
Recommended
Recommended
More Related Content
Similar to ORIGINAL ARTICLE HIP - ANESTHESIAA randomized controlled.docx
Similar to ORIGINAL ARTICLE HIP - ANESTHESIAA randomized controlled.docx (20)
More from gerardkortney
More from gerardkortney (20)
Recently uploaded
Recently uploaded (20)
ORIGINAL ARTICLE HIP - ANESTHESIAA randomized controlled.docx
- 1. ORIGINAL ARTICLE � HIP - ANESTHESIA A randomized controlled trial of postoperative analgesia following total knee replacement: transdermal Fentanyl patches versus patient controlled analgesia (PCA) M. J. Hall1 • S. M. Dixon2 • M. Bracey3 • P. MacIntyre4 • R. J. Powell3 • A. D. Toms3 Received: 13 November 2014 / Accepted: 12 February 2015 / Published online: 11 March 2015 � Springer-Verlag France 2015 Abstract Background This randomized controlled trial compared a standard patient controlled analgesic (PCA) regime with a transdermal and oral Fentanyl regime for post-operative pain management in patients undergoing total knee replacement. Methods One hundred and ninety-six patients undergoing total knee replacement were recruited. Pre- and post-op-
- 2. eratively Visual Analogue Score (VAS), Oxford Knee Score, Health Anxiety and Depression Score and Brief Pain Inventory Score were completed. According to the day 1, VAS score patients were randomly allocated to either a PCA regime or a Fentanyl transdermal/oral regime. Patient reported outcomes were measured until the patients were discharged. Results The results demonstrate that in terms of analgesic effect, day of discharge and side effect profile the two regimes are comparable. Conclusions We conclude that a Fentanyl transdermal regime provides adequate analgesic effect comparable to a standard PCA regime in conjunction with a low side effect profile. Using a transdermal analgesic system provides ef- ficient continuous delivery enabling a smooth transition from hospital to home within the first week. Transdermal Fentanyl provides an alternative analgesic regime that can provide an equivalent analgesic effect so as to enable a
- 3. satisfactory outcome for the patient in terms of function and pain. Level of evidence II. Keywords Total knee replacement � Post-operative analgesia � Patient controlled analgesia � Fentanyl patches Introduction Knee replacement surgery has proved a successful and cost-effective method for relieving pain and restoring function in patients with osteoarthritis [1]. However, pain management after knee replacement surgery remains a significant problem, with patients reporting this as a major concern prior to surgery [2]. Implementing relevant pre- operative screening methods may facilitate the identifica- tion of individuals at high risk of experiencing high post- operative pain [3]. Despite recent advances in the aetiology of pain, improved pain treatments and the development of clinical guidelines for pain assessment, the under-treatment of post-operative pain remains a challenge to both surgeon
- 4. and anaesthetist. Recent studies have clearly demonstrated that patient satisfaction following total knee replacement is multifactorial with the most significant predictor of dis- satisfaction being a painful total knee replacement [1]. Providing effective pain relief in the post-operative pe- riod is essential to enable early mobilisation and reha- bilitation, minimise immobility-related complications, maximise functional outcome and reduce hospital stay. Many different methods of delivering adequate analgesia are currently employed but one of the most established is intravenous (IV) patient controlled analgesia (PCA). This provides the benefit of self-titrated IV opioid medication & M. J. Hall [email protected] 1 Yeovil District Hospital, Higher Kingston, Yeovil BA21 4AT, UK 2 Royal Cornwall Hospital, Truro, UK 3 Royal Devon & Exeter Hospital, Exeter, UK
