Original Articles and Reviews
The Psychology of Euthanasia
Why There Are No Easy Answers
Miguel Ricou1,2 and Tony Wainwright3
1Faculty of Medicine, University of Porto, Porto, Portugal
2Department of Psychology and Education, Portucalense University, Porto, Portugal
3Department of Psychology, University of Exeter, UK
Abstract: Voluntary euthanasia has been legalized in several countries and associated with this development there has been much discussion
concerning the relationship between the ethical principle of autonomy and the respect for human life. Psychological science should make a
significant contribution to understanding how polarizing positions may be taken in such debates. However, little has been written concerning
the implications of this research for the euthanasia debate and about the contributions of psychology. In the same way, very little is written
about the psychologist’s role in countries where voluntary euthanasia or assisted suicide is legalized. We take as a starting assumption that
there are no solutions that will meet everyone’s wishes or needs, but that an understanding of psychological ideas, can assist in developing
strategies that may help people with opposing views come to some agreement. In our view, it is fundamental to a fruitful analysis, to leave
aside a polarized approach and to understand that an eventual answer to the question of how we approach voluntary euthanasia will only be
achieved after the hard process of carefully considering the consequences of having either legalized voluntary euthanasia or its prohibition, in
the context of a psychological understanding.
Keywords: euthanasia, suffering, psychology, ethics, decision-making
Voluntary euthanasia has been legalized in several coun-
tries,1 and in others it is being considered. This trend
toward legalization has led to much debate concerning
competing ethical principles (Youngner & Arnold, 2016).
As an example, in Portugal, where discussion about legisla-
tion has been in progress for some time, the head of Portu-
gal’s national nurses association alleged that euthanasia is
already being carried out, despite it currently being illegal
(https://www.bioedge.org/bioethics/nurse-ignites-debate-
over-euthanasia-in-portugal/11783) and this provoked
intense debate and criminal investigations into the medical
staff concerned.
There are clearly very strong feelings involved here, but
our contention is that there is no right or wrong answer. In
discussing the issues arising from ethics at the end of life, as
in the case of voluntary euthanasia2 or assisted suicide, our
contention is that taking an absolutist position – that there is
a “right or wrong” answer – will not be helpful. We intend
to outline the boundaries between the values or principles
that are in contention and to develop some ideas about
how these may be, at least partially, reconciled, using psy-
chological ideas as our framework.
When we consider the decision to end our life, either.
Original Articles and ReviewsThe Psychology of Euthanasia.docx
1. Original Articles and Reviews
The Psychology of Euthanasia
Why There Are No Easy Answers
Miguel Ricou1,2 and Tony Wainwright3
1Faculty of Medicine, University of Porto, Porto, Portugal
2Department of Psychology and Education, Portucalense
University, Porto, Portugal
3Department of Psychology, University of Exeter, UK
Abstract: Voluntary euthanasia has been legalized in several
countries and associated with this development there has been
much discussion
concerning the relationship between the ethical principle of
autonomy and the respect for human life. Psychological science
should make a
significant contribution to understanding how polarizing
positions may be taken in such debates. However, little has been
written concerning
the implications of this research for the euthanasia debate and
about the contributions of psychology. In the same way, very
little is written
about the psychologist’s role in countries where voluntary
euthanasia or assisted suicide is legalized. We take as a starting
assumption that
there are no solutions that will meet everyone’s wishes or
needs, but that an understanding of psychological ideas, can
assist in developing
strategies that may help people with opposing views come to
some agreement. In our view, it is fundamental to a fruitful
2. analysis, to leave
aside a polarized approach and to understand that an eventual
answer to the question of how we approach voluntary euthanasia
will only be
achieved after the hard process of carefully considering the
consequences of having either legalized voluntary euthanasia or
its prohibition, in
the context of a psychological understanding.
Keywords: euthanasia, suffering, psychology, ethics, decision-
making
Voluntary euthanasia has been legalized in several coun-
tries,1 and in others it is being considered. This trend
toward legalization has led to much debate concerning
competing ethical principles (Youngner & Arnold, 2016).
As an example, in Portugal, where discussion about legisla-
tion has been in progress for some time, the head of Portu-
gal’s national nurses association alleged that euthanasia is
already being carried out, despite it currently being illegal
(https://www.bioedge.org/bioethics/nurse-ignites-debate-
over-euthanasia-in-portugal/11783) and this provoked
intense debate and criminal investigations into the medical
staff concerned.
There are clearly very strong feelings involved here, but
our contention is that there is no right or wrong answer. In
discussing the issues arising from ethics at the end of life, as
in the case of voluntary euthanasia2 or assisted suicide, our
contention is that taking an absolutist position – that there is
a “right or wrong” answer – will not be helpful. We intend
to outline the boundaries between the values or principles
that are in contention and to develop some ideas about
how these may be, at least partially, reconciled, using psy-
chological ideas as our framework.
3. When we consider the decision to end our life, either in
the case of suicide or voluntary euthanasia, we are facing a
complex challenge that involves privileging one of at least
two main principles: the principle of autonomy which
may be seen as also promoting respect for human dignity;
or the principle of respecting life, also related to the princi-
ple of nonmaleficence (Beauchamp & Childress, 2001). It is
also the case that if you take the view, as we do, that there
are no absolute values or principles here, (see, e.g., (Engel-
hardt, 1999) the main decision for any society, is to draw a
conscious and considered boundary between these two cen-
tral values. Of course, many people hold that there are
absolute values or principles, as in the case of some faith
communities, but our view is that these can only be used
a guide, not a prescription in secular societies where many
faiths, and those with no faith, have to live together.
Here we explore the consequences of either undervalu-
ing the principle of autonomy, for example, in a society
where voluntary euthanasia as a personal choice does not
exist, and the parallel consequences where the value of life
may be thought to be diminished in society where voluntary
euthanasia is available as part of public policy.
1 In Europe Euthanasia and Assisted Suicide are legalized in the
Netherlands, Belgium, and Luxembourg. Also in Europe there
are two more
countries – Switzerland and Germany – with laws allowing
Assisted Suicide. In the rest of the World just in Colombia
Euthanasia and Assisted
Suicide are legal. In Japan, although there is not a law,
Euthanasia and Assisted Suicide are not illegal. Assisted
Suicide is also legal in Canada
and in five states of USA – Oregon, California, Colorado,
Washington, and Montana.
4. 2 Where we use the term euthanasia alone, we mean by this
voluntary euthanasia.
� 2018 Hogrefe Publishing European Psychologist (2019),
24(3), 243–256
https://doi.org/10.1027/1016-9040/a000331
T
hi
s
do
cu
m
en
t i
s
co
py
ri
gh
te
d
by
th
e
A
m
8. e
di
ss
em
in
at
ed
b
ro
ad
ly
.
This paper will also aim to explore the role that psychol-
ogy can play in helping an individual make the best deci-
sion, given their circumstances. There are very few
published studies about psychology and hastened death,
which is unexpected, given the importance of this area
for clinical practice. We believe psychology should play a
major role whether in the discussion of legalizing or not
euthanasia or assisted suicide, or in the work with people
who ask to die. Furthermore we will develop some ideas
on the role of the professional psychologist in this field.
Finally we hope to outline what psychology can contribute
to the development of public policy in this area.
Conceptualization and Definitions
9. It will be useful to introduce our argument with some his-
tory and some definitions. Euthanasia comes from two
Greek words: eu, meaning good, and thanatos, meaning
death. Contemplating this, we can say that, at least in its
original meaning, euthanasia refers the promotion of dying
as a good experience (as far as that is possible) and so
would include the idea of voluntariness as well as active
engagement, even when this involves the assistance of
another person.
From a historical point of view it is believed that Francis
Bacon was the first to write about euthanasia in a medical
context in 1605 where he says:
“Nay further, I esteem it the office of a physician not
only to restore health, but to mitigate pain and dolors;
and not only when such mitigation may conduce to
recovery, but when it may serve to make a fair and
easy passage.” (Bacon, 1605/2000, p. 100)
Over the years, attitudes to euthanasia have changed, and
particularly in Europe and the United States there have
been increasing numbers of jurisdictions making voluntary
euthanasia legal or at least decriminalizing it (Youngner &
Arnold, 2016).
One reason for the change in attitudes to voluntary
euthanasia has been the rapid advance in medical treat-
ment that has allowed life to be sustained much longer,
for example, through intensive care, than hitherto. This
has meant that increasing numbers of patients survive only
by being kept alive through artificial means and has pro-
duced situations in which ethical concerns raise major chal-
lenges (McDermid & Bagshaw, 2009). It has also been
argued that this shift in opinion reflects an even longer
trend that has seen science and technology offer meth-
10. ods for fixing the world’s problems and even death is
now seen as a possible fixable problem. Euthanasia could
then be viewed as consistent with this idea, that it provides
a way of controlling, if not preventing, death (Harari, 2016).
In the UK, there have been many debates and legal chal-
lenges to the current prohibition, but these have not been
successful (Bowcott, 2017).
Over 20 years ago, the UK House of Lords Select Com-
mittee on Medical Ethics, for example, made a clear dis-
tinction between prolonging life unnecessarily and the
voluntary refusal of treatment – orthothanasia – on the
one hand, and euthanasia on the other, and this distinction
has been maintained ever since: autonomy in refusing
treatment being maintained, but autonomy for receiving a
lethal drug, for example, being denied.
“With respect to euthanasia, may I first indicate
that in our deliberations we defined voluntary eutha-
nasia, at the request of the individual concerned, as
being a deliberate intervention undertaken with
the intention of ending a life so as to relieve intract-
able suffering; an act which must inevitably termi-
nate life. We were unanimous in concluding that
the right to refuse medical treatment is far removed
from the right to request assistance in dying.” (House
of Lords Selection Committee on Medical Ethics,
1994)
Defining Our Terms: Voluntary Euthanasia,
Nonvoluntary Euthanasia, and Involuntary
Euthanasia
There are some further distinctions that need to be made,
11. as they play an important role in debates and firstly we deal
with “voluntary euthanasia,” “nonvoluntary euthanasia,”
and “involuntary euthanasia.”
Voluntary euthanasia is performed with the consent of
the person. This is the term that we shall be using when
we discuss legalization later in this paper, as its fundamen-
tal purpose is to respect the wishes and autonomy of the
person concerned.
The second term is nonvoluntary euthanasia where the
person is not able to give consent. As a consequence it is
harder to argue that here autonomy is being respected.
