Downloaded 17 times

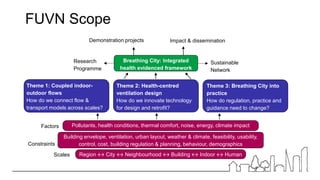
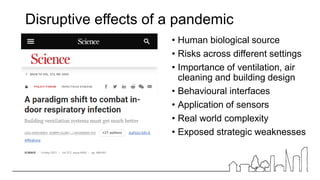
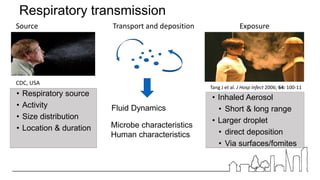
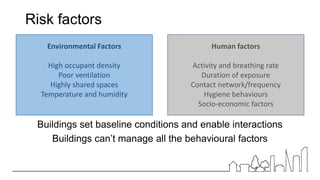







1) The document discusses enabling resilient indoor environments in light of the COVID-19 pandemic by learning from past outbreaks and focusing on improving indoor air quality and ventilation. 2) It recommends immediate actions like improved guidance for building owners on balancing infection control with other priorities like energy efficiency. It also recommends long-term strategies around standards, regulations, and research to embed infection resilience in building design, operation, and retrofits. 3) Real-world evidence shows ventilation is a key factor in reducing disease transmission indoors, but the relationship is complex depending on activities, space usage, and other environmental factors. More health-focused metrics and monitoring are needed.




























