- 5. 4 Nelson Bay District Hospital, Nelson, New Zealand 123 Eur J Orthop Surg Traumatol (2015) 25:1073–1079 DOI 10.1007/s00590-015-1621-6 http://crossmark.crossref.org/dialog/?doi=10.1007/s00590-015- 1621-6&domain=pdf http://crossmark.crossref.org/dialog/?doi=10.1007/s00590-015- 1621-6&domain=pdf enabling active participation in the patient’s own post-op- erative management compared to a more generic, orally delivered analgesia. The disadvantages are the cost of PCA pumps along with the monitoring required and nursing time to manage the systems appropriately. The literature provides no clear answers as to the best method of post-operative pain relief, with studies showing PCA [4] and regional techniques [5, 6] both providing good analgesia to enable rehabilitation. The major drawback of morphine can be the side effect profile, including nausea,
- 6. constipation and itching, whereas with regional analgesia the reliability and duration of action can be problematic. Fentanyl has formed the mainstay of intra-operative analgesia and has many beneficial features. In the lozenge form, it has a very rapid onset and can reach peak activity within 20 min compared to 40–60 min for oral morphine [7]. For this reason, the main clinical application of oral fentanyl lozenges is in the field of oncology for manage- ment of breakthrough pain. The aim of this randomized controlled study was to compare two analgesic regimes, PCA and Fentanyl (in a transdermal and oral form) and demonstrate that a trans- dermal Fentanyl patch can provide comparable post-op- erative analgesia to a standard PCA regime in terms of pain and side effect profile without compromising rehabilitation and discharge times. Post-operatively on day 1, we divided patients into a low and high pain group based on a pain score to see if this enabled an accurate prediction of pain
- 7. requirements during the subsequent post-operative period. Patients and methods All patients undergoing a unilateral total knee replacement at the Royal Devon and Exeter Hospital were invited to take part in the trial, which included all surgeons per- forming knee replacement surgery within the trust. Patients were excluded from the study if they were unable to walk twenty metres or climb three stairs for any reason other than pain in the affected joint, trauma and refusal or in- ability to give valid consent. Pre-operatively the study group completed the Oxford Knee Score (OKS) [17], Health Anxiety Depression Score (HADS) and Brief Pain Inventory Score (BPI). Participants in the trial were pre- scribed paracetamol (1 g QDS), an anti-inflammatory (Diclofenac 50 mg BD) and oral morphine (10–20 mg two hourly) as required. Patients were given a pain diary on day 1 and asked to score the pain on movement of the limb using a ten-point
- 8. Visual Analogue Score (VAS). If this score was 6/10 or more they were entered into the high pain group (HPG), and less than six entered the low pain group (LPG). An independent statistician using a sealed envelope technique carried out randomization of the HPG into the two treat- ment arms. The LPG remained on the routine analgesic regime. In the HPG, patients were randomized to either intravenous morphine administered through a PCA pump, or a Fentanyl patch with oral Fentanyl in the form of a lozenge that can be taken two hourly prior to exercise or for breakthrough pain. The doses of morphine in the PCA were 1 mg bolus with a 5 min lockout and no 4-h limit or background infusion. The doses of Fentanyl patch were 12.5 mcg for patients over 65 years and 25 mcg for pa- tients under 65 years with lozenges up to 400 mcg for breakthrough pain and up to five 200 mcg lozenges, whilst waiting for the patch to reach therapeutic plasma levels. The lozenges were titrated against signs of
- 9. lightheadedness. Each day until discharge, patients attempted standard physiotherapy tasks as part of their physiotherapy regime and then scored their pain using the VAS which is scored zero to ten (where the lower the score the less the patient’s pain). Patients were also asked to complete the BPI score with 1–4 being mild, 4–6 moderate and 7–10 severe pain. These scores were completed for worst pain, least pain, average pain, pain currently, pain on activity, pain effect on mood, pain on walking, pain whilst at work, pain affect on relations, pain whilst sleeping and pain effect on enjoy- ment. Pain assessment was carried out on a daily basis until discharge in the form of a short interview and completion of the above-mentioned scores. As part of the question- naires, we recorded the presence of side effects and their severity and impact on rehabilitation. For this study, full ethical approval was granted from the local ethics committee as well as full approval from the