However, in situations where the person lacks capacity,
for example, they are in a coma or a persistent vegetative
state, if food and fluids are withdrawn or life support is
turned off, the procedure can be described as nonvoluntary
euthanasia. This term is also commonly applied to cases in
which the person is a minor and may not be able to make
their own judgment. Usually, in these cases, it is the family
who ask for euthanasia, representing the person’s will. In
the same way, previously expressed wishes, as in advance
European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe
Publishing
244 M. Ricou & T. Wainwright, The Psychology of Euthanasia
T
hi
s
do
cu
m
16. ly
.
healthcare directives, can be on the basis of a nonvoluntary
euthanasia, if at the time the person lacks capacity.
The third term – involuntary euthanasia – refers to the sit-
uation where the person is killed against their expressed
will or, at least, without their consent. A major example
was the Nazi T4 or “Euthanasia Programme,” where many
disabled people were put to death, and indeed the first gas
chambers were used for killing people with a learning dis-
ability (Lifton, 1986). In more recent times the term has
been applied to cases of euthanasia where it is alleged that
consent was not given, or the person was not correctly
assessed, raising doubts about whether the persons con-
cerned had really expressed a wish to die (Singer, 2003;
Gillon, 1999). Our literature review suggests there is insuf-
ficient research on the psychological issues here, and that a
much fuller application of psychology in the debates on
how any policy is implemented, would be beneficial in
avoiding some of the risks of involuntary euthanasia taking
place. In the same way, it is possible to argue that when a
society accepts voluntary euthanasia, as time goes by, the
practice becomes more and more acceptable, so people
are not so strict with the criteria that are applied for some-
one to receive euthanasia (Pelligrino, 1998). In that way,
voluntary euthanasia slides to involuntary euthanasia. We
will come to this issue when discussing the idea of a “slip-
pery slope.”
Active Euthanasia, Passive Euthanasia,
Orthothanasia, Disthanasia, and
17. Physician-Assisted Suicide
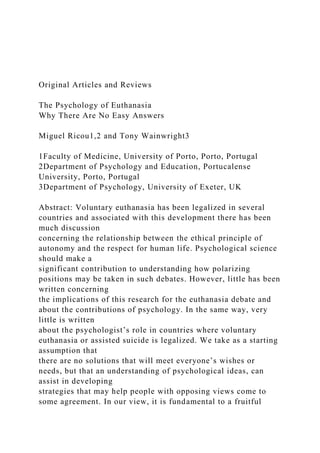
Finally there are some further terms that need to be made
clear for the purposes of our discussion; these are active
euthanasia, passive euthanasia, orthothanasia, disthanasia,
and physician-assisted suicide (Table 1).
In active euthanasia – a third person (usually a medical
professional) deliberately does something that causes the
person’s death – an act of commission. In passive euthana-
sia something is not done – an act of omission – whereby
the effect is the ending of the person’s life (an example of
this might be a patient refusing medical treatment that
would have kept them alive). The term orthothanasia (from
the Greek “normal death”) refers to a person’s right to
refuse treatment, even if this leads to their dying. The dif-
ference in meaning between passive euthanasia and
orthothanasia is that, in cases of passive euthanasia, people
do want to die, while in cases of orthothanasia people do
not want to die, per se, but rather want to deal with the neg-
ative effects or consequences of their treatment or condi-
tion. This difference makes it easier in general for people
to accept the latter as ethically justified, and goes some
way to explain why orthothanasia is usually legally accepted
and passive euthanasia is not (Singer 1995).
Another term that it will be useful to be clear about is dis-
thanasia (from the Greek “bad death”). This refers to the
situation, for example, where a person’s life is prolonged,
perhaps against their will, through what may be regarded
as disproportionate means, perhaps causing a person with
an incurable condition additional and unnecessary suffer-
ing. Disthanasia can be therefore understood in some ways
as standing as the opposite of voluntary euthanasia as it
may extend suffering instead of promoting its end by a
18. “good death.” Of course, disthanasia is an unacceptable
practice in health care.
The final term we would like to introduce is physician-
assisted suicide. This describes the situation where a doctor
provides a patient with the means to end their own life but
Table 1. Definitions
Person
asks to
die
Person
doesn’t ask
to die
because
he/she
is not
autonomous
Person
doesn’t
ask to
die
Person
doesn’t want
to die,
but refuses
treatment*
Someone
kills the
patient
19. The patient
kills
themself
with help
Death
resulting
from
withholding
treatment
Prolonging
life with
disproportionate
means
Active voluntary euthanasia X X
Passive voluntary euthanasia X X
Active nonvoluntary euthanasia X X
Passive nonvoluntary euthanasia X X
Active involuntary euthanasia X X
Passive involuntary euthanasia X X
Orthothanasia X X
Dysthanasia X
Physician-assisted suicide X X
*Usually legal in most countries.
20. � 2018 Hogrefe Publishing European Psychologist (2019),
24(3), 243–256
M. Ricou & T. Wainwright, The Psychology of Euthanasia 245
T
hi
s
do
cu
m
en
t i
s
co
py
ri
gh
te
d
by
th
e
A
m
er
24. di
ss
em
in
at
ed
b
ro
ad
ly
.
takes no part in its administration – this being left to the
patient themselves. Some have argued that from an ethical
perspective, physician-assisted suicide and voluntary eutha-
nasia are much the same (Brock 1995; Dixon 2012), since
in situations where the administration of medication is
the means of dying, whether it is administered by the doc-
tor or by the patient, from an ethical perspective, makes lit-
tle difference. Those who are in favor of physician-assisted
suicide argue that in these circumstances, the patient is the
ultimate cause of their own death, and this ensures that it
really is their decision – that they were clearly motivated
to take their own life. In the same way the possibility of sub-
tle coercion, error, and other abuses are reduced (Battin
1991; Quill, Cassel, & Meier 1996).
One issue that these definitions have in common con-
cerns the motivation of the person concerned and raises
25. an important question of how can this be assessed. How
sure can we be that the person is motivated to die for the
“right” reasons and not being pressured into it by others,
or by a mistaken belief that this is the only course open
to them? Research on those who narrowly escape killing
themselves in suicide attempts support the idea that people
can change their minds and often do (Seiden, 1978); but for
those who are successful, there is no way of knowing of
course.
Nevertheless, we can argue that those who defend
assisted suicide, as a way to ensure that the person’s moti-
vation is fully engaged with dying, is to admit that in gen-
eral, it is hard to be sure what someone’s real reasons are
when they are asking to die. We will come back to that
when we will be discussing the role of psychology.
Euthanasia – Potentially Conflicting
Values
Values and Social Norms
The question of euthanasia and human rights, their rela-
tionship with personal values, and how they may come into
conflict with each other, is an important theme in this dis-
course. In addition, social norms change as societies
develop and the interplay between social norms and per-
sonal values is an important further consideration. In gen-
eral, societies across the world and their associated
cultures have been evolving in a way that promotes human
rights in many different ways and so the discussion of
euthanasia is often located in that framework, that is, a dis-
cussion about rights (Pegram, 2015).
The first of these personal values is dignity and there has
been an increasing focus on people’s dignity, and other
26. rights, that enlarge a person’s opportunity to differentiate
themselves from others, and to assert their own individual
identity (Pinker, 2011). In such a framework, each individ-
ual is taught that they are unique, making them the only
one who truly knows what is best for them. One of the con-
sequences of this is that when we are faced with a situation
where we are trying to judge what is best for another per-
son, it means accepting and respecting the other person’s
will and also their autonomy, and only by doing this will
we be treating them with dignity (Ricou, Sá, & Nunes,
2017).
Another fundamental value that is clearly important in
this context is how we judge the importance or indeed
the value of human life. It is a truism to say that people
in general appreciate and value their lives, so it is almost
impossible to imagine a modern society where human life
is not respected. In fact, if people did not cherish life in their
social relationships, the social order would swiftly break
down. So in the context of this discussion of euthanasia,
we are proposing that there are two central values that
are in play: dignity (that is operationalized as respect for
autonomy) and respect for human life.
Absolute and Relative Values
Whether values are regarded as absolutes or change
depending on circumstances has a significant impact on
ethical decision-making (Neumann & Olive, 2003). Taking
the position that there are absolute values or principles is to
accept that there are absolute right things and absolute
wrong things, which is contrary to the global consensus that
people have different world views. Of course, respecting
differences does mean accepting that we live in a world
where people with absolute values and people with more
27. relative values will need to coexist.
In clinical practice, given this situation, professionals
working with absolute principles will find particular ethical
challenges, since they will need to work with everyone
including those whose values differ from their own (Page,
2012). Beauchamp and Childress (2001), in their moral
common theory, talk about middle-level principles. These
are principles that can be considered absolutes, except
when they conflict between each other. When they do con-
flict, the professional should analyze the situation and
define which principle should be, in that particular situa-
tion, prioritized, and should try to reach some form of
resolution.
As argued later in this paper, in the case of euthanasia,
there is a conflict between the principle of autonomy and
the principle of nonmaleficence; neither one nor the other
can be treated as an absolute, but they are extremely
European Psychologist (2019), 24(3), 243–256 � 2018 Hogrefe
Publishing
246 M. Ricou & T. Wainwright, The Psychology of Euthanasia
T
hi
s
do
cu
m
en
t i
32. important. Our main goal is to understand the possible
implications of the overvaluing of one principle compared
to the other. What can happen if we overvalue autonomy
compared with nonmaleficence when accepting euthana-
sia? On the other hand, if we overvalue nonmaleficence,
are we being paternalistic? And how can we evaluate people
to understand if what they are expressing represents his or
her best interest?
In conclusion, if we accept that there are no absolute
principles, the role of the health professional is to choose,
in each particular case, which principle should be priori-
tized. Because the values we are talking about (value of
autonomy and value of life) are strongly endorsed in con-
temporary western societies, with differing views about
how they should be implemented, it is not reasonable to
leave these decisions alone to the health professional. The
legal system is the vehicle through which such competing
views can be regulated that provides the overall framework.
The best law needs to take account of the possible conse-
quences of the different possible choices and we explore
that in the remainder of this paper.
Respecting Autonomy
A psychologist, in the same way as a medical doctor, always
works intending the best outcome for his client or patient.
The difficulty is to understand, in these cases, what repre-
sents the best outcome, respecting life or respecting
autonomy.
It is known that well-being is highly related to the per-
son’s ability to adapt to new circumstances in life. When
33. something, like a terminal disease, happens in a person life,
suffering will prevail if the person is not able to adapt to the
new circumstances imposed. Respecting autonomy is
respecting the way the person thinks it will allow them to
adapt and have the chance of pursuing a fulfilling future.
In this way respecting someone’s autonomy is also a way
to promote the person adaptation, because only the person
knows the best way to adapt to the changes that have befal-
len them.
