
Recommended
More Related Content
What's hot
What's hot (20)
Similar to hodgkins lymphoma
Similar to hodgkins lymphoma (20)
Recently uploaded
Recently uploaded (20)
hodgkins lymphoma
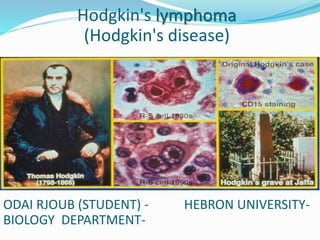
- 1. Hodgkin's lymphoma (Hodgkin's disease) ODAI RJOUB (STUDENT) - HEBRON UNIVERSITY- BIOLOGY DEPARTMENT-
- 2. Def: is a chronic ( in rare case acute) disease ,the growth of the tumor cells take place mainly in the lymphatic node. Hodgkin's disease, is a type of lymphoma, which is a type of cancer originating from white blood cells called lymphocytes.
- 3. History: It was named after Dr. Thomas Hodgkin, who first described abnormalities in the lymph system in 1832. Dorothy Reed and Carl Stenberg first described the malignant cells of Hodgkin’s lymphoma called Reed Stenberg cells. 1798-1866
- 4. Sign and symptoms:(Clinical features) Night Sweats Unexplained weight loss Lymph nodes: the most common symptom of Hodgkin's is the painless enlargement of one or more lymph nodes. The nodes may also feel rubbery and swollen when examined Splenomegaly: enlargement of the spleen occurs in about 30% of people with Hodgkin's lymphoma Hepatomegaly: enlargement of the liver
- 5. 1. Painless Lymphadenopathy – involving superficial lymph nodes of cervical and (Dsupraclavicular nodes) • The lymph nodes are swollen and have a rubbery feeling 2. Systemic Symptoms a) Fevers, Night Sweats and Weight Loss b) Pruritus c) Pel-Ebstein Fever e) cough and dyspnoea. 3. Pain a) Alcohol – induced pain b) Abdominal Pain c) Bone Pain d) Neurogenic Pain e) Back Pain f) chest pain
- 6. Famous People With Hodgkin's Disease: • Paul Allen- Investor and co-founder of Microsoft Corporation. • Charles Lindbergh- The first pilot to make a transatlantic flight. • Jackie Kennedy- Former First Lady • Gene Wilder- Actor
- 7. Causes: The exact cause of Hodgkin's lymphoma is unknown Hodgkin's lymphoma commonly begins in lymph nodes located in the upper part of your body. Some lymph nodes are in areas more readily noticed, such as in your neck, above your collarbone, under your arms or in your groin area. Enlarged lymph nodes in the chest cavity also are common. Eventually, Hodgkin's lymphoma may spread outside your lymph nodes to virtually any part of your body. A key step in Hodgkin's lymphoma involves the development of abnormal B cells.