- 10. Medicines and Healthcare Products Regulatory Agency (MHRA). Research and Development reference from Royal Devon and Exeter Hospital: 612163 and Research Ethics Committee reference: 06/Q2102/57. Statistical analysis Based on preliminary data for PCA that we can expect a 15 % reduction in pain worst score after 4 days (which is what we saw on average), and if there is truly no difference between the standard and experimental treatment, then 50 patients are required to be 80 % sure that the limits of a two-sided 90 % confidence interval will exclude a differ- ence between the standard and experimental group of more than 30 %. Continuous outcome data were tested for normality us- ing the Shapiro Wilks test. If the data were found to be normally distributed, central tendency was expressed using means and dispersion using standard deviation. If the data proved not to be Gaussian, and could not easily be trans-
- 11. formed, they were summarised using medians and 1074 Eur J Orthop Surg Traumatol (2015) 25:1073–1079 123 interquartile ranges and comparisons were made using nonparametric tests such as the Mann–Whitney U test. Confidence intervals were derived wherever possible. Categorical data were summarised as proportions and percentages as appropriate with associated confidence in- tervals. A comparison of time to discharge was analysed using Kaplan–Meier survival analysis. Repeated con- tinuous measures such as VAS pain, OKS, BPI elements and HADS were analysed using repeated measures analysis of variance provided the basic requirements were met. The first 5 days of data were included as in subsequent days, too many patients had been discharged to make analysis feasible. Results
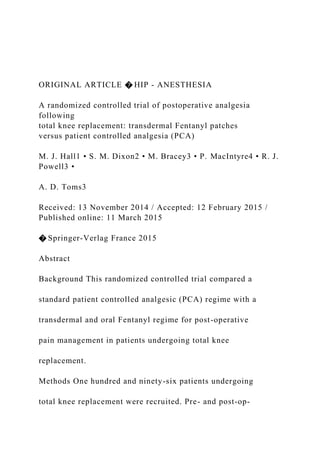
- 12. One hundred and ninety-six patients undergoing unilateral total knee replacement were recruited into the trial. Of these 64 subsequently withdrew from the trial after initially consenting and 25 had incomplete data collection for analysis and were excluded. This left a total of one hundred and seven patients in the trial with 69 in the LPG, 38 in the HPG with sixteen of these receiving Fentanyl patches and lozenges and 22 receiving a PCA infusion (Fig. 1). The mean age in the LPG was 68; Fentanyl group 64 and PCA group 66 years. Patient ages ranged from 41 to 96 years with patients in the LPG tending to be older on average, but this was not statistically significantly different. Day of discharge Kaplan–Meier survivorship analysis comparing the three groups showed a significant difference in day of discharge between the three groups. Mean time to discharge was 6.23 days for Fentanyl, 5.95 days for PCA and 4.48 days in the low pain group (p = 0.007) (Fig. 2).
- 13. We also analysed the percentage of patients discharged by day 5. The LPG had the highest rate of discharge overall, with forty-two (77.8 %) discharged by this time period. In the HPG, thirteen (68 %) of the PCA group and 7 (5 %) of the Fentanyl group were discharged by day 5; however, this difference was not significant (p = 0.284). Pain scores Pain scores were analysed at day 5 post-operatively as a large proportion of patients had been discharged after this time. Comparison of VAS scores showed that there was no significant difference in pain scores on movement (p = 0.317), rest (p = 0.811), worst pain (p = 0.353) and night (p = 0.730) between the Fentanyl and PCA groups (see Table 1). Both HPG groups (Fentanyl and PCA) showed a sig- nificant reduction, i.e. pain is better, in BPI Worst score, BPI Average score, BPI Now score, BPI Activity score,