Nevertheless, whereas autonomy is an important guiding
principle, it is insufficient to capture the full range of com-
plex issues involved in end-of-life decision-making (APA,
2000). People change their minds often and there is sub-
stantial variation in the will to live which suggests that a
desire to die is inherently changeable (Maier & Newman,
1995; Chochinov, Tataryn, Clinch, & Dudgeon, 1999); there
are emotional states that can interfere with people’s deci-
sions; we know people can be rational but the decision pro-
cess is not simple and involves many, sometimes
competing, variables (Haidt, 2001; Damásio, 2010). The
decision to commit suicide is a good example of the
difficulty we face in understanding if a person’s decision
always represents the best decision as we know from psy-
chological science that decision-making under stressful cir-
cumstances is subject to biases that may not lead to the best
outcome (Mather & Lighthall, 2012). Given this evidence-
base we believe that psychology has a major role to play
here.
Euthanasia and Suicide – A Right or an
Absence of Choice
Euthanasia, Suicide, and Rights
Issues concerning euthanasia are closely connected with
34. those surrounding suicide. It is only in recent times that sui-
cide has been decriminalized in some countries and it is still
regarded as deeply wrong by many of the major world reli-
gions and indeed, perhaps because of this, religious belief
may act to reduce suicide risk (Cook, 2014; Lawrence,
Oquendo, & Stanley, 2016; Stack & Kposowa, 2011; Wu,
Wang, & Jia, 2015). So the question arises, should there
be a legal right to suicide? In most jurisdictions where it
is no longer a criminal offense, there is no right to suicide
as such. If we were to advocate for such a right, how would
we go about defining it? There would be strong views about
this on both sides, as some people would regard suicide as
acceptable as it would fit with their views about personal
autonomy, whereas others would regard it as, for example,
in the Catholic Church, as a Mortal Sin.
We believe, no matter the perspective someone can have
about suicide, that it would be possible for someone to want
to die (Schramme, 2013). So, the question should be if we,
as a society, should let people do it, or should we restrain
them, because it would be always impossible to know, for
sure, which people, between the ones who express the idea
of committing suicide, want really to die and which people
will change their minds.
Different Types of Suicide
One question that arises is whether there are different types
of suicide and we can turn to Durkheim’s classic study
(1897/2001) and list four types of suicide: egoistic, anomic,
fatalist, and altruistic. Considering this last, it becomes
obvious that suicide can have social motivations: the indi-
vidual kills himself due to a social cause which he/she con-
siders a more important value than his own life. In the case
of a suicide bomber carrying out a terrorist attack, for
instance, there is a belief in a more important value than
the innate wish to preserve one's own life (Joiner, 2014).
35. Given this, we can say that suicide may be a rational option;
a person may chose to die in a rational way.
� 2018 Hogrefe Publishing European Psychologist (2019),
24(3), 243–256
M. Ricou & T. Wainwright, The Psychology of Euthanasia 247
T
hi
s
do
cu
m
en
t i
s
co
py
ri
gh
te
d
by
th
e
A
39. b
e
di
ss
em
in
at
ed
b
ro
ad
ly
.
Sleek (1996) also states an important point regarding sui-
cide: when it is performed by individuals who live with an
incurable disease it can be seen as providing a sense of
comfort once it gives the patient the chance to choose the
moment he/she is going to die. In the opposite way, we also
know that, often, people claim they want to die and after all
they change their minds.
How Do We Know if Someone Would Regret Their
Decision if They Lived?
One key fact here is that most of the people with suicidal
intention, or even having attempted to kill themselves,
end up changing their minds (Maser et al., 2002). Only a
small minority go on to commit suicide (Klonsky, May, &
40. Saffer, 2016). However, of course, this data is compromised
as we cannot ask those who do commit suicide whether
they had a change of heart before they died.
Nevertheless, given this discussion, it is always possible
for a person to change their mind. They may wish to die
at a particular moment, but if they survive, they may be
very grateful. On the other hand, they may not, and telling
the difference between these two situations is very difficult.
From the evidence that we have, it is relatively common for
people to have second thoughts, so that it is clearly better to
err on the side of assuming that someone may change their
minds as if they do die, there is no chance to regret it or
otherwise.
The Role of Professionals
While there are no absolute methods for assessing a person
wishes and whether they are likely to change their minds
concerning their wish to die, psychologists always draw
on whatever scientific evidence is available to inform their
judgment; this means that their starting assumption is that
it would be highly probable that the person might wish to
die at one point in time but would be likely to change their
minds.
But this issue becomes more complicated for doctors.
Usually they are the only professional group that would
are legally accredited to perform euthanasia, where it is
legal3 (Pereira, 2011). And why is that? Medical codes of
ethics are clear; they must relieve a patient’s suffering
and/or cure them whenever possible. Therefore, when con-
fronted with a patient whose pain or disease cannot be
cured and they are likely to continue suffering despite treat-
ment, the doctor considering their obligation to relieve …
42. & Saydah, 1999). The trend has continued: From 1980 to
2005, life expectancy increased by nearly four years
(National Center for Health Statistics, 2010). Although
living longer is generally viewed as a blessing, society is
witnessing increased rates of chronic disease and termi-
nal illness as a result (National Center for Health
Statistics, 2010). Advances in medical technology can
often postpone these deaths, but many view a life pro-
longed by dialysis, ventilators, and feeding tubes as unde-
sirable (Sears & Stanton, 2001).
In the United States, people are increasingly express-
ing an interest in controlling the way their lives end should
they be diagnosed with a terminal illness or chronic con-
dition that yields a poor quality of life (Cerminara &
Perez, 2000). As a result, every state has legalized advance
directives, which allow individuals to specify the circum-
stances in which particular life sustaining treatments may
be refused or withdrawn, ensuring that their wishes are
respected in the event they are rendered incompetent to
make their own medical decisions (Sears & Stanton,
2001; Werth, Lewis, & Richmond, 2009).
Physician assisted suicide (PAS) and euthanasia are
alternative end-of-life decisions. PAS and euthanasia
both hasten the death of an individual, but the two con-
cepts meaningfully differ in the role of the physician
(Cerminara & Perez, 2000; Sears & Stanton, 2001).
Physicians carrying out a request for PAS provide indi-
viduals with the means, generally prescription medica-
tion, to end their life; individuals decide if and when to
use the means. Euthanasia indicates cases in which the
physician administers the lethal dose of medication with
the intention of killing the patient (Cerminara & Perez,
2000; Sears & Stanton, 2001).
43. This review examines PAS from both legal and ethical
perspectives, and discusses issues related to assessment of
competence in patients requesting PAS in an effort to
clarify the role and duties of psychologists participating
in competence evaluations. The practice of PAS is widely
considered to be a criminal offense; however, the practice
is currently legal in Oregon, Washington, and Montana
(Oregon Death with Dignity Act [ODDA], 1995;
Washington Death with Dignity Act [WDDA], 2008;
Baxter v. Montana, 2009). PAS is also a highly controver-
sial topic from an ethical standpoint and the duties of
psychologists involved in the process remain unclear.
Thus, we present arguments regarding the rationality of
suicide as a framework for understanding the debate that
surrounds the acceptability of PAS. We include a review
Received 29 September 2012; accepted 6 June 2013.
Address correspondence to Shara M. Johnson, Department of
Psychology, Sam Houston State University, Huntsville, TX
77341.
E-mail: [email protected]
THE ROLE OF AND CHALLENGES FOR PSYCHOLOGISTS
583
of the ambiguous ethical obligations of psychologists
involved in PAS. In addition, guidelines for psychologists
tasked with determining competence are critiqued, and
we offer practical suggestions for completing the evalua-
tion. Lastly, we identify areas for future research to
improve PAS competence evaluations.
44. PHYSICIAN ASSISTED SUICIDE LEGISLATION:
CRITERIA AND THE ROLE OF MENTAL HEALTH
PROFESSIONALS
In 1994, voters passed the ODDA (1995), which became
available for use at the end of 1997 following a failed
attempt to have the law repealed (Werth, Benjamin, &
Farrenkopf, 2000). To qualify for PAS, an individual must
be (a) a resident of Oregon (Oregon Revised Statute [ORS]
127.860 § 3.10), (b) at least 18 years old (ORS 127.805 §
2.01), (c) terminally ill, which two physicians agree will
result in death within 6 months (ORS 127.820 § 3.02), and
(d) making an informed decision (ORS 127.830 § 3.04).
Furthermore, (e) the individual must make three requests
to his or her attending physician, two oral and one written
(ORS 127.840 § 3.06). The oral requests must be made at
least 15 days apart, and an additional waiting period of 48
hr must pass between the written request and the prescrip-
tion (ORS 127.850 § 3.08). Lastly, (f) the physician must
offer to stop the process following the second oral request,
which the individual must refuse (ORS 127.845 § 3.07).
According to ODDA, to receive the life ending pre-
scription, the patient must be considered to be making an
“informed decision,” which is
based on appreciation of the relevant facts and after
being fully informed by the attending physician of: a) his
or her medical diagnosis; b) his or her prognosis; c) the
potential risks associated with taking the medication to
be prescribed; d) the probable result of taking the medi-
cation to be prescribed; and e) the feasible alternatives,
including, but not limited to, comfort care, hospice care,
and pain control. (ORS 127.800 § 1.01.7)
45. As the law is written, a mental health professional
should only become involved in requests for PAS when
either the attending or consulting physician believes the
patient is “suffering from a psychiatric or psychological
disorder or depression causing impaired judgment” and
makes a “counseling referral” (ORS 127.825 § 3.03). It is
up to “the person performing the counseling” to deter-
mine that the patient is no longer suffering from the psy-
chological disorder causing impaired judgment and
capable of continuing with PAS. However, the definition
of capable provided by the ODDA, “the ability to make
and communicate health care decisions to health care
providers” is too vague to serve as a guide for psycholo-
gists asked to make such a determination (ORS 127.800 §
1.01; Werth et al., 2000). Guidelines do not exist and no
recent court cases have clarified what constitutes
decisional competency in PAS (Werth et al., 2000).
Two other states have followed Oregon. In 2008,
Washington voted to adopt an assisted suicide law
(WDDA, 2008). In 2009, the District Court of Montana
held that state residents’ constitutional rights of individ-
ual privacy and human dignity grant the right of a “com-
petent, terminally ill patient to die with dignity” (Montana
Death with Dignity Act [MDDA], 2009). The Montana
Court went on to permit patients to use the assistance of
their physician in obtaining a prescription for a lethal
dose of medication, but specified that the patient is
responsible for deciding to self-administer the medication
and induce death (Baxter v. Montana, 2009).
