
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to Anatomy of parapharyngeal space and its tumours
Similar to Anatomy of parapharyngeal space and its tumours (20)
Recently uploaded
Recently uploaded (20)
Anatomy of parapharyngeal space and its tumours
- 1. ANATOMY OF PARAPHARYNGEAL SPACE AND ITS DISEASE GUEST----- HOD AND PROFF DR KAVITA SACHDEVA MADAM SPEAKER-----DR JOSHNA THAKUR
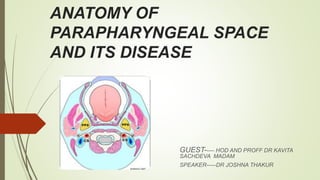
- 2. PARAPHARYNGEAL SPACE (lateral pharyngeal space, pharyngomaxillary space) It is classically described as an inverted pyramidal shaped potential space . Bounderies Base lies superiorly at the skull base and comprises the sphenoid and petrous portion of temporal bone . Apex ----inferiorly at the level of greater cornu hyoid bone. Medial surface---comprises superior pharyngeal constrictor muscle ,buccopharyngeal membrane and the pharynx. Lateral suface-----medial pterygoid muscle,the ramus of mandible,deep lobe of parotid gland and fascia of post. Belly of diagastric. Posterior surface----bordered by carotid sheath
- 3. FASCIAL CONDENSATION Two fascial condensation are present in parapharyngeal space 1. Aponeurosis of Zuckerkandl and Testut which divide the paraphyrngeal space into 2 compartment by joining the styloid process to the tensor veli palatini. 2. Second condensation of cervical fascia form a band which extend from styloid process to angle and post. Border of mandible and form a stylomandibular tunnel Tumors of deep lobe parotid gland can extend into parapharyngeal space through this tunnel giving rise to a dumbbell shaped tumour.
- 4. …
- 5. Compartment of parapharyngeal space COMPARTMENT VESSELS NERVES Others PRESTYLOID 1 Maxillary artery 2 Ascending pharyngeal artery 1 Auriculotempora l nerve 2 Lingual nerve 3 Inferior alveolar nerve. Fat,connective tissue, Deep aspect of parotid gland Lymph nodes POSTSTYLOID 1 ICA 2 Internal jugular vein 1 Cranial nerve 9th,10th,11th,12th, 2 Cervical sympathetic chain. Lymph node of glomus bodies
- 6. CLINICAL SIGNIFICANCE Radiological features----- Displacement pattern of fat and internal carotid artery within the space will aid in the localization of lesion. In prestyloid space lesion---mc associated with deep lobe of parotid gland and will deflect the carotid sheath and paraphyrngeal fat posterolaterally and may have a rim of fat anteromedially In poststyloid space lesion---- include neuroendocrine origin arising from carotid sheath as carotid body tumors or vagal schwannomas or neuroma of sympathetic chain.Lesion displaces parapharyngeal space fat and internal carotid artery anteromedially.
- 8. PRIMARY TUMOUR METASTATIC LESIONS MISCELLANEOUS 1 salivary gland tumour(benign and malignant SCC of nasopharynx lipoma 2Neurogenic neoplasm vagal schwannoma sympathetic chain Sch. vagal paragangliomas neurofibromas SCC of oral cavity sarcoma 3 Vascular and Lymphatic lesios ----- ---carotid artery aneurysm brachial cleft cyst --Hemangioma -- -A V malformation --Lymphatic malformation Carcinoma of oropharynx lymphoma Carcinoma of thyroid gland teratoma
- 9. Sign and Symptoms 1 Neck mass 2 Oropharngeal mass 3 Dyspnea 4 Cranial nerve deficit 5 Dysphgia or odynophagia may present. 6 Unilateral Conductive hearing loss due to ET blockage 7 Hoarseness of voice due to vagus nerve involvement 8 Horner syndrom due to sympathetic chain involvement 9 Rhinolalia clausia due to oropharyngeal component. 10 Trismus due to pterygoid muscle involvement. 11 Cranial nerve deficits 12 symptoms of catecholamines excess
- 10. … 13. tumor involve prestyloid area displace lateral pharyngeal wall and tonsil medially. lump behind the angle of mandible. 14. tumour involve poststyloid area fusiform appearance of tumour eg nerve sheath tumour. Intracranial extension via carotid canal ,jugular foramen,foramen ovale.
- 11. ....
- 12. ...
