoverdose Toxic thesholdToxic theshold 140 mcg/ml140 mcg/ml Melrin Cyrstal, Wikimedia Commons 41
- 42. Specific intoxications: TylenolSpecific intoxications: Tylenol The rule of 140The rule of 140 Toxic dose is 140 mg/kgToxic dose is 140 mg/kg Toxic level at 4 hours is 140 mcg/mlToxic level at 4 hours is 140 mcg/ml First dose of NAC is 140 mg/kg poFirst dose of NAC is 140 mg/kg po (subsequent 17 doses are 70mg/kg)(subsequent 17 doses are 70mg/kg) If 15 kg child, how many ES TylenolIf 15 kg child, how many ES Tylenol pills (500 mg each) for toxic level?pills (500 mg each) for toxic level? 42
- 43. AcetaminophenAcetaminophen Treatment: N-acetylcysteineTreatment: N-acetylcysteine Replenishes glutathione in the liverReplenishes glutathione in the liver Tastes AWFULTastes AWFUL May require NGT administrationMay require NGT administration Newer IV form (Acetadote – 2004)Newer IV form (Acetadote – 2004) 43
- 45. SalicylatesSalicylates ASA, Peptobismol,ASA, Peptobismol, Oil of wintergreenOil of wintergreen 1 tsp = 7gm salicylate (peds lethal dose)1 tsp = 7gm salicylate (peds lethal dose) Symptoms onset within 1 hourSymptoms onset within 1 hour Enteric-coated delays absorptionEnteric-coated delays absorption Gastric bezoars also delay absorptionGastric bezoars also delay absorption Renal clearanceRenal clearance 45
- 46. SalicylatesSalicylates SymptomsSymptoms Vomiting, tinnitus, hyperpnea, fever (mild)Vomiting, tinnitus, hyperpnea, fever (mild) Acidosis, AMS, seizures and shockAcidosis, AMS, seizures and shock (severe)(severe) **Metabolic acidosis w/ respiratory**Metabolic acidosis w/ respiratory alkalosisalkalosis Toxicity begins at 50mg/kg (acute)Toxicity begins at 50mg/kg (acute) 46
- 47. Specific intoxications:Specific intoxications: SalicylatesSalicylates General guidelines for severityGeneral guidelines for severity Mild <300 mg /kg ingestedMild <300 mg /kg ingested Moderate 300-500 mg/kgModerate 300-500 mg/kg Severe / potentially lethal > 500 mg/kgSevere / potentially lethal > 500 mg/kg Serum level > 30 mg/dl at 6 hrs - toxicSerum level > 30 mg/dl at 6 hrs - toxic Done nomogramDone nomogram Historical interest onlyHistorical interest only Serum level not predictive of degree of toxicitySerum level not predictive of degree of toxicity 47
- 48. Salicylates - TreatmentSalicylates - Treatment Increased elimination in urineIncreased elimination in urine Urine alkalinizationUrine alkalinization 3 amps of bicarb in 1 L of D5W3 amps of bicarb in 1 L of D5W Hemodialysis indicated ifHemodialysis indicated if Coma, seizureComa, seizure Renal, hepatic, or pulmonary failureRenal, hepatic, or pulmonary failure Pulmonary edemaPulmonary edema Severe acid-base imbalanceSevere acid-base imbalance Deterioration in conditionDeterioration in condition 48
- 50. Tricyclic antidepressantsTricyclic antidepressants Depression, sleep, & pain disordersDepression, sleep, & pain disorders Less common due to SSRI prevalenceLess common due to SSRI prevalence High toxicity in overdoseHigh toxicity in overdose 50
- 51. Tricyclic antidepressantsTricyclic antidepressants Anticholinergic toxidrome plusAnticholinergic toxidrome plus Cardiac DysrhythmiasCardiac Dysrhythmias Quinidine-like (Ia) effects on Na channelsQuinidine-like (Ia) effects on Na channels Sinus tach, Vfib, VtachSinus tach, Vfib, Vtach SeizuresSeizures 51
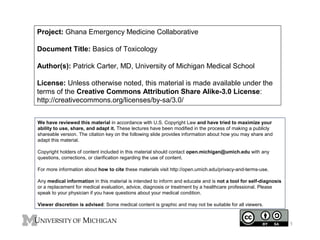
- 52. Tricyclic antidepressantsTricyclic antidepressants Screening EKGScreening EKG Widened QRSWidened QRS > 100ms – sz & dysrhythmia risk> 100ms – sz & dysrhythmia risk R wave in aVR and S waves in I, aVLR wave in aVR and S waves in I, aVL Prolonged QTcProlonged QTc 52
- 53. Electrocardiographic changes associated with tricyclic antidepressant overdose. The QRS complex is prolonged with delayed right ventricular activation and intraventricular conduction delay, which results in rightward shift in the terminal 40 msec frontal plane QRS vector. In qualitative terms, this shift manifests as a deep, slurred S wave in leads I and AVL, and an R wave in lead AVR (blue arrows). Source Undetermined 53
- 54. Tricyclic antidepressants - TxTricyclic antidepressants - Tx ABCsABCs Bicarbonate dripBicarbonate drip Reduces cardiac effectsReduces cardiac effects Control seizuresControl seizures BenzodiazepinesBenzodiazepines PhenobarbitalPhenobarbital Avoid phenytoin – risk of dysrhythmiasAvoid phenytoin – risk of dysrhythmias 54
- 55. Case 3:Case 3: 27 yo F brought in by family. Confused27 yo F brought in by family. Confused and vomiting.and vomiting. “She took some Tylenol“She took some Tylenol this morning” (about 4 hours ago)this morning” (about 4 hours ago) P125 BP135/65 T99.4 Warm, dry skin.P125 BP135/65 T99.4 Warm, dry skin. Oriented x 2. Sometimes nonsensicalOriented x 2. Sometimes nonsensical answers. +gag reflex. Dilated pupils.answers. +gag reflex. Dilated pupils. What do you need to know?What do you need to know? Does this fit with a Tylenol OD?Does this fit with a Tylenol OD? 55
- 56. Case 3Case 3 Gary Seidman, Flickr 56
- 57. Case 3Case 3 What are your initial orders?What are your initial orders? Hint: ABC, IV, O2, monitorHint: ABC, IV, O2, monitor What labs / tests do you want?What labs / tests do you want? Medications?Medications? 57
- 58. Case 3Case 3 Acetaminophen level – 375 mg/dlAcetaminophen level – 375 mg/dl What next?What next? 58
- 59. Case 4Case 4 32 yo M brought in because of violent32 yo M brought in because of violent behaviorbehavior Agitated and combativeAgitated and combative P125 BP 160/95 T99.4P125 BP 160/95 T99.4 Warm & sweaty. Dilated pupils. ExamWarm & sweaty. Dilated pupils. Exam otherwise non-focalotherwise non-focal Differential?Differential? 59
- 60. Case 4Case 4 UDS – cocaine positiveUDS – cocaine positive Treatment?Treatment? 60
- 61. Slides & content for this lecture developed by Stacey Noel, MD With revisions by Colin Greineder, MD & Laura Hopson, MD 61