ARGUMENTS FOR AND AGAINST PAS
Understanding variant perspectives on suicide itself is
necessary to fully evaluate the ethical issues involved in
46. PAS. From a medical model, suicidal ideation is com-
monly considered symptomatic of mental illness and irra-
tionality (Sullivan, Ganzini, & Younger, 1998). As proof,
thoughts of death are listed among diagnostic criteria for
depression in the Diagnostic and Statistical Manual (4th
ed., text rev.; American Psychiatric Association, 2000),
much clinical literature is devoted to assessing and pre-
venting suicide (e.g., Bryan, Corso, Neal-Walden, &
Rudd, 2009; Cukrowicz, Wingate, Driscoll, & Joiner,
2004; Kleespies & Dettmer, 2000; Wingate, Joiner, Walker,
Rudd, & Jobes, 2004), and numerous organizations (i.e.,
American Association of Suicidology, American
Foundation for Suicide Prevention, and International
Association for Suicide Prevention) are committed to pre-
venting suicide (Silverman, 2000). Furthermore, the
implication that suicidal ideation indicates incapacitating
pathology extends into the legal arena and is used to jus-
tify involuntary commitment and mental health treatment
(Sullivan et al., 1998).
Although a wide body of research on suicide exists, it
focuses primarily on prediction and prevention; very little
conceptualizes suicide as a rational alternative (Werth,
1998; Widiger & Rinaldi, 1983). This emphasis likely
reflects a denial of circumstances that may render a life
no longer worth living and common fears about death.
Two arguments support suicide prevention. The first is
the link between suicidal ideation and psychopathology
(Widiger & Rinaldi, 1983). Indeed, presence of suicidal
ideation results in a lower Global Assessment of
Functioning score, which is a rating of psychological dys-
function. Suicidal behavior also mimics four features
common among mental disorders: the low base rate for
suicide represents a deviation from normal behavior, it is
viewed as undesirable by society, it is indicative of high
levels of distress, and it impairs functioning in one or
47. more domains (Widiger & Rinaldi, 1983). The second is
584 S. M. JOHNSON ET AL.
the ambivalence of the individual toward death.
Individuals who are in, or seek, treatment during their
suicidal crisis are perceived to be ambivalently committed
to ending their own life and receptive toward intervention
(Widiger & Rinaldi, 1983).
Belief in an inherent right to autonomy and acknowl-
edgement of the possibility that death can be a desirable
alternative to life are arguments used by those who lobby
for an acceptance of suicide (Silverman, 2000; Widiger &
Rinaldi, 1983). Autonomy proponents believe that indi-
viduals have the right to oversee their own goals and des-
tinies, which includes the manner and timing of their
death. They argue psychologists’ duty to commit or refer
a patient who is experiencing suicidal ideation fully
removes the autonomy from the patient so that the psy-
chologist assumes control over the suicidal patient
(Abeles & Barlev, 1999). They also point out that circum-
stances may arise in which the individual experiences
unbearable suffering or permanent impairment, and
death would be a merciful relief (Silverman, 2000;
Widiger & Rinaldi, 1983). From this perspective, there is
little perceived difference between PAS and acceptable
end-of-life alternatives, such as refusal or withdrawal of
life sustaining treatment (Jamison, 2000).
Opponents of PAS cite numerous concerns. One com-
mon argument is that PAS would be unnecessary if termi-
nally ill patients had adequate palliative care (Cerminara
& Perez, 2000; Jamison, 2000; Rosenfeld, 2000). It is
48. argued that more effective pain management for termi-
nally ill patients and additional social support for the
patient and family should be developed. Another fre-
quently cited argument against PAS is monetary; PAS is
less expensive than extensive palliative treatment and
might be more frequently used when medical resources
are scarce (Rosenfeld, 2000). Furthermore, it has been
theorized that should such a scarcity arise, PAS may be
used more frequently with members of vulnerable soci-
etal groups, such as minorities, individuals with disabili-
ties, and those of low socioeconomic status (Rosenfeld,
2000). Lastly, there is fear that legalizing PAS will lead to
a slippery slope in which euthanasia and assisted death
for patients not suffering from a terminal illness also
become legal (Rosenfeld, 2000). In fact, White and
Callahan (2000) proposed that “the most disastrous long-
term effect of legal PAS would be to legitimate suicide as
a socially acceptable way of dealing with pain and suffer-
ing of life and the end of life” (p. 333).
THE ROLE OF PSYCHOLOGISTS
The legal statutes recommend that a psychologist become
involved in PAS when there are concerns regarding the
patient’s decisional capacity due to the presence of psy-
chopathology, such as depression (ODDA, 1995; WDDA,
2008; MDDA, 2009). There appears to be a consensus
that the training psychologists receive in assessment,
psychopathology, and cognitive impairment qualifies
them to assist in determining whether a patient is capable
to consent to PAS (Farberman, 1997; Farrenkopf &
Bryan, 1999; Werth et al., 2000; Werth et al., 2009). It has
been proposed that psychologists with forensic training
may be uniquely qualified to evaluate competence
requests in PAS, given their training and experience with
49. issues related to competence and capacity (Ganzini,
Leong, Fenn, Silva, & Weinstock, 2000). Indeed, a survey
of forensic psychiatrists revealed that the majority had
professional experience with competence evaluations and
end-of-life decisions, with 74% having conducted compe-
tence evaluations for individuals refusing life sustaining
treatment, 54% having personally cared for a family
member or close friend who was suffering from a termi-
nal illness, and 67% having witnessed the suffering of a
dying family member or friend (Ganzini et al., 2000).
There is no consensus regarding the extent to which
the psychologist should be involved in the process and the
statutes provide no guidance aside from allowing for the
assessment. According to Farrenkopf and Bryan (1999),
when consulting on a case of PAS, the psychologist
should first clarify the reason for the referral, which may
be an evaluation of competence, but may also include
treatment of a disorder and treatment designed to
improve competence. In addition to performing the
assessment, Farberman (1997) proposed that psycholo-
gists serve as protectors of the patient’s rights and pro-
vide support for the patient’s family.
In a survey of Oregonian psychologists, further dis-
agreement regarding the psychologist’s role was revealed.
Sixty-two percent of those willing to perform the evalua-
tion indicated they would take no further action after
providing the referring physician with a report (Fenn &
Ganzini, 1999). However, 28% reported they would sup-
port the patient in completing the request, whereas 10%
reported they would actively work to prevent the suicide
(Fenn & Ganzini, 1999).
ETHICAL CONSIDERATIONS
FOR PSYCHOLOGISTS
50. Individual psychologists possess considerable freedom of
choice in regard to duties and involvement in PAS. Werth
and colleagues (2009) suggested there are no unique pro-
fessional or ethical considerations for a psychologist
working with a patient making end-of-life decisions
beyond the ethical concerns present with any client, but
our position is that the ambiguously defined and poten-
tially dynamic role could give rise to complex ethical
dilemmas.
One could construe the participation of psychologists as
a violation of Standard 3.04 Avoid Harm in the American
Psychological Association Ethics Code (APA, 2010); after
THE ROLE OF AND CHALLENGES FOR PSYCHOLOGISTS
585
required by using relevant research, training, consulta-
tion, or study” (APA, 2010, p. 5). Unfortunately, the lit-
erature offers few and often impractical suggestions for
psychologists conducting an evaluation for PAS.
PAS COMPETENCE EVALUATIONS
The concepts of capacity and informed consent are focal
points of a patient being competent to request PAS. In an
attempt to elucidate the potential roles and responsibilities
of psychologists who receive a counseling referral for a cli-
ent requesting PAS, we believe it beneficial to look to stan-
dards of competence in related domains (e.g., competence
to stand trial or consent to treatment). In addition, because
the state statutes specifically name depression as a psycho-
logical disorder believed to impair capacity, we address dif-
51. ficulties assessing depression in terminally ill patients. We
also provide a critique of protocols for assessment that
have been proposed in the literature.
Standards of Competence
A successful PAS requires an “informed decision” (ORS
127.800 § 1.01.7). Similarly, when mental health profes-
sionals assist in competence evaluations for purposes other
than PAS, such as competence to stand trial and compe-
tence to withdraw treatment, four elements are commonly
assessed: (a) the ability to communicate choice, (b) factual
understanding of information related to the decision, (c)
appreciation of the situation and possible consequences,
and (d) a rational understanding of information (Ganzini
et al., 2000; Werth et al., 2000). In addition, the psycholo-
gist is responsible for ensuring that patients are making the
request of their own volition (Werth, 1999).
Competence evaluations in other domains have estab-
lished precedents to be considered in PAS competence
evaluations. For example, assessments should begin with
the assumption that the individual is competent; therefore
the patient will only be rendered incapable of making deci-
sions should sufficient evidence exist (Werth et al., 2000).
Mere presence of a mental illness or history of mental
health treatment is insufficient to determine incompetence
(Werth et al., 2000). However, the profession of psychol-
ogy has long viewed suicidal ideation as not only a symp-
tom of mental illness, but also as justification for
involuntary hospitalization. Thus, psychologists may be
unprepared to perform the type of evaluation specified by
statutes legalizing PAS without better defined standards
for evaluations (Ganzini et al., 2000; Sullivan et al., 1998).
Although these precedents provide some basis for
52. what to consider in an assessment, the legal definition of
capacity remains vague and evaluators are responsible for
determining how to conduct an assessment and how
stringent of a standard to use in making a determination
(Werth et al., 2000). Unfortunately, forensic psychiatrists,
all, psychologists are typically required to intervene in cases
of suicidal crises. As APA has no official opinion regarding
the involvement of psychologists in PAS, psychologists
should carefully consider whether participation would vio-
late their professional responsibility to avoid harm. If upon
self-reflection the psychologist feels that participation
would violate personal or professional ethics and impair
objectivity, he or she must decline the task according to
Standard 3.06 Conflict of Interest (APA, 2010).
As the laws are written, it is unclear whether the client
being served is the patient making the request or the phy-
sician making the referral (Fenn & Ganzini, 1999).
According to Standard 3.07 Third-Party Requests for
Services, psychologists must clarify the nature and
bounds of relationships with everyone involved (APA,
2010). Properly defining the relationships will help the
psychologist adhere to Standard 3.05 Avoid Multiple
Relationships and Standard 4.01 Maintain Confidentiality
(APA, 2010).
Limits of confidentiality will vary depending on who
the client is. Should the physician be identified as the cli-
ent being served, the patient and patient’s family should
not receive direct communication from the evaluator
regarding the findings and any report generated should
be delivered directly to the physician (Fenn & Ganzini,
1999). Furthermore, identifying the client will also deter-
mine whether services in addition to the evaluation
should be rendered. Specifically, if the physician is the
53. client, then the patient and patient’s family will be ineli-
gible for treatment or intervention from the evaluator and
would need to seek their own service provider. Similarly,
it would be inappropriate for psychologists serving the
referring physician to then either become advocates for
the patient’s wishes or actively intervene in the patient’s
request, as they were hired as an objective evaluator
(Fenn & Ganzini, 1999).