- 13. EXAMINATION Detailed head and neck examination. Cranial nerve examination. Bimanual palpation Bruit / thrill Carotid tumour moves side to side but fixed when moved up and down. Vitals ----blood pressure ,pulse rate,
- 14. Salivary gland neoplasms Neoplasms of salivary gland origin are located in the prestyloid parapharyngeal space (PPS) and account for 40-50% of PPS lesions. Salivary neoplasms may arise from the deep lobe of the parotid gland, ectopic salivary rests, or minor salivary glands of the lateral pharyngeal wall. The most common prestyloid PPS lesion is pleomorphic adenoma, which represents 45-64% of salivary neoplasms in the PPS. Common benign neoplasms include pleomorphic adenomas, monomorphic adenomas, Warthin tumors, and oncocytomas. Malignant neoplasms include adenoid cystic carcinomas, mucoepidermoid carcinomas, adenocarcinomas, and acinic cell carcinomas. Approximately 20% of all salivary lesions in the PPS are malignant, with carcinoma ex pleomorphic adenoma and adenoid cystic carcinoma being the most frequently reported.
- 15. SCHWANNOMAS Neurilemmomas, or schwannomas, arise from any nerve surrounded by Schwann cells and fibroblast supporting the nerve. Present in patients between 30 nd 70 yrs of age. In the PPS, the most common sites of origin are the vagus nerve and the sympathetic chain. They grow slowly and rarely cause palsy of the nerve of origin. Nerve paraesthesia common in these. Neurilemmomas are encapsulated and histologically distinct from the nerve itself. Treatment is by enucleation, and preservation of the nerve of origin is usually possible; however, every patient should be cautioned about the possibility of postoperative paralysis
- 16. PARAGANGLIOMAS Paragangliomas are benign vascular neoplasms that arise from the paraganglia or extra- adrenal neural crest tissue. Paraganglia function as chemoreceptors and are associated with the carotid body, the jugular bulb, and the vagus nerve in the poststyloid PPS. Highly vascular tumor. Carotid body tumors, glomus jugulare, and glomus vagale are slow-growing paragangliomas that may not produce symptoms may cause cranial nerve (CN) deficits, bone erosion, or intracranial extension as they increase in size. These are mobile in lateral direction not in cephalocaudal direction. Approximately 2% of head and neck paragangliomas secrete catecholamines and may cause paroxysmal symptoms of catecholamine excess.
- 17. .. Ten percent of paragangliomas are multiple and associated with paraganglioma at other locations. Ten percent of paragangliomas are hereditary, associated with a familial paraganglioma syndrome. ( genetic origin related to SHD sucinyl dehydroge gene locus) Head and Neck paraganglioma may also be associated with MEN 2a and MEN 2b syndromes Hypertension and flushing are suggestive of either a secreting paraganglioma or an associated pheochromocytoma. Malignant paragangliomas occur in less than 5-13.5% of patients and are associated with rapid growth and development of metastatic disease Carotid para ganglioma mobile in lateral direction but not in cephalocaudal direction , which differentiated it from lymph node.(fontaine sign)
- 18. CAROTID BODY TUMOUR Carotid body tumour, also known as a chemodectoma or carotid body paraganglioma, are highly vascular tumors arising from the paraganglion cells of the carotid body. These tumors are located at the site of the carotid bifurcation. Shamblin classification helps in predicting the prognosis and difficulties for surgical resection Shamblin classification Shamblin, et al. in 1971 classified carotid body tumors in relation to the carotid vessels. In his classification Group I – includes localized tumors not involving the carotid vessels. Group II – tumors partially surround carotid vessels or is adherent to them. Group III – defined as larger tumors encasing the carotid vessels. As carotid body tumors become larger in size they get more adherent to the vessels. However, Shamblin classification had some limitations because it does not reflect how deep tumor infiltrates through the wall of carotid vessels, which decides if it is possible to preserve the carotid vessels.
- 19. … Modified Shamblin classification Luna-Ortiz, et al. in 2006 proposed modifications to Shamblin classification, to improve the prediction of difficulties and complications. They introduced a class IIIa, representing the old class III, and a class IIIb which includes tumors of any class (I, II, or III) where there is infiltration of the vessel wall and not just circumferential encasement.
- 20. .. Need for vascular resection and reconstruction was significantly higher among class IIIb tumors.
- 21. .
- 22. NEUROFIBROMA Neurofibromas, in contrast, are unencapsulated and intimately involved with the nerve of origin. They may occur as a manifestation of the neurofibromatosis-1 (NF-1) syndrome. a disease in which the incidence of malignant transformation is increased. Cystic degeneration is common. The nerve of origin is usually sacrificed during excision to ensure complete removal of the neoplasm.
- 23. METASTASIS TO THE PARAPHARYNGEAL SPACE In parapharyngeal space lymph nodes are present which drain the mucosa of the upper aerodigestive tract and viscera of the neck . The most common metastasis to the parapharngeal space is from nasopharyngeal cancer . Nodes may also involved in tonsil and tongue base cancers and maxillary sinus cancer. Other primary sites include thyroid and parotid glands. Space may be directly invaded by malignancy from nasopharnx, tonsil, retromolar trigone, palate and tongue base.