- 14. BPI Mood score, BPI Walk score, BPI Relations score, BPI Work score, BPI Sleep score, BPI Enjoy score (see Table 2). The reduction in all BPI Worst scores was similar in both of the treatment groups (i.e. fentanyl from 6.81 to 4.22) and PCA from 7.44 to 4.48). BPI (Now) showed a significant difference between the LPG and HPG (p 0.001); however, all other modalities of the BPI score showed no significant difference. Side effects Using repeated measures ANOVA showed that the side effect scores between the Fentanyl and PCA groups were relatively low (1.271–1.417) and did not vary significantly across the 4 days. There was no significant difference in side effect score between the two groups, PCA (mean 1.368) and Fentanyl (mean 1.339) (p = 0.887). Oxford Knee Scores Both HPG groups (Fentanyl and PCA) demonstrated a significant reduction in OKS score (p 0.001). However, there was no significant difference between the two
- 15. treatment groups (p = 0.974) (see Table 3). The reduc- tion in OKS score was similar in both of the treatment groups, dropping from a mean of 36.9–28.72 in the Fentanyl group and 37.16–28.58 in the PCA group (see Table 3). Anxiety and depression: HADS scores Both HPG groups (Fentanyl and PCA) demonstrated a significant reduction in mean HADS score; 10.16–7.91 in the Fentanyl group and 12.89–7.06 in the PCA group (p = 0.004). Comparison of HADS Score for the LPG and HPG showed no significant difference (p = 0.615). Discussion The results from this study show that a post-operative regime of transdermal Fentanyl patches compares to that of a more conventional PCA regime in terms of analgesic effect, day of discharge and side effect profile. By using the VAS score pre-operatively, we showed that patients can be allocated into a high or low pain group and consequently a
- 16. Eur J Orthop Surg Traumatol (2015) 25:1073–1079 1075 123 targeted analgesic regime can be implemented to suit the individuals analgesic requirements. Over the last decade, the emphasis on peri-operative pain management in joint replacement surgery has made significant advances, to the extent that many consider it to be the most substantial advance in clinical practice [8]. A 4-year follow-up study concluded that pain is a common persistent problem in the community with a relatively high incidence and low recovery rate [9]. Ip et al. [10] in a systematic review found that preexisting pain, anxiety, age and type of surgery are the most significant factors for the intensity of post-operative pain with type of surgery, age and psychological distress, the three most important pre- dictive factors for analgesic consumption. It is well established that more than half the numbers of
- 17. patients undergoing lower limb joint replacement surgery Assessed for eligibility (n=196) Excluded (n=90) ♦ Not meeting inclusion criteria (n=26) ♦ Declined to participate (n=64) ♦ Other reasons (n=0) Analysed (n=14) at day 4 ♦ Excluded from analysis (n=0) Discontinued intervention (discharged home):- day 1, n=0 day 2, n=0 day 3, n=1 (1) day 4, n=1 (2) day 5, n=1 (3) day 6, n=6 (9) day 7, n=4 (10) (Cumulative totals in brackets) Allocated to Fentanyl intervention (n=15) ♦ Received allocated intervention (n=15) ♦ Did not receive allocated intervention (n=0) Discontinued intervention (discharged home):- day 1, n=0) day 2, n=0) day 3, n=1 (1) day 4, n=3 (4) day 5, n=7 (11)
- 18. day 6, n=10 (18) day 7, n=0 (18) (Cumulative totals in brackets) Allocated to PCA intervention (n=23) ♦ Received allocated intervention (n=23) ♦ Did not receive allocated intervention (n=0) Analysed (n=19) at day 4 ♦ Excluded from analysis (n=0) Allocation Analysis Follow-Up High pain group. Randomized (n=38) Enrollment Observational group (low pain) (n=68) Discontinued intervention (discharged home):- day 1, n=0 day 2, n=0 day 3, n=3 (3) day 4, n=20 (23) day 5, n=27 (50) day 6, n=5 (55)
- 19. day 7, n=4 (59) (Cumulative totals in brackets) Analysed (n=45) at day 4 ♦ Excluded from analysis (n=0) Fig. 1 Consort diagram of study patients 1076 Eur J Orthop Surg Traumatol (2015) 25:1073–1079 123 receive suboptimal analgesia especially during the initial post-operative period [8], with patients now well informed to their pain management and consider it a high priority [2]. However, the importance of delivering adequate analgesia reaches beyond that of clinical duty with recog- nition that inadequate pain management can increase the possibility of developing a poor outcome. Severe post-op- erative pain results in longer hospital stay, increased opioid use with resultant side effects and lower patient mood. Studies have demonstrated that those patients that receive suboptimal analgesia post-operative have higher levels of