An additional ethical concern pertains to Standard
2.01 Bounds of Competence, which indicates that psychol-
ogists should only provide services within their compe-
tence, “based on their education, training, supervised
experience, consultation, study or professional experi-
ence” (APA, 2010, p. 4). Some (33%) of Oregonian psy-
chologists surveyed felt that a competence evaluation for
PAS would fall outside of their area of practice; however,
60% reported that they would perform the evaluation
(Fenn & Ganzini, 1999). Although the general training
psychologists receive seems to qualify them for such an
evaluation, it is unlikely that they have enough training in
or exposure to geriatrics, end-of-life issues, the intersec-
tion of health and psychology, and the concept of capac-
ity to be truly competence in this domain. Standard 2.01
makes allowances for psychologists to work outside of
their area of competence to ensure individuals who
require mental health services are not denied, but only if
the psychologist has had related prior experiences and
“makes a reasonable effort to obtain the competence
586 S. M. JOHNSON ET AL.
that it is the loss of autonomy, as opposed to the physical
illness itself, which creates the desire for death.
54. An additional concern is that the methods commonly
used to identify depressive disorders may have less utility
when implemented with individuals suffering from grave
physical illnesses (Forkmann et al., 2009). Specifically,
the presentation of depressive symptoms may be due to a
genuine depressive disorder; however, effects of the illness
itself and even the palliative treatments can mimic symp-
toms of depression, particularly neurovegetative symp-
toms (Christensen & Ehlers, 2002). For example, patients
with end-stage renal disease often receive diagnoses of
depression; however, a number of the somatic symptoms
of depression (i.e., sleep disturbance, loss of appetite, and
cognitive deficits) are identical to the physical symptoms
of renal failure and effects of treatment (Christensen &
Ehlers, 2002).
Suggested Protocols for Assessment
Several authors have published suggestions for assessing
competence in patients requesting PAS, including neces-
sary qualifications for an evaluator, the number of inde-
pendent evaluators needed, and topics to review during
the assessment. In addition to the necessary training and
experience, Werth (1999) recommended that the psychol-
ogist should have general training in assessment, diagno-
sis, theories of individual and family therapy, death and
dying, hospice/palliative care, ethics, and medical/mental
health law. Ideally, the psychologist would also have prior
experience with individuals considering end-of-life alter-
natives (Werth, 1999).
In regard to general procedural guidelines for con-
ducting a competence evaluation for PAS, psychologists
should first ensure that the patient meets the require-
ments of the statute (Werth, 1999). The evaluator should
55. then review the patient’s record to become familiar with
the condition, prognosis, and treatment alternatives
(Farrenkopf & Bryan, 1999; Jamison, 2000). Suggested
topics to review in the interview with the patient, and
family if possible, include psychosocial history, patient’s
values, motivation for making the request, perceived
quality of life, patient’s description of physical condition
and treatment options, and certainty of decision
(Farrenkopf & Bryan, 1999; Jamison, 2000).
In 2000, Werth and colleagues published guidelines to
follow when conducting a competence evaluation for a
patient requesting PAS. They recommend exhaustively
reviewing medical records from past and current care
providers, using relevant objective assessment instru-
ments (i.e., depression and hopelessness inventories,
intelligence tests), conducting an extensive clinical inter-
view, and interviewing family and friends. Furthermore,
within each of these domains are long lists of specific
probes and rule out disorders. These guidelines intended
to synthesize components of competence evaluations
reported high standards for competence (Ganzini et al.,
2000). Specifically, 78% reported that a stringent stan-
dard should be set, even if some competent patients are
disqualified as a result. This directly contradicts the prec-
edent of basing the evaluation on assumed competence.
Also, psychiatrists who believed PAS to be unethical
favored stricter standards than those who believed PAS to
be acceptable in some or all circumstances, which sug-
gests personal bias may interfere with the assessment
(Ganzini, 2000).
Assessment of Depression
Although legal statutes allowing for PAS specifically cite
56. depression as a mental illness that could interfere with a
patient’s decisional capacity, the importance placed on
this diagnosis may be overemphasized (ODDA, 1995;
WDDA, 2008; MDDA, 2009). Although a mental illness
does not necessarily render an individual incompetent,
58% of forensic psychiatrists reported that major depres-
sion, in their opinion, would automatically classify a
patient as incompetent to make a request for PAS and
approximately 38% felt that less severe mood disorders
(i.e., dysthymic or adjustment disorders) were enough to
render a patient automatically incompetent (Ganzini
et al., 2000). Furthermore, personal values influenced
clinical decision making; psychiatrists who believed that
PAS was never acceptable were more likely to automati-
cally determine a patient with a mood disorder incompe-
tent (Ganzini et al., 2000).
There appears to be an assumption that terminally ill
patients are more disposed to symptoms of depression
and suicidal ideation than other patients due to the pain
and physical limitations inflicted by their medical diagno-
sis (Farberman, 1997). Indeed a positive association exists
between physical illness, symptoms of depression, and a
desire for death, creating complex cases for the consulting
psychologist (Breibart et al., 2000; Conwell et al., 2010;
Duberstein, Conwell, Connor, Eberly, & Caine, 2004).
However, it is likely that the patient’s personal values and
current behaviors are better indicators of suicide risk
(Farberman, 1997). Support for this hypothesis can be
found in public surveys regarding attitudes toward PAS.
Most people could envision circumstances in which PAS
would be acceptable, but those with higher religious con-
viction and abhorrence of suicide were consistently less
accepting and less likely to have considered PAS as a per-
sonal option (Achille & Ogloff, 1997; Wilson et al., 2007).
57. Autonomy is another personal value that likely con-
tributes to requests for PAS among terminally ill patients.
In one study, when functional impairments were added to
the regression model of physical illness and suicide, phys-
ical health no longer predicted suicide (Conwell et al.,
2010). In addition, severe physical illness, particularly
those necessitating in-home assistance, predict suicide
(Duberstein et al., 2004). Both of these results suggest
THE ROLE OF AND CHALLENGES FOR PSYCHOLOGISTS
587
shape their perspectives may increase the objectivity of
the evaluator and perhaps help correct for their biases. In
addition, psychologists may want to consult with col-
leagues following the evaluation. Discussing the data
gathered during the assessment with a party who is
removed from the immediate process may also help to
reduce potential bias.
FUTURE RESEARCH
The extent to which personal values of psychologists
appear to influence their decision making in competence
evaluations for PAS is concerning. In Oregon, six personal
values predicted opposition to PAS: no personal consider-
ation of PAS as an end-of-life alternative, belief that sui-
cide is an immoral act, belief in a physician’s duty to
preserve life, viewing patient autonomy and self-determi-
nation as less important than maintaining life, concern
about abuse, and younger age. Future research should sur-
vey psychologists about their personal values, professional
obligations in competence assessments, how they conduct
competence assessments for PAS, and any perceived ethi-
58. cal concerns, in addition to having participants make a
competence decision. Doing so would allow for analyses
to determine whether particular personal characteristics
of psychologists actually impact their decision making.
Also, developing a standard of practice for PAS is crit-
ical. These standards should be practical for use with
debilitated, terminal patients. The MacCAT-T should be
researched in the context of PAS as a possible structured …
34
Medical Ethics
and scientific communities and the right to
information about epidemics or outbreaks
of disease; persecution of health profession-
als for their independent medical or human
rights activities; attacks on health facilities
and personnel; medical evidence of torture
and sexual violence and their severe physi-
cal and psychological impacts; reproduc-
tive rights and health; collusion of health
professionals in human rights violations,
including torture and executions; overt ob-
struction of the right to health; discrimina-
tion within health systems; and much more.
PHR has submitted documentation to this
process on human rights violations in Bah-
rain, Myanmar, the United States and Zim-
babwe, among other countries.
Dozens of organizations worldwide regu-
59. larly send representatives to speak at Hu-
man Rights Council meetings on a range of
issues. But the credible and influential voice
of the medical community in these halls of
power is singularly underrepresented. PHR
has been opening a door to these opportu-
nities and welcomes company to develop a
more robust presence in Geneva as threats
against the independence of medical pro-
fessionals and the silencing of civil soci-
ety become ever more pervasive across the
globe.
Susannah Sirkin, Director of Policy,
Physicians for Human Rights
Ewan C Goligher Maria Cigolini Alana Cormier Sinéad
Donnelly Catherine Ferrier Vladimir A. Gorsh-
kov-Cantacuzène
Sheila Rutledge
Harding
Mark Komrad Edmond Kyrillos Timothy Lau Rene Leiva Renata
Leong Sephora Tang John Quinlan
Euthanasia and Physician-Assisted Suicide are Unethical Acts
The World Medical Association (WMA),
the voice of the international community
of physicians, has always firmly opposed
euthanasia and physician-assisted suicide
(E&PAS) and considered them unethi-
cal practices and contrary to the goals of
health care and the role of the physi-
60. cian [1]. In response to suggested changes
to WMA policy on this issue, an exten-
sive discussion took place among WMA
Associate Members. We, representing a
voice of many of those involved in this
discussion, contend that the WMA was
right to hold this position in the past and
must continue to maintain that E&PAS
are unethical.
The Central Issue Under Debate
is the Ethics of E&PAS
The question is whether it is ethical for
a doctor to intentionally cause a patient’s
death, even at his or her considered re-
quest. The fact that E&PAS has been
legalized in some jurisdictions and that
some member societies support these
practices has no bearing on the ethical
question. What is legal is not necessarily
ethical. The WMA already recognizes this
distinction, for example, by condemning
the participation of physicians in capital
punishment even in jurisdictions where
it is legal. The WMA should be consis-
tent in this principle also with respect to
E&PAS.
35
Medical Ethics
61. E&PAS Fundamentally
Devalues the Patient
This devaluation is built into the very
logic of E&PAS. To claim that E&PAS
is compassionate is to suggest that a pa-
tient’s life is not worth living, that her
existence is no longer of any value. Since
the physician’s most basic tasks and con-
siderations are to ‘always bear in mind
the obligation to respect human life’ and
‘the health and well-being of the patient’
[2, 3], E&PAS must be opposed. E&PAS
distorts the notion of respect for the pa-
tient. On the one hand it claims to help
suffering persons, while on the other hand
it eliminates them. This is a profound in-
ternal contradiction; the ethical priority
is to respect the fundamental intrinsic
worth of the person as a whole.