- 8. REAL* Classification Classic: 1. Nodular Sclerosis 2.Lymhocyte rich 3. Mixed Cellularity 4. Lymphocyte depleted Non-Classic: Nodular lymphocyte predominant Hodgkins lymphoma (NLPHL)
- 9. Classic: 1.Nodular Sclerosis: Most common type diagnosed. About 70% of adolescents Lacunar cells are seen 40% of younger patients CD 15 and 30 positive EBV negative Only subtype without a male predominance Seen in younger pts with stage I – II disease
- 10. 2. Lymphocyte-Rich: This was introduced by the World Health Organization classification in 1999. RS cells CD15+, CD30+; 40% EBV+ Uncommon M > F Tends to be seen in older adults This is an uncommon form of classical HL
- 11. 3. Mixed Cellularity: Constitutes about 20% More common in young children CD 15,30 EBV positive Presents in advanced stages Tendency to involve spleen , bone marrow More than 50% present as stage III or IV disease Biphasic incidence, peaking in young adults and again in adults older than 55
- 12. 4. Lymphocyte depleted: Constitutes <5% RS cells CD15+, CD30+; most EBV+ Worst prognosis of all subtypes Present as febrile illness with pancytopenia, hepatomegaly, and no peripheral lymphadenopathy Older males , rare in children Advanced stage , Stage IV HIV infection
- 13. Non-Classic: Lymphocyte predominant Hodgkins lymphoma <5% of Hodgkins lymphoma Mainly involves cervical , axillary or mediastinal “L&H” cells or Popcorn cells are seen Positive for CD20,45 Negative for CD15,30.EBV
- 14. Ann Arbor Staging Classification for Hodgkin Disease: Stage I: Involvement of a single lymph node (1) or of a single extra lymphatic site or organ(1f) Stage II: Involvement of two or more lymph node regions on the same side of the diaphragm(II) or localised involvement of an extra lymphatic Site or organ and one or more lymph node regions on the same side of the diaphragm (IIf)
- 15. Stage III: Involvement of lymph node regions on both sides of the diaphragm (III) which may be accompanied by the involvement of spleen (IIIS) or by localized involvement of an extra lymphatic site or organ ( IIIf) or both ( IIIsf) Stage IV: Diffuse or disseminated involvement of one or more extra lymphatic organs or tissues with or without associated lymph node involvement. involvement of liver or bone marrow
- 16. Epidemiology: Most frequently (Bimodal)occur in age group 15 to 35 and >50 years More common in males except Nodular Sclerosis which is more common in females Increase incidence in HIV infections. Bimodal incidence Early peak middle to late 20s Second peak after 50 yearr Immunodeficiency
- 17. Sex (Male : Female) 4: 1 for 3-7 yr 3: 1 for 7-9 yr 1-3: 1 for > 10 yr 100 folds risk for unaffected monozygotic twin of affected twin Associated with specific HLA antigen Infectious agents Human herpes virus 6 CMV Epstein – Barr virus
- 18. Risk Factors Hodgkins: Family History Environmental – wood workers, farmers, meat workers Diseases- Mononucleosis (EBV infection), AIDS, Bone marrow transplant. HIV
- 19. Complication: Renal amyloidosis followed by contracted kidney and uremia Intoxication Septic complication Cardiovascular disease Second malignancy, such as leukemia, non-Hodgkin's lymphoma and tumors in the lungs, breasts or gastrointestinal system Vascular disease, including stroke Thyroid dysfunction Sterility
- 20. Diagnostic:
- 21. CBC LIVER FUNCTION RENAL FUNCTION SERUM ALBUMIN Serum Copper & Ferritin ESR LACTEATE DEHYDROGENASE BONE MAROW BIOBSEY
- 23. PET SCAN:
- 24. TREATMENT: Treatment depends on : Stage of the disease Age at diagnosis Presence / absence of B symptoms Presence of hilar lymphadenopathy Presence of bulky nodal disease Current Treatment Regimen: Combined chemotherapy with or without low dose involved field radiation therapy.
- 26. Radiotherapy: Radiation therapy is the most effective single thrapeutic agent for treating Hodgkin lymphoma. The main objective of radiation in Hodgkin lymphoma is to treat involved and contiguous field. Radiotherapy can be given by 1. 2D planning 2. 3D planning 3. IFRT Involved field radiotherapy is the most commonly used technique at present. It targets a smaller area rather than a classical extended field.
- 27. Conclusion: Radiation therapy is the most effective single therapeutic agent for treating Hodgkins lymphoma The management of Hodgkins lymphoma has evolved from extended field radiation to a combined modality of chemo radiation or chemo alone. Interest is in achieving the best therapeutic ratio by minimizing late toxicity while maintaining effectiveness. With improvement in diagnostic modality and PET scanning and improved treatment policy the results in future will be encouraging
- 28. IFRT Involved field radiotherapy. IFRT is the most commonly used technique at present Targets a smaller area rather than a classical extended field. IFRT(ASTRO 2002)DEFINITION IFRT encompasses region and not an individual lymph node. Initially involved Pre chemo sites and volume are treated Exception to above rule is for transverse diameter of mediastinum and paraaortic lymphnodes for which reduced post chemo volume is treated.
- 29. Thank you