- 20. arthrofibrosis and diminished range of motion [5, 11, 12]. In this study, analysis of pre-operative BPI pain score data demonstratedthattheHPG had a higherpercentage ofpatients reporting a BPI greater than 5, 61 %, compared to the LPG which only had 40 %. Early identification of patients likely to require additional or alternative methods of post-operative analgesia means maximising rehabilitation enabling achievement of physiotherapy targets sooner ultimately Fig. 2 Kaplan–Meier curve of discharge days Table 1 Mean VAS pain scores for pain on movement, at rest, worst and at night. A comparison of fentanyl and PCA interventions in the high pain group and also a comparison of the high pain group with the low pain group Intervention Mean VAS pain score Day Pain on movement Pain at rest Worst pain Pain at night High pain group Fentanyl 1 7.33 5.83 7.92 8.20 2 7.08 5.25 7.33 5.50 3 5.83 4.17 7.25 4.50
- 21. 4 5.42 3.50 6.25 4.00 5 5.33 3.50 6.67 3.30 PCA 1 7.67 6.58 8.00 7.71 2 7.67 4.58 8.50 4.43 3 6.75 4.33 7.33 5.00 4 6.08 4.17 7.25 3.86 5 5.50 3.50 6.92 2.71 Within subjects comparison (i.e. changes over time) F = 4.9 with 4, 88 df, p = 0.001 F = 5.83 with 4, 88 df, p = 0.001 F = 1.94 with 4, 88 df, p = 0.111 F = 17.83 with 4, 88 df, p = 0.001
- 22. Main effect: comparison of fentanyl versus PCA F = 1.05 with 1, 22 df, p = 0.317 F = 0.06 with 1, 22 df, p = 0.811 F = 0.90 with 1, 22 df, p = 0.353 F = 0.12 with 1, 22 df, p = 0.730 Low pain group 1 3.06 1.88 3.77 3.46 2 5.00 2.29 5.41 2.85 3 4.88 1.65 5.53 1.85 4 4.88 1.53 5.77 1.77 5 4.47 1.06 5.88 1.69 Within subjects comparison (i.e. changes over time)
- 23. F = 2.17 with 4, 156 df, p = 0.095 F = 6.01 with 4, 156 df, p = 0.001 F = 0.89 with 4, 156 df, p = 0.451 F = 19.97 with 4, 112 df, p 0.001 Main effect: comparison of LPG with HPG F = 17.87 with 1, 39 df, p 0.001 F = 29.39 with 1, 39 df, p 0.001 F = 19.87 with 1, 39 df, p 0.001 F = 14.54 with 1, 28 df, p = 0.001 Eur J Orthop Surg Traumatol (2015) 25:1073–1079 1077 123
- 24. reducing length of stay. In those patients identified as requir- ing additional analgesic support post-operatively the Fentanyl transdermal delivery regime has a distinct advantage of pro- viding a smooth transition to the home environment. The use of Fentanyl in orthopaedic surgery is limited with its most common usage being in management of breakthrough pain in the palliative care setting. Fentanyl patches do add to the total narcotic dosage as well as providing an alternative route for administration of anal- gesia. However, concerns over unpredictable delivery and the potential for adverse effects does deter many centres from using Fentanyl through this method. Using Fentanyl ionophoretic transdermal systems, Viscusi et al. [13, 14] demonstrated pain control equivalent to standard morphine PCA delivery systems in a variety of post-operative pa- tients, with no significant difference in side effect profiles. Analysis of the side effect profile in our study showed
- 25. similar findings with no significant difference demonstrated between the Fentanyl group and the PCA group. From this study, we suggest Fentanyl patches and lozenges provide a viable alternative to the standard morphine based regime used in most PCA pumps. Fentanyl in a transdermal therapeutic system provides several attractive features; firstly it provides stable plasma concentrations in a relatively short period of time which are maintained a background steady- state level, secondly newer formulations are safer and bioe- quivalent to standard oral preparations. Minville et al. re- ported on a small group of patients who had a fentanyl patch applied 10 h prior to total hip arthroplasty. No difference in respiratory depression was noted between that group and those who did not receive the patch [15, 16]. However, the use of fentanyl lozenges in this setting is innovative with the ability of the oral form of Fentanyl to be rapidly absorbed through the buccal mucosa providing high plasma levels rapidly means that its profile is ideally suited to managing