E&PAS Puts Patients at
Risk
Patients are autonomous agents but are
not invulnerable to their need for affirma-
tion from others, including their physi-
cian. Amidst the overwhelming fears of
those who suffer (4, 5), a free autono-
mous decision to die is an illusion. Par-
ticular concern exists for those who may
feel their life has become a burden due
to changing perceptions of the dignity
and value of human life in all its differ-
ent stages and conditions, and an explicit
or implicit offer of E&PAS by a physi-
cian profoundly influences the patient’s
own thinking. The troubles of human
62. relationships within families, the pres-
ence of depression, and problems of abuse
and physician error in an already stressed
medical system, make muddy waters even
more turbulent [6]. Evidence shows that
societies cannot always defend the most
vulnerable from abuse if physicians be-
come life-takers instead of healers [1, 6].
The power of the therapeutic relationship
cannot be underestimated in the creation
of patient perceptions and choices.
E&PAS Totally Lacks
Evidence as ‘Medical
Treatment’
The consequences of E&PAS are unknown
as both physicians and patients have no
knowledge of what it is like to be dead. Ad-
vocates of E&PAS place blind faith in their
own assumptions about the nature of death
and whether or not there is an afterlife
when arguing that euthanasia is beneficial.
E&PAS is therefore a philosophical and
quasi-religious intervention, not a medical
intervention informed by science. Doctors
should not offer therapy when they have no
idea of its effects—to offer E&PAS is to
offer an experimental therapy without any
plans for follow-up assessment. Therefore,
key elements in any medical intervention
such as informed consent are simply not
possible without knowing what stands on
the other side of death. Rather than a stan-
dard medical discussion of alternatives based
on scientific data or clinical experience, the
63. discussion must leave the clinical domain
and enter the domain of speculation. This
is not an exercise in informed-consent. This
is not the accepted medical ethics of medi-
cal practice. All this is, in part, why E&PAS
cannot be a medical procedure.
These Weighty Moral
Considerations are Supported
by the Ethical Intuition of the
Global Medical Community
Only a small minority of physicians sup-
port E&PAS. The vast majority of doctors
around the world wish only to foster the
will to live and to cope with illness and suf-
fering, not to facilitate acts of suicide or to
create ambiguity around what constitutes a
medical treatment. We must remember that
the four regional WMA symposia demon-
strated that most doctors would never be
willing to participate in euthanasia. Even
the insistence of E&PAS proponents on (a)
using ambiguous language such as ‘Medical
Assistance in Dying’ to describe their prac-
tice and (b) avoiding mention of E&PAS
on death certificates suggests that they
share to some degree this fundamental ethi-
cal intuition about killing patients.
Acceptance of E&PAS
Undermines Boundaries
Between End-Of-Life Care
Practices That do not Intend
Death (palliative care,
64. withholding/withdrawing life-
sustaining therapy) and Those
that do Intend Death (E&PAS)
Confusion is created at a societal level about
what constitutes “medical treatment,” espe-
cially when language such as “medical assis-
tance in dying” or “voluntary assisted dying”
is used. This renders the reality of such acts
and their application unclear. As many pa-
tients share our conviction that deliberately
causing death is wrong, a misunderstanding
of the distinction between E&PAS and pal-
liative care may lead to rejection of palliative
care or insistence on futile life-sustaining
therapies. The availability of E&PAS also
distracts from the priority of providing so-
cial services and palliative care to those who
are sick and dying [7].
The WMA’s Code of Ethics
Strongly Influences Standards
for the Practice of Medicine
Around the World and
Neutrality on E&PAS by the
WMA Would be Interpreted
Globally as Tacit Approval
A change in the WMA statement would
imply a tacit endorsement of E&PAS and
render the WMA complicit with such prac-
tices [8, 9]. Neutrality by professional medi-
36
65. cal organisations on E&PAS is perceived by
society, governments and the international
pro-euthanasia lobby as that organisation’s
acceptance of them as medical practice,
rather than as a response to a societal/po-
litical agenda. Those who seek international
approval to justify these practices will cre-
ate a silencing of the majority of the com-
munity, which has real medical, societal and
ethical concerns around E&PAS and their
effects on society internationally.
WMA policy on E&PAS reflects that
which is in place in hundreds of jurisdic-
tions with widely divergent legal and politi-
cal traditions. While it may be tempting to
placate some member societies so as to avoid
dissension, we must not destabilize medical
ethics around the world. We must continue
to characterize E&PAS as unethical even
if it conflicts with the demands of the state
or influential groups backed by the law. We
must not let imperfect law trump good
medical ethics. Undoubtedly many doctors
who perform E&PAS believe themselves
to be acting nobly; but it does not follow
that they should expect others to affirm
their views or not to oppose them; nor are
they wronged by existing WMA policy. Any
society that insists on transforming suicide
from a freedom to a right, should stand up
a different profession with the duty to fulfil
that new right, as killing does not belong in
the House of Medicine.
66. Neutrality on E&PAS
has Serious Consequences
for Physicians who
Refuse to Participate
In jurisdictions where E&PAS is legalized,
physicians who adhere to the long-standing
Hippocratic ethical tradition are suddenly
regarded as outliers, as conscientious objec-
tors to be tolerated and ultimately excluded
from the profession [10]. A neutral stance
by the WMA would compromise the po-
sition of the many medical practitioners
around the world who believe these prac-
tices to be unethical and not part of health
care. In some jurisdictions it is illegal not to
refer for these practices, creating a dystopic
situation where the doctor who practises
quality end-of-life care needs to conscien-
tiously object in order to do so, and may
be coerced to refer for E&PAS. Neutrality
from the WMA would promote the con-
travention of the rights and ethical practice
of these doctors, undermining their ethical
medical position at the behest of a societal
demand that can fluctuate with time.
In sum, the changes currently being de-
bated, arising from political, social, and
economic factors, have been rejected time
and again and most recently by the over-
whelming consensus of WMA regions. The
present debate represents a crucially im-
portant moment for the WMA that must
not be squandered. Given the influence of
67. the WMA and the profound moral issues
at stake, neutrality should not be an option.
The WMA policy must continue to stand
as a beacon of clarity to the world, bringing
comfort to patients and support to physi-
cians around the globe. The WMA should
not be coerced into promoting euthanasia
and assisted suicide by making its stance
neutral.
References
1. Leiva R, Friessen G, Lau T. Why Euthana-
sia is Unethical and Why We Should Name it
as Such. WMJ. 2018 Dec; 64 (4) pages 33-37.
[Cited 2019 Feb 05]. https://www.wma.net/wp-
content/uploads/2019/01/wmj_4_2018_WEB.
pdf
2. WMA INTERNATIONAL CODE OF
MEDICAL ETHICS. WMA [Internet] [cited
2019 Feb 05]. https://www.wma.net/policies-
post/wma-international-code-of-medical-
ethics
3. WMA DECLARATION OF GENEVA.
WMA [Internet] [cited 2019 Feb 05]. https://
www.wma.net/policies-post/wma-declaration-
of-geneva
4. Zaorsky NG et al. Suicide among cancer pa-
tients. Nat Commun. 2019 Jan 14;10 (1):207.
[cited 2019 Feb 05]. https://www.nature.com/
articles/s41467-018-08170-1
5. Rodríguez-Prat A et al. Understanding pa-
68. tients’ experiences of the wish to hasten
death: an updated and expanded systematic
review and meta-ethnography. BMJ Open.
2017 Sep 29;7(9):e016659. [Cited 2019 Feb
05].https://bmjopen.bmj.com/content/7/9/
e016659.long
6. Miller DG, Kim SYH. Euthanasia and physi-
cian-assisted suicide not meeting due care cri-
teria in the Netherlands: a qualitative review of
review committee judgements. BMJ Open. 2017
Oct 25;7(10):e017628. [cited 2019 Feb 05].htt-
ps://bmjopen.bmj.com/content/7/10/e017628.
long
7. The Canadian Society of Palliative Care Physi-
cians -KEY MESSAGES RE HASTENED
DEATH [Internet] [cited 2019 Feb 05]. https://
www.cspcp.ca/wp-content/uploads/2015/10/
CSPCP-Key-Messages-FINAL.pdf
8. Sulmasy DP, Finlay I, Fitzgerald F, et al. Phy-
sician-assisted suicide: why neutrality by organ-
ized medicine is neither neutral nor appropriate.
J Gen Intern Med 2018; 33: 1394-1399.
9. Canadian Medical Association softens stand on
assisted suicide. Globe and Mail. AUGUST 19,
2014 [Internet] [cited 2019 Feb 05]. https://
www.theglobeandmail.com/news/national/ca-
nadian-medical-association-softens-stance-on-
assisted-suicide/article20129000/
10. Euthanasia in Canada: A Cautionary Tale.
WMJ 2018 Oct; 64 (3), p 17-23. [cited 2019
Feb 05].https://www.wma.net/wp-content/up-
69. loads/2018/10/WMJ_3_2018-1.pdf
(Institutional affiliations are provided for
identification purposes only and do not im-
ply endorsement by the institutions.)
Ewan C Goligher MD PhD
Assistant Professor
Interdepartmental Division of
Critical Care Medicine
University of Toronto
E-mail: [email protected]
Dr Maria Cigolini
MBBS(Syd) FRACGP FAChPM
Grad.DiPallMed(Melb)
Clinical Director Palliative Medicine,
Royal Prince Alfred Hospital
Senior Clinical Lecturer,
University of Sydney
New South Wales, Australia
E-mail: [email protected]
Medical Ethics
https://www.wma.net/wp-
content/uploads/2019/01/wmj_4_2018_WEB.pdf
https://www.wma.net/wp-
content/uploads/2019/01/wmj_4_2018_WEB.pdf
https://www.wma.net/wp-
content/uploads/2019/01/wmj_4_2018_WEB.pdf
71. https://www.wma.net/wp-
content/uploads/2018/10/WMJ_3_2018-1.pdf
mailto:[email protected]
mailto:[email protected]
37
Alana Cormier MD CCFP
Family Physician, Twin Oaks
Memorial Hospital
Assistant Professor, Department of Family
Medicine, Faculty of Medicine, Dalhousie
University, Nova Scotia, Canada
E-mail: [email protected]
Sinéad Donnelly MD, FRCPI,
FRACP, FAChPM
Consultant physician Internal
Medicine and Palliative Medicine,
Module convenor and Clinical lecturer
Palliative Medicine, University Otago,
Wellington, Aotearoa New Zealand
E-mail: [email protected]
Catherine Ferrier, MD,
CCFP (COE), FCFP
Division of Geriatric Medicine,
McGill University Health Centre
Assistant Professor of Family
Medicine, McGill University
72. E-mail: [email protected]
Vladimir A. Gorshkov-Cantacuzène,
BChE, MNeuroSci, MD,
DSc(med), TD, JCD
Director, Department of Clinical
Cardioneurology, American Institute
of Clinical Psychotherapists
E-mail: [email protected]
Sheila Rutledge Harding, MD, MA, FRCPC
Hematologist, Saskatchewan Health Authority
Professor, College of Medicine,
University of Saskatchewan
Saskatoon SK Canada
E-mail: [email protected]
Mark Komrad MD
Faculty of Psychiatry Johns Hopkins,
University of Maryland, Tulane
Ethics Committee, American
College of Psychiatrists
E-mail: [email protected]
Edmond Kyrillos, MD, CCFP, B. Eng.
