
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Understanding Otitis Media: Causes, Symptoms and Treatment
Similar to Understanding Otitis Media: Causes, Symptoms and Treatment (20)
More from NEHA MALIK
More from NEHA MALIK (20)
Recently uploaded
Recently uploaded (20)
Understanding Otitis Media: Causes, Symptoms and Treatment
- 1. Otitis Media
- 2. Otitis media OT ‘GREEK WORD’ MEDIA LATIN WORD “ITIS” EAR INFLAMMATION SOMETHING THAT IS IN THE MIDDLE VIRUSES :-RSV(Respiratory syncytial virus) and ,INFLUENZA , and most likely to precipitate the condition
- 3. Most cases of Otitis Media occur in first 24months of life but the incidence decrease with age except for a small increase at the age 0f 5 to 6 years where children enter school. It don’t occur frequently in children older than 7, pre schooler boys get affected with this then pre schooler girls. Children who have a chronic family history of OM Children living with a large family that also have smokers in it have higher incidence rate of OM(passive smoking increases the risk of persistent middle ear effusion by enhancing attachment of the pathogen that causes otitis to the respiratory epithelium in the middle ear space, by prolonging the inflammatory response, and by impending drainage through the eustachian tube) Socio economic status and extent of exposure to other children
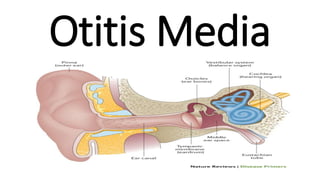
- 4. Basic Anatomy of Ear
- 5. PHYSIOLOGY OF EAR Through eustachian tube the nerve signals travels to the brain where they are then translated into recognizable and meaningful sounds. It is the brain that “hears”. Sound transfers into the ear canal and causes the eardrum to move The eardrum will vibrate differently with different sounds These sound vibrations make their way through the ossicles to the cochlea Sound vibrations make the fluid in the cochlea travel like ocean waves and created it into nerve impulses
- 6. Middle ear Cleft It can be thought as a miniature of lungs as it Allow for ventilation Pressure equilibrium Any problem in this area can cause ear pathologies
- 7. EUSTACHIAN TUBE FUNCTION 1.Equalibration of middle ear with atmospheric pressure 2. Protects middle ear from reflux of nasopharyngeal content 3. Drains secretions from the middle ear into the nasopharyngeal 1.INFECTION EUSTACHIAN TUBE OEDEMA ADENOIDS HYPERTROPHY 2.FAILING OF TENSOR VELI PALATINI LEVATOR VELI PALATINI
- 8. TENSOR VELI PALATINI LEVATOR VELI PALATINI OPENING EUSTACHIAN TUBE SWALLOWING YAWNING
- 9. ADULT EUSTACHIAN TUBE LONGER VERTICLE STIFFER LARGER PASSAGEWAY CHILD EUSTACHIAN TUBE SHORTER HORIZONTAL SOFTER SMALLER PASSAGEWAY All this allow an easy infection from the nasopharynx to the middle ear
- 11. Viral infection Congestion and edema Eustachian tube Occlusion -VE pressure in middle ear -ve Accumulation of fluid in the middle ear Acute otitis media Secondary viral or bacterial infection Increase pressure in middle ear Perforation in the tympanic membrane Suppurative Otitis Media OTORRHEA Chronic Suppurative Otitis Media Resolved Otitis Media
- 12. Acute otitis media Resolved Acute otitis media Otitis Media with Effusion Residual fluid in middle cavity after acute otitis media –mostly resolves on its own within 3 months and is asymptomatic Recurrent otitis media
- 13. Clinical manifestation OTALGIA FEVER HEARING LOSS OTORRHEA IRRITABILITY, LOSS OF APPATITE Otitis Media with Effusion It sometimes causes hearing loss because of the poor movements of auditory ossicles in an environment full of fluid ,hence it is a conductive hearing loss rather than a sensory neural hearing loss
- 14. Diagnosis OTOSCOPE BULDING EARDRUM AND BLOOD VESSELS IN Acute otitis media Suppurative Otitis Media Some practitioners also consider the presence of acute onset of less than 48 hours of ear pain with the Tympanic membrane revealing a purulent discolored effusion and a bulging and a reddened immobile membrane to be diagnostic factor in AOM.
- 15. Otitis Media with Effusion
- 16. Recently the concern about the drug resistant S Pneumonia and other drug resistances have led infectious disease authority to recommend careful and judicious use of anti-biotics for the treatment of the illness. healthy infants order than 6 months of age, without severe signs and symptoms Current literature indicates that waiting up to 72 hours for spontaneous resolution is safe and appropriate management of AOM children younger than 2 years with uncomplicated AOM. Some reviews of treatment reveals no clear evidence that antibiotics improves outcome children younger than 2 years who have persistent acute symptoms of fever and severe ear pain. The watchful waiting approach is not recommended. Oral amoxicillin in high dose (80-90mg/kg/day divided twice daily is the treatment of choice for initial episode of AOM.
- 17. In infants younger than 6 month should be treated with antibiotics because of their immature immune system and the potential for infection with bacteria. Antibiotic therapy in severe AOM is 10-14 days in children of the age 6 years & older with an uncomplicated AOM with a moderate and mild infection a 5-7 day course maybe sufficient. Second line antibiotics includes cephalosporin and injection and IM ceftriaxone is used of the causative organism is a highly resistance pneumococcus. Application of heat and cold and tropical pain relief drops. Antibiotics ear drops have no value in treating in AOM.
- 18. Otitis Media with Effusion Recurrent otitis media Hearing loss Developmental delays or learning difficulties Tympanostomy tube MYRINGOTOMY A SURGICAL INCISION IN THE EARDRUM IN CASE OF MASTODITIS AND FACIAL PALSY
- 19. A MINIMAL INVASIVE LASER ASSISTED MYRIGOTOMY PROCEDURE ADENOIDECTOMY IS ALSO PERFORMED IN RECURRENT CHRONIC OTITIS MEDIA