- 26. breakthrough pain during the post-operative period. Current trends favour the multimodal approach that provide adequate analgesia yet minimise opioid-related Table 2 Mean (and 95 % CI) BPI scores for worst pain and pain now Intervention BPI worst BPI now High pain group Fentanyl Pre 6.81 (5.74–7.89) 4.90 (3.46–6.34) Post 4.22 (3.15–5.3) 2.43 (1.30–3.56) PCA Pre 7.44 (6.56–8.33) 5.39 (4.2–6.57) Post 4.48 (3.59–5.37) 2.55 (1.62–3.48) Within subjects comparison (i.e. change over time) F = 6.74 with 1, 29 df; p = 0.015 F = 3.27 with 1, 29 df; p = 0.081 Main effect: comparison of fentanyl versus PCA F = 0.682 with 1, 29 df; p = 0.486 F = 0.21 with 1, 29 df; p = 0.653 Low pain group Pre 10.11 (8.35–11.87) 3.56 (2.87–4.25)
- 27. Post 6.07 (4.57–7.57) 1.24 (0.8–1.68 Within subjects comparison (i.e. change over time) F = 5.64 with 1, 80 df; p = 0.02 F = 5.38 with 1, 80 df; p = 0.023 Comparison of LPG with HPG F = 2.57 with 1, 80 df; p = 0.113 F = 15.51 with 1, 80 df; p 0.001 A comparison of fentanyl and PCA interventions in the high pain group and also a comparison of the high pain group with the low pain group. Age as a covariate Table 3 Mean (and 95 % CI) Oxford Knee Score and Hospital Anxiety and Depression Score Intervention Pre-OKS Post-OKS Pre-HADS Post-HADS High pain group Fentanyl 36.9 (32.61–41.19) 28.72 (25.56–31.89) 10.16 (6.38– 13.95) 7.91 (5.04–10.79) PCA 37.16 (33.92–40.41) 28.58 (26.19–30.97) 12.89 (9.77– 16.01) 7.06 (4.69–9.43) Within subjects comparison F = 43.96 with 1, 27 df; p 0.001 F = 9.93 with 1, 29 df; p = 0.004 Main effect: comparison of fentanyl versus PCA F = 0.001 with 1, 27 df; p = 0.974 F = 0.26 with 1, 29 df; p = 0.615 Low pain group 35.28 (33.34–39.54) 26.70 (25.03–28.37) 10.11 (8.35–11.87) 6.07 (4.57–7.57) Within subjects comparison F = 4.78 with 1, 78 df; p = 0.032 F
- 28. = 5.64 with 1, 79 df; p = 0.02 Comparison of LPG with HPG F = 2.57 with 1, 78 df; p = 0.113 F = 1.42 with 1, 79 df; p = 0.237 A comparison of fentanyl and PCA interventions in the high pain group and also a comparison of the high pain group with the low pain group. Age as a covariate 1078 Eur J Orthop Surg Traumatol (2015) 25:1073–1079 123 side effects. From this study, we suggest that the use of Fentanyl in a transdermal delivery system with oral Fen- tanyl for breakthrough pain provides equivalent pain re- lieve compared to the more standard opioid based PCA systems, which several studies have demonstrated provide adequate cost-efficient pain relief [2, 4]. However, none of the theoretical advantages were seen as a practical differ- ence in our patient group. Early identification of patients falling into the high pain category means that suitable analgesic regimes can be planned so as to create an envi-
- 29. ronment in which both mentally and physically the patient is able to undertake progressive rehabilitation. We know that patient expectations correlate highly with satisfaction and by managing expectations and considering the mental health of the patient can all help reduce the risk of overall dissatisfaction. Post-operative pain relief is one important aspect in the process of undergoing a knee re- placement with many global factors pertaining to that in- dividual playing an important role to the overall outcome. The benefits of splitting patients into low and high pain groups results means that those patients at risk of devel- oping severe acute post-operative pain are identified at an early stage and specific analgesic regime can be imple- mented so as to manage the pain appropriately in order that rehabilitation is not compromised. Central to successful enhanced recovery programs is providing a platform for patients to mobilise such that they can be discharged safely with a minimal length of stay. Multi-modal analgesic