(Mechanical), Lecturer, Department
of Family Medicine, Faculty of
Medicine, University of Ottawa
E-mail: [email protected]
Timothy Lau, MD, FRCPC
73. Distinguished Teacher, Associate
Professor, Faculty of Medicine,
Department of Psychiatry, Geriatrics,
Royal Ottawa Hospital.
E-mail: [email protected]
Rene Leiva, MD CM, CCFP (Care of
the Elderly/ Palliative Care); FCFP
Assistant Professor
Department of Family Medicine
Faculty of Medicine
University of Ottawa
E-mail: [email protected]
Renata Leong
MDcM, MHSc, CCFP, FCFP
Assistant Professor, DFCM,
University of Toronto
E-mail: [email protected]
Sephora Tang, MD, FRCPC
Staff Psychiatrist, The Ottawa Hospital
Lecturer, Faculty of Medicine,
Department of Psychiatry
University of Ottawa
E-mail: [email protected]
John Quinlan MB.BS(Syd)
FAFRM MA(ethics)
74. E-mail: [email protected]
Defensive medical practice represents an
increasing concern in all over the world.
The practice of defensive medicine is main-
ly associated to the rising number of medi-
cal malpractice lawsuits. It negatively affect
the quality of care and waste the limited
resources in health sector. The economic
burden of defensive medicine on health
care systems should provide an essential
stimulus for a prompt review of this situ-
ation. Defensive medicine in simple words
is departing from normal medical practice
as a safeguard from litigation. The most
frequent daily practice of defensive medi-
cine is performing more unnecessary tests
and referring more patients to consultants
and hospitalization. Such behavior is an
ethically wrong and disagrees with deon-
tological duties of the doctor. Investigating
the prevalence of defensive medicine in a
number of international healthcare set-
tings, defensive medicine has been found
to be highly prevalent in many countries.
Majority of physicians across various spe-
cialties tends to adopt a defensive profes-
sional culture. Daiva Brogiene
Regional Medical Affairs
The Defensive Medicine isn’t the Best
Way to Avoid Mistakes
LITHUANIA
75. mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
mailto:[email protected]
Copyright of World Medical Journal is the property of World
Medical Association and its
content may not be copied or emailed to multiple sites or posted
to a listserv without the
copyright holder's express written permission. However, users
may print, download, or email
articles for individual use.
Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 1
3 , N U M B E R 1 1 – 1 2 , N O V E M B E R – D E C E M B
E R 2 0 1 6 ]12
ABSTRACT
Managing individuals with chronic
disorders of consciousness raises
ethical questions about the
76. appropriateness of maintaining life-
sustaining treatments and end-of-life
decisions for those who are unable to
make decisions for themselves. For
many years, the positions fostering
the “sanctity” of human life (i.e., life
is inviolable in any case) have led to
maintaining life-sustaining
treatments (including artificial
nutrition and hydration) in patients
with disorders of consciousness,
allowing them to live for as long as
possible. Seldom have positions that
foster “dignity” of human life (i.e.,
everyone has the right to a worthy
death) allowed for the interruption
of life-sustaining treatments in some
patients with disorders of
77. consciousness. Indeed, most ethical
analyses conclude that the decision
to interrupt life-sustaining therapies,
including artificial nutrition and
hydration, should be guided by
reliable information about how the
patient wants or wanted to be
treated and/or whether the patient
wants or wanted to live in such a
condition. This would be in keeping
with the principles of patient-
centered medicine, and would
conciliate the duty of respecting both
the dignity and sanctity of life and
the right to a worthy death. This
“right to die” has been recognized in
some countries, which have legalized
euthanasia and/or physician-assisted
78. suicide, but some groups fear that
legalizing end-of-life decisions for
some patients may result in the
inappropriate use of euthanasia, both
voluntary and nonvoluntary forms
(slippery slope argument) in other
patients.
This review describes the current
opinions and ethical issues
concerning end-of-life decisions in
patients with disorders of
consciousness, with a focus on the
impact misdiagnoses of disorders of
consciousness may have on end-of-
life decisions, the concept of
“dignity” and “sanctity” of human life
in view of end-of-life decisions, and
the risk of the slippery slope
79. argument when dealing with
euthanasia and end-of-life decisions.
We argue that the patient’s diagnosis,
prognosis, and wishes should be
by ROCCO SALVATORE CALABRÒ, MD, PhD; ANTONINO
NARO, MD, PhD;
ROSARIA DE LUCA, MS, PhD; MARGHERITA RUSSO, MD,
PhD;
LORY CACCAMO, PhD; ALFREDO MANULI, MS; ALESSIA
BRAMANTI;
and PLACIDO BRAMANTI, MD
Drs. Calabró, Naro, de Luca, Russo, Manuli, A. Bramanti, and
P. Bramanti are from the IRCCS
Centro Neurolesi “Bonino-Pulejo” in Messina, Italy; and Dr.
Caccamo is from the Department
of Psychology, University of Padua, Padua, Italy.
Innov Clin Neurosci. 2016;13(11–12):12–24
FUNDING: No funding was received for the
preparation of this article.
FINANCIAL DISCLOSURES: The authors have no
conflicts of interest relevant to the content of
this article.
ADDRESS CORRESPONDENCE TO:
Rocco Salvatore Calabrò, MD, PhD;
E-mail: [email protected]
80. KEY WORDS: Artificial nutrition and hydration;
euthanasia; minimally conscious state; right to
die; sanctity of life; vegetative state.
R E V I E W A N D C O M M E N T A R Y
The Right to Die in Chronic
Disorders of Consciousness:
Can We Avoid the Slippery
Slope Argument?
mailto:[email protected]
Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 1
3 , N U M B E R 1 1 – 1 2 , N O V E M B E R – D E C E M B
E R 2 0 1 6 13
central to determining the most
appropriate therapeutic approach
and end-of-life decisions for that
individual. Each patient’s diagnosis,
prognosis, and wishes should also be
central to legislation that guarantees
the right to die and prevents the
slippery slope argument through the
establishment of evidence-based
81. criteria and protocol for managing
these patients with disorders of
consciousness.
INTRODUCTION
Consciousness is the condition of
normal wakefulness (opening and
closing eyes, preserved sleep-wake
cycle) and awareness (of the self and
environment) in which an individual
is fully responsive to thoughts and
perceptions, as suggested by his or
her behaviors and speech.
1,2
A
disorder of consciousness (DOC)
results when awareness and/or
wakefulness are compromised
because of severe brain damage.
3
82. In recent years, the advances in
diagnostic procedures and intensive
care have increased the number of
patients who survive severe brain
injury and enter a vegetative state
(VS) (also recently named
unresponsive wakefulness
syndrome)4,5 or a minimally
conscious state (MCS). These
entities represent the two main
forms of chronic DOCs.
6–9
In
particular, patients suffering from VS
are unaware of the self and the
environment and cannot show
voluntary, purposeful behaviors
because of severe cortico-thalamo-
cortical connectivity breakdown
83. 10,11
that globally impairs sensory-motor
processing and cognition. On the
other hand, patients with MCS show
fluctuant but reproducible signs of
awareness and have a limited
repertoire of purposeful behaviors.
The best management of patients
in VS and MCS requires a correct
diagnosis, an evidence-based
prognosis, and the full consideration
of the medical, ethical, and legal
elements concerning DOC.
12
In
particular, patients with DOC need
artificial nutrition and hydration
(ANH) and, often, intensive
treatments. These issues evoke a
84. thorny ethical problem concerning
the therapeutic decision-making of
such patients (including the
continuation of life-sustaining
therapies) in view of the
uncertainties about their state of
consciousness, prognosis, and
personal wishes, with particular
regard to the end-of-life decisions
(ELD).
13
In fact, it is worth
remembering that the
implementation of any life-sustaining
treatment, including ANH, should
not be automatic when considering
that every individual should make his
or her own decisions regarding any
85. kind of therapy, according to the
ethical principles of autonomy and
the right of self-determination and
freedom. If an individual is unable to
make a decision, as in the case of
patients with DOC, a surrogate
should be empowered to ensure the
patient’s best interest and personal
wishes concerning ELDs. Therefore,
the right to lose health, become ill,
refuse treatment, live the end of life
according to one’s personal view of
life, and die should be guaranteed,
which is in keeping with human
dignity and the duty to protect
physical and mental health.
14
The right to die is further
supported by the following
86. arguments.
14–19
1. The right to (a worthy) life
implies the right to (a worthy)
death.
2. There is no reason to have a
“dedicated” right to die, given that
dying is a very natural
phenomenon, as is life.
3. Death is a private matter, and
other people have no right to
interfere if there is no harm to
others or the community (a
libertarian argument.
4. It is possible to regulate
euthanasia by proper laws, and
thus avoid the slippery slope
argument (SSA).
87. 3. Euthanasia may avoid illegal acts,
given that euthanasia may happen
anyway (a utilitarian or
consequentialist argument) and
save the extreme despair of
suicide or homicide.
6. Death is not necessarily a bad
thing, owing to the naturalness of
the phenomenon, regardless of
whether it is induced.
7. Euthanasia may satisfy the
criterion that moral rules must be
universalizable, but
universalizability is a necessary
but not a sufficient condition for a
rule to be morally good.
8. Medical resources can be better
managed, and though this is not a
88. primary reason for the right to
die, it is a useful consequence.
On the other hand, an opposite
view states that life is a unique and
incorruptible gift that, in keeping
with the concept of the sanctity of
human life, must always be
preserved. Hence, each individual
has the moral duty to attend to all
the treatment necessary to preserve
life, with the exception of those
burdensome and/or disproportionate
to the hoped for or expected result
(i.e., life preservation), and to avoid
behaviors that can deliberately
hasten or cause death.
