Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Case of Dimorphic Histoplasmosis in Vivo
Similar to Case of Dimorphic Histoplasmosis in Vivo (20)
More from mfabzak
Recently uploaded
Recently uploaded (20)
Case of Dimorphic Histoplasmosis in Vivo
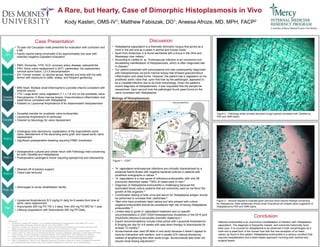
- 1. Kody Kasten, OMS-IV1; Matthew Fabiszak, DO1; Aneesa Afroze, MD, MPH, FACP2 Conclusion Infective endocarditis is an uncommon manifestation of infection with Histoplasma capsulatum. The diagnosis is frequently missed, and outcomes historically have been poor. It is unusual for Histoplasma to be observed in both morphologies as a mold and a yeast form in the human host with the rare exception of on heart valves, as found in this patient. Histoplasma endocarditis is a serious condition that requires hospitalization and a team-based approach involving both medical and surgical teams. A Rare, but Hearty, Case of Dimorphic Histoplasmosis in Vivo Figure 2 – Pathology slides showed abundant fungal hyphae consistent with Candida by PAS and GMS stains. Figure 3 – Second request to evaluate given previous bone marrow findings concerning for Histoplasma. Slide additionally shows small intracellular pill shaped yeast suggestive of Histoplasma by PAS and GMS stains. Case Presentation HPI Histories • PMH: Dementia, HTN, HLD, coronary artery disease, osteoarthritis • PSH: Aortic valve replacement in 2011, pacemaker, hip replacement, cervical spine fusion, L2-L5 decompression • SH: Former smoker, no alcohol abuse, Married and lives with his wife, farmer with exposure to cattle, sheep, and frequent gardening Outside Hospital • MRI Head: Multiple small bihemispheric punctate infarcts consistent with embolic source • TTE: Large aortic valve vegetation (1.1 x 1.6 cm) on the prosthetic valve • Pancytopenia Bone marrow biopsy: Granulomatous inflammation and yeast forms consistent with Histoplasma • Initiated on Liposomal Amphotericin B for disseminated histoplasmosis Transfer • Accepted transfer for prosthetic valve endocarditis • Liposomal Amphotericin B continued • Cleared by Neurology for valve replacement POD 0 • Undergoes redo sternotomy, explantation of the bioprosthetic aortic valve, debridement of the ascending aorta graft, and repeat aortic valve replacement • Significant postoperative bleeding requiring PRBC transfusion POD 1 • Intraoperative cultures and smear return with Pathology read concerning for both Candida and Histoplasma • Postoperative cardiogenic shock requiring epinephrine and dobutamine POD 3 • Weaned off of pressor support • Chest tube removed POD 12 • Discharged to acute rehabilitation facility Plan • Liposomal Amphotericin B 5 mg/kg IV daily for 6 weeks from time of aortic valve replacement • Itraconazole 200 mg PO TID x 3 days, then 200 mg PO BID for 1 year • Lifelong suppression with Itraconazole 200 mg PO Daily Discussion • Histoplasma capsulatum is a thermally dimorphic fungus that grows as a mold in the soil and as a yeast in animal and human hosts. • Apart from Antarctica, it is found worldwide with a focus in the Ohio and Mississippi river valleys.1 • According to Ledtke et. al, “Endovascular infection is an uncommon but devastating manifestation of histoplasmosis, which is often diagnosed late in disease.” • Our patient presented with pancytopenia and was subsequently diagnosed with histoplasmosis via bone marrow biopsy that showed granulomatous inflammation and yeast forms. However, the patient had a vegetation on his prosthetic aortic valve that, upon first look by the pathologist, appeared to be a Candida infection due to its mold morphology. Given the patient’s recent diagnosis of histoplasmosis, it was requested that the sample be reexamined. Upon second look the pathologist found yeast forms on the valve consistent with Histoplasma. • “H. capsulatum endovascular infections are clinically characterized by a subacute febrile illness with negative bacterial cultures in patients with prosthetic endographs or valves.”4 • “H. capsulatum is a rare cause of infectious endocarditis, with only 58 previously described cases.”6 85% of cases were in men.5 • Diagnosis of Histoplasma endocarditis is challenging because the automated blood culture systems that are commonly used do not favor the growth of this organism.5 • Combination testing of both urine and serum for Histoplasma antigen should be performed to increase their usefulness.5 • “Men who have prosthetic heart valves and who present with culture negative endocarditis should be considered high risk of having Histoplasma endocarditis.”5 • Limited data to guide H. capsulatum treatment and no specific recommendations in 2007 IDSA Histoplasmosis Guidelines or the 2015 joint IDSA/AHA Infective Endocarditis Scientific Statement.5 • Expert recommendations include initial period with Liposomal Amphotericin B 5mg/kg per day for 4-6 weeks with step-down therapy to Itraconazole for at least 12 months.5 • Isuvaconazole was used off label in one study because it doesn’t appear to have an interaction with warfarin, and it causes QTc interval shortening instead of lengthening like other azole drugs. Isuvaconazole also does not require renal dosing adjustment.6 References: 1. Armstrong PA, Jackson BR, Haselow D, et al. Multistate Epidemiology of Histoplasmosis, United States, 2011–20141. Emerging Infectious Diseases. 2018;24(3):425-431. doi:10.3201/eid2403.171258. 2. Benedict K, Thompson GR, Deresinski S, Chiller T. Mycotic Infections Acquired outside Areas of Known Endemicity, United States. Emerging Infectious Diseases. 2015;21(11):1935-1941. doi:10.3201/eid2111.141950. 3. Biology of Histoplasmosis. https://www.cdc.gov/fungal/diseases/histoplasmosis/causes.html. Accessed October 5, 2018. 4. Ledtke C, Rehm SJ, Fraser TG, et al. Endovascular Infections Caused by Histoplasma capsulatum: A Case Series and Review of the Literature. Archives of Pathology & Laboratory Medicine. 2012;136(6):640-645. doi:10.5858/arpa.2011-0050-oa. 5. Riddell J, Kauffman CA, Smith JA, et al. Histoplasma capsulatum Endocarditis: Multicenter Case Series with Review of Current Diagnostic Techniques and Treatment. Medicine. 2014;93(5):186-193. doi:10.1097/MD.0000000000000034. 6. Wiley Z, Woodworth MH, Jacob JT, et al. Diagnostic Importance of Hyphae on Heart Valve Tissue in Histoplasma Endocarditis and Treatment With Isavuconazole. Open Forum Infectious Diseases. 2017;4(4):ofx241. doi:10.1093/ofid/ofx241. Figure 1 – CDC3 • 70-year-old Caucasian male presented for evaluation with confusion and a fall • Family reports being chronically ill for approximately one year with relatively negative outpatient evaluation