- 30. regimes we feel are therefore a key component to these programs. Managing patients post-operative analgesia and pain perception efficiently can result in faster rehabilitation and ultimately improved functional outcome and patient satisfaction. This study demonstrates the potential benefits of multi-modal analgesia in enabling a faster rehabilitation in the initial post-operative period and ultimately improves outcomes. Conflict of interest None. References 1. Scott CEH, Howie CR, MacDonald D, Biant LC (2010) Pre- dicting dissatisfaction following total knee replacement. J Bone Joint Surg (Br) 92-B:1253–1258 2. Kastanias P, Gowans S, Tumber PS, Snaith K, Robinson S (2010) Patient-controlled oral analgesia for postoperative pain management following total knee replacement. Pain Res Manag J Can Pain Soc 15(1):11–16
- 31. 3. Werner MU, Mjobo HN, Nielson PR, Rudin A (2010) Prediction of postoperative pain. A systematic review of predictive ex- perimental pain studies. Anesthesiology 112:1494–1502 4. Hudova J, McNicol E, Quah C, Lau J, Carr DB (2006) Patient controlled opioid analgesia versus conventional analgesia for postoperative pain. Cochrane Database Syst Rev 4:48 5. Singelyn FJ, Deyaert M, Joris D et al (1998) Effects of intra- venous patient-controlled analgesia with morphine, continuous epidural analgesia and continuous three-in-one block on postop- erative pain and knee rehabilitation after unilateral total knee arthroplasty. Anesth Analg 87:88–92 6. Capdevila X, Barthelet Y, Biboulet P et al (1999) Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesi- ology 91:8–15 7. Collins SL, Faura CC, Moore RA, McQuay HJ (1998) Plasma concentrations after oral morphine: a systematic review. J Pain
- 32. Syndrome Manage 16:388–402 8. Maheshwari AV, Blum YC, Shekhar L, Ranawat A, Ranawat C (2009) Multimodal pain management after total hip and knee replacement at the Ranawat Orthopaedic Center. Clin Orthop Relat Res 467:1418–1423 9. Shipton EA, Tait B (2005) Flagging the pain: preventing the burden of chronic pain by identifying and treating risk factors in acute pain -. Eur J Anaesthesiol 22:405–412 10. Ip HYV, Abrishami A, Peng PWH et al (2003) Predictors of postoperative pain and analgesic consumption. A qualitative systematic review. Anesthesiology 111:657–677 11. Ranawat CS, Ranawat AS, Mehta A (2003) Total knee arthro- plasty rehabilitation protocol: what makes the difference? J Arthroplasty 18(3 Suppl 1):27–30 12. Lundbald H, Kreicbergs A, Jansson KA (2008) Prediction of persistent pain after total knee replacement for osteoarthritis. J Bone Joint Surg 90:166–171
- 33. 13. Viscusi ER, Siccardi M, Damaraju CV, Hewitt DJ, Kershaw P (2007) The safety and efficacy of fentanyl ionophoretic trans- dermal system compared with morphine intravenous patient- controlled analgesia for post-operative pain management: an analysis of pooled data from three randomized, active- controlled clinical studies. Pain Med 105(5):1428–1436 14. Viscusi ER, Reynolds L, Chung F, Atkinson LE, Khanna S (2004) Patient-controlled transdermal fentanyl hydrochloride vs intravenous morphine pump for postoperative pain. JAMA 291:1333–1341 15. Minville V, Lubrano V, Bounes V et al (2008) Postoperative analgesia after total hip arthroplasty: patient-controlled analgesia versus transdermal fentanyl patch. J Clin Anesth 20:280–283 16. Parvizi J, Miller A, Gandhi K (2011) Multimodal pain manage- ment after total joint arthroplasty. J Bone Joint Surg Am 93:1075–1084
- 34. 17. Dawson J, Fitzpatrick R, Murray D, Carr A (1998) Questionnaire on the perception of patients about total knee replacement. J Bone Joint Surg 80:63–69 Eur J Orthop Surg Traumatol (2015) 25:1073–1079 1079 123 Copyright of European Journal of Orthopaedic Surgery & Traumatology is the property of Springer Science & Business Media B.V. and its content may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express written permission. However, users may print, download, or email articles for individual use. A randomized controlled trial of postoperative analgesia following total knee replacement: transdermal Fentanyl patches versus patient controlled analgesia (PCA)AbstractBackgroundMethodsResultsConclusionsLevel of evidenceIntroductionPatients and methodsStatistical analysisResultsDay of dischargePain scoresSide effectsOxford Knee ScoresAnxiety and depression: HADS scoresDiscussionConflict of interestReferences