- 24. Lymphoreticular lesions Lymphoreticular lesions make up 10-15% of PPS lesions. [3, 22] The lymphatics of the PPS may be involved primarily or secondarily by carcinoma, or they may be involved by infectious or inflammatory processes. Lymphoma is the most common malignant lymphoid process, but metastases from thyroid cancer, osteogenic sarcoma, squamous cell carcinoma, renal cell carcinoma, hypernephroma, and meningioma may also appear as PPS masses. The most common lymphoreticular lesions are lymphomas and metastases
- 25. INVESTIGATION Fine slice CT and MRI provides the detail reqired. MR Angiography and Carotid angiography provide information regarding vascularity and relationship to the neurovascular structures. FNAC BIOPSY ( EXCISIONAL , INCISIONAL—FROZEN SECTION,TRANSORAL FNAC IS SAFE AND INTRAORAL INCISIONAL BIOPSY MUST NOT BE CARRIED OUT.) BALLON OCCLUSION TEST 24 HOURS VMA(VANILLYLMANDELIC ACID) ---measures amount of VMA in urine over24 hr to detect excess epinephrine and norepinephrine. PLASMA CATECHOLAMINES LEVELS. METAIODOBENZLGUANIDINE SCAN. (MIBG) ---radioactive material injected intravenous ,which is takeup by tumour cells and this is sccaned by a scanner to locate and confirm the presence of tumour.
- 26. .. In imaging (MRI) paraganglioma gives salt and pepper appearance LYRE SIGN (splaying of internal and external carotid arteries) in vascular carotid body tumor. CT Scan shows evidence of bony details and erosion by these tumours. MRI Scan show soft tissue extension of these tumours including intracranial.extension. MRI Scan with gadolinium also show involvement of nerves and perineural spread..
- 27. .
- 28. .
- 29. .
- 30. .
- 31. .
- 33. PRE OPERATION Pre op counselling Preop embolization----------24 hrs prior to surgery, tumor >3cm with obvious feeding vessels Alpha blockers, Beta blockers------functioning paraganglioma.
- 34. SURGICAL APPROACHES FOR PARAPHARYNGEAL TUMOURS
- 36. 1 TRANSCERVICAL APPROACH It is the most commonly utilized approach.used in about 46% of cases. It is ideal for small benign tumors independent of deep lobe involvement of parotid gland. For poststyloid and prestyloid space tumours. Incision given 2 finger(5 cm) breadth below mandible. Submandibular triangle exposed (if needed) Facial nerve branches preserved. Facial artery ligated and divided. Submandibular gland retracted or excised. Digastric tendon divided Mandibulectomy done (if needed)
- 38. TRANSCERVICAL TRANSPAROTID APPROACH Next most common approach. Used in 27% cases. For lesion involve deep lobe of parotid tumours, vascular tumours. Doubly modified blair incision or slight anterior extension (in front of ear) of cervical incision i . Same procedure as in transcervical approach. Division of stylomandibular ligament ,styloglossus,stylohyoid muscle Deep parotid lobe tumours
- 39. MANDIBULOTOMY Transcervical and transcervical transparotid approaches can be combined with a mandibular osteotomy. Better visual asses to superior aspect of parapharyngeal space and the skull base. Inverted L OSTEOTOMY or double osteotomy above lingual and in front of the mental foramen to protect the inferior alveolar nerve. For excision of infiltrating malignancy and multifocal recurrent benign tumours.
- 40. TRANSORAL ROBOTIC SURGERY (TORS) 1 It has technical advantage ,it being the 3D high resolution image with magnification. 2 Scaled movement and tremor filtration allow for deldicated dissection around tumour capsule ensuring resection with a margin. 3 Ideal for benign salivary gland tumour in prestyloid space. 4 Absolute contraindication tumour that is adherent or involving the carotid artery, vascular tumor ,dumbbell tumor with significant involvement of deep lobe of parotid gland.
- 41. RADIOTHERAPY POST OP radiotherapy ---extensive malignant head and neck tumours Irresectable tumours. Control/ Arrest the growth of tumours. Nasopharyngeal tumour. Recurrent deep lobe of parotid tumour. Regional lymph node metastasis. Paraganglioma
- 42. CHEMOTHERAPY RHABDOMYOSARCOMA AND OTHER SARCOMAS NASOPHARYNGEAL TUMOUR. DOXORUBICIN---GLANDULAR TUMOUR CISPLATIN AND 5 FLUOROURACIL----SQUMOUS CELL TUMOURS
- 43. COMPLICATION VASCULAR INJURY CRANIAL NERVE INJURIES TUMOUR SPILLAGE AND RECURRENCE. FIRST BITE SYNDROME HEMATOMAS MARGINAL MANDIBULAR NERVE INJURY