13,19–24
A possible middle ground is
represented by the concept that the
89. sanctity and the dignity of life are
somehow coincident; consequently,
there is no reason why accepting
euthanasia makes some individuals
worth less than others. Since it is
possible to regulate euthanasia by
proper laws, there is no risk of the
following:
13,19–24
1. Starting an SSA that leads to
involuntary euthanasia, thus
killing people who are thought
undesirable
2. Less than optimal care for
terminally ill patients (for
economic reasons)
3. Giving too much power to medical
staff in limiting the access to
90. palliative and optimal care for the
dying, pain relief, saving lives,
using euthanasia as a cost-
effective way to treat the
terminally ill, and limiting the
research for new cures and
treatments for the terminally ill
Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 1
3 , N U M B E R 1 1 – 1 2 , N O V E M B E R – D E C E M B
E R 2 0 1 6 ]14
3. Exposing vulnerable people to
pressure to end their lives (duty
to die) by selfish families or by
medical staff to free up medical
resources or when patients are
abandoned by their families.
At first glance, the problem of
ELDs in patients with DOC may
91. seem easy to solve. The supporters
of the dignity of human life claim
that since patients with DOC are
unconscious and therefore cannot
fully benefit from their rights, ELDs
should assumed by a third party
(e.g., those with whom the patient is
familiar, medical staff, ethics
committees, or courts).25 These
parties would make the ELDs, taking
into account the best interests of the
patient, his or her wishes, the right
to freedom, and the respect of
human dignity. On the contrary,
those who advocate the sanctity of
life deny any possibility to hasten (by
interrupting life-sustaining
treatments) or cause death (by using
92. euthanasia and physician-assisted
suicide) (PAS), because they believe
that life preservation is a social and
ethical duty. Moreover, patients with
DOC are in a very frail and
vulnerable condition in which they
cannot express their thoughts on
these issues.13,19–24
Judgements in the Schiavo and
Englaro cases highlight this
controversy. In the Schiavo case,26
the argument was over whether Terri
Schiavo was in a persistent VS,
which had already lasted 15 years. It
began with her collapse in 1990, due
to cardiac arrest, and then her
husband’s initial court attempt to
have her feeding tubes removed in
93. 1998. That was followed by court
battles between the husband and
Schiavo’s parents, who opposed the
removal the feeding tube. Her
feeding tube was removed several
times and then reinserted after more
court orders. It was removed for the
last time in March 2005 after the last
successful court petition by the
husband. Schiavo died 13 days later.
Likewise, Eluana Englaro27
entered a persistent VS in 1992
following a car accident, and
subsequently became the focus of a
court battle between supporters and
opponents of euthanasia. Shortly
after her accident, medical staff
began feeding Englaro with a feeding
94. tube, but her father “fought to have
her feeding tube removed, saying it
would be a dignified end to his
daughter’s life.” According to
reports, Englaro’s father said that
before the car accident, his daughter
visited a friend who was in a coma
and afterward told him, “If something
like that ever happened to me, you
have to do something. If I can’t be
what I am now, I’d prefer to be left to
die. I don’t want to be resuscitated
and left in a condition like that.” The
authorities refused father’s request,
but the decision was finally reversed
in 2009, after she had spent 17 years
in a persistent VS.
Of note, the United States
95. Supreme Court has stated that the
irreversibility of a DOC condition and
the clearly defined patient’s wish to
not live under such conditions should
both be clearly demonstrated in
order to withdraw the sustaining
therapies, including ANH.28,29 These
decisions are fully in keeping with
the right of freedom and self-
determination and with the
supporters of the right to life.
However, these are fiercely criticized
and hindered by the sanctity of life
supporters.13,19–24
Therefore, we consider whether it
is more ethical to respect human
dignity than to protect the sanctity
of human life at all costs. A correct
96. approach to this thorny ethical
dilemma requires taking into account
that there is a tangible uncertainty of
DOC diagnosis and prognosis,
consequently making it more difficult
to respect a patient’s rights properly
when making ELDs. Moreover, it is
still debated whether ANH should be
considered a fundamental (i.e.,
always due) or an aggressive therapy
(i.e., useless and bearer of further
suffering).22,24,30–34 Finally, the
motivation sustaining the right to live
with dignity and in respect of human
life sanctity must be analyzed
carefully, given that the access to the
right to die is a SSA. In fact, both the
withdrawal and the maintenance of
97. ANH may lead to a chain of related
events that may culminate in some
significant and potentially negative
effects on patients with DOC (e.g.,
death or unnecessary and prolonged
suffering). Liberalizing euthanasia
may lead to unnecessary application
in some cases. The strength of each
argument in favor or against ELDs
depends on whether one can
demonstrate a process that leads to a
significant effect. SSAs can be used
as a form of fear mongering in an
attempt to scare the audience, thus
ignoring the possibility of a middle
ground between the dignity and the
sanctity of human life. In this article,
we will review the key concepts of
98. the positions supporting the dignity
and the sanctity of human life in an
attempt to find a conciliating view to
solve the SSA.
DOC DIAGNOSES AND
PROGNOSES
When family members are faced
with an irreversible and hopeless
case of unconsciousness, leaving
their loved one in such a condition
may be unbearable for both the
patient and his or her family
members. The relatives of patients
with DOC live a paradoxical reality.
In fact, they live with a family
member who is both present
(inasmuch as he or she is awake)
and absent (unaware) and alive
99. (inasmuch as he can open and close
his or her eyes, breathe
independently, and make some
movements) and dead (given that he
or she cannot interact with the
family members or the
environment).35–37 These issues can
foster denial or misunderstanding in
the family members of their current
situation. For example, they may
deny that their loved one is in a VS
because they interpret spastic or
reflexive movements as signs of
improvement,6 thus imagining
chances of recovery that are not
supported by evidence-based
medicine. Given that the family
100. Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 1
3 , N U M B E R 1 1 – 1 2 , N O V E M B E R – D E C E M B
E R 2 0 1 6 15
members may witness important
responses by the patient that have
not been observed by the clinicians,
the medical staff should attempt to
observe the patient with the family
members and involve them in the
patient evaluation. Assisting family
members in better understanding the
patient’s behaviors and level of
awareness is important and may
strengthen the family members’
relationship with the medical staff.38
Hence, the correct communication
of a proper diagnosis and a reliable
prognosis is essential for the best
management of a patient with DOC.
101. In fact, inaccurate diagnoses and
prognoses and disclosure of false
diagnostic information to families
may have serious ethical, medical,
and legal consequences regarding
the medical management of the
patient, the well-being of patient’s
family members, and ELDs.39,40 In
fact, an incorrect diagnosis and
prognosis may result in a false
expectancy for recovery by the
family members, the unnecessary
and potentially harmful life-support
prolongation of the patient, financial
and emotional resources being
withheld or withdrawn, resource
misuse and misallocation, and an
inappropriate rehabilitation or long-
102. term care facility enrollment.13
Nonetheless, identifying residual
awareness in unconscious patients
(thus differentiating VS from MCS)
and establishing a correct prognosis
are extremely challenging, owing to
the inadequate sensitivity of the
clinical and paraclinical approaches
currently available for DOC diagnosis
and prognosis.41–47 Even though the
rate of consciousness recovery varies
from eight percent to 72 percent
(but decreases to 20–30% in patients
persisting in comas longer than 24
hours),47 a severe brain injury may
result persistent unconsciousness for
many years. There have been cases
of emergence from DOC, even after
103. many years.48 Generally, recovery
from a metabolic or toxic coma is far
more likely than from an anoxic one
where the traumatic brain injury
(TBI) occupies an intermediate
prognostic position. A post-anoxic
coma is a state of unconsciousness
caused by global anoxia of the brain,
most commonly due to cardiac
arrest. The outcome after a post-
anoxic coma lasting more than
several hours is generally, but not
invariably, poor.47
About 40 percent of patients with
VS may be clinically misdiagnosed in
that they may be conscious but are
unable to manifest any signs of
consciousness.49–51 Such a condition
104. has been recently labeled functional
locked-in syndrome (FLIS),
whereby, using neurophysiological
and functional neuroimaging
approaches, clinicians are able to
record residual brain network
connectivity that is sustaining a
covert awareness.52 A patient with
FLIS is clinically similar to one with
VS, with the exception that the
former is aware of the self and the
environment but is unable to
demonstrate awareness or
communicate.6–9 This may due to the
deterioration of sensory-motor
processes, which support motor
function, rather than the breakdown
of cerebral connectivity.6–12,53,60
105. The low rate of correct diagnoses
and prognoses may depend on the
variations in scale application,
awareness fluctuation, and subjective
interpretation of clinical findings.
The use of paraclinical tests to
detect residual and covert signs of
awareness may help in better
managing patients with DOC and
consequently supporting their right
to ELDs. Nevertheless, different
paraclinical tests would be necessary
to confirm awareness since single
tests may suffer from the same
methodological bias that clinical
approaches do.39,40,54
ELDs AND THE DIGNITY OF
HUMAN LIFE
106. The thought of interrupting life-
sustaining treatments, including
ANH, may arise in family members
and caregivers when their loved one
suffers from a long-lasting and
potentially irreversible DOC
condition.34 The idea of hastening
one’s own death may occur when
one’s quality of life is poor or
unbearable (e.g., in the case of
physical pain and/or mental anguish)
and life is considered without dignity
(e.g., feeling there is no chance of
recovery, finding nothing that makes
life worth living, and perceiving life
as a burden to others).55–58 One might
consider that respecting the dignity
of life means respecting the dignity
107. of death and thus avoiding
unbearable and/or unnecessary
suffering or living in what one might
considered a handicapped and
hopeless condition. As stated by
Marc Augé,59 “To die without dignity
is to die alone, abandoned, in an
inhospitable and anonymous place, in
a non-place. To die without dignity
means to die, suffering needlessly or
to die tied up to a technical gadget
that becomes the sovereign of my
last days. To die without dignity also
means to die in isolation, surrounded
by insensitive people, soulless
specialists, and bureaucrats who
carry out their professional tasks
mechanically.”
108. Many authors22,24,30–34,60–62 criticize
using the interruption of ANH as a
way to hasten death because ANH
suspension inevitably leads to a
lengthy death with the potential for
suffering, and suffering would be
considered an unworthy way to die.
This reasoning suggests that ANH
should be continued in order to avoid
suffering by the patient, even when
that patient is unconscious.61,62
Others argue that ANH is a
standard part of treatment for
patients with DOC, and suggest that
the discontinuation of ANH along
with any other standard treatment
should be permitted when explicitly
requested and that this is in keeping
109. with the principles of beneficence
and non-maleficence and the
“patient’s best interests” rationale.63–65
However, the rights to freely live
(with obvious due respect for others)
and to make any decision concerning
one’s own personal health are well
established as respecting the
principles of free will and the
personal understanding of the quality
Innovations in CLINICAL NEUROSCIENCE [ V O L U M E 1
3 , N U M B E R 1 1 – 1 2 , N O V E M B E R – D E C E M B
E R 2 0 1 6 ]16
of life and human dignity.66 This
suggests that a human being has an
innate right to be valued and
respected and to receive ethical
treatment. In 1964, the Declaration