Use of cellular phone contacts to increase return rates for immunization services
•
0 likes•577 views

Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Use of cellular phone contacts to increase return rates for immunization services
Similar to Use of cellular phone contacts to increase return rates for immunization services (20)
More from JSI
More from JSI (20)
Use of cellular phone contacts to increase return rates for immunization services
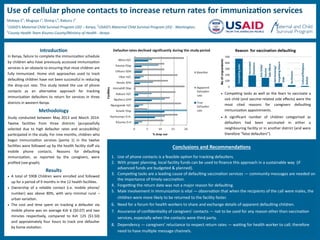
- 1. Use of cellular phone contacts to increase return rates for immunization services Mokaya E1 ; Mugoya I1 ; Shimp L2 ; Raburu J3 1 USAID’s Maternal Child Survival Program (JSI) – Kenya, 2 USAID’s Maternal Child Survival Program (JSI) - Washington, 3 County Health Team Kisumu County/Ministry of Health - Kenya Competingtasks Vaccinated Elsewhere SickChild/ Vaccine SideEffects NotKnowing/ ForgettingReturn Date NoReason Cultural/Religious Beliefs Introduction In Kenya, failure to complete the immunization schedule by children who have previously accessed immunization services is an obstacle to ensuring that most children are fully immunized. Home visit approaches used to track defaulting children have not been successful in reducing the drop-out rate. This study tested the use of phone contacts as an alternative approach for tracking immunization defaulters to return for services in three districts in western Kenya. Methodology Study conducted between May 2013 and March 2014. Twelve facilities from three districts (purposefully selected due to high defaulter rates and accessibility) participated in the study. For nine months, children who began immunization services (penta 1) in the twelve facilities were followed up by the health facility staff via mobile phone contacts. Reasons for defaulting immunization, as reported by the caregivers, were profiled (see graph). Results A total of 5908 Children were enrolled and followed up for a period of 9 months in the 12 health facilities. Ownership of a reliable contact (i.e. mobile phone/ number) was above 80%, with very minimal rural – urban variation. The cost and time spent on tracking a defaulter via mobile phone was on average Ksh 6 ($0.07) and two minutes respectively, compared to Ksh 125 ($1.50) and approximately four hours to track one defaulter by home visitation. Competing tasks as well as the fears to vaccinate a sick child (and vaccine-related side effects) were the most cited reasons for caregivers defaulting immunization appointments. A significant number of children categorised as defaulters had been vaccinated in either a neighbouring facility or in another district (and were therefore “false defaulters”). Conclusions and Recommendations 1. Use of phone contacts is a feasible option for tracking defaulters. 2. With proper planning, local facility funds can be used to finance this approach in a sustainable way (if advanced funds are budgeted & planned). 3. Competing tasks are a leading cause of defaulting vaccination services — community messages are needed on the importance of timely vaccination. 4. Forgetting the return date was not a major reason for defaulting. 5. Male involvement in immunization is vital — observation that when the recipients of the call were males, the children were more likely to be returned to the facility faster. 6. Need for a forum for health workers to share and exchange details of apparent defaulting children. 7. Assurance of confidentiality of caregivers’ contacts — not to be used for any reason other than vaccination services, especially when the contacts were third party. 8. Dependency — caregivers’ reluctance to respect return rates — waiting for health worker to call; therefore need to have multiple message channels.