FINANCIAL MANAGEMENT (PART 4)
INTRODUCTION OF
CAPITAL BUDGETING PART- 1
1. INTRODUCTION
Dear students, welcome to the lecture series on capital budgeting. Today in this
lecture, we shall learn about meaning, nature and importance of capital
budgeting, what is the process involved in capital budgeting and the types of
capital budgeting decisions. The objective of this lecture is to understand the
conceptual frame work of capital budgeting, the meaning and significance of
capital budgeting, the mechanism of capital budgeting process from identification
of investment opportunities till its implementation and review and we shall also
learn various type of capital budgeting decisions.
2. TYPES OF EXPENDITURE
We will learn certain basic concepts before understanding the concept of capital
budgeting. What is investment? Investment is the expenditure in the expectation
of some benefit; hence expenditure can be of two types, revenue expenditures
and capital expenditures.
Revenue expenditures are those expenditures which are charged to profit and loss
account. They are incurred for the following reasons, first to trade of business that
is for running the business, such expenses are selling and distribution expenses,
administrative expenses and finance expenses.
Secondly, they are incurred for maintaining the earning capacity of fixed assets,
example, repairs of machinery, second type of expenditure is capital expenditure.
They are the expenditure which are incurred for acquisition of fixed assets and for
improving their earning capacity. They are not charged to profit and loss account
but they are shown as fixed assets in the balance sheet, example, plant and
machinery building.
3. MEANING OF CAPITAL BUDGET AND CAPITAL BUDGETING
What is capital budget? It’s a list of expenditure which we need to incur. Under
capital plans,
we allocate the expenditure towards the various fixed assets. What is the meaning
of capital budgeting? It is the process of planning the acquisition of long term
assets.
Let us learn the definition in detail what is capital budgeting. Capital budgeting
decisions are related to allocation of resources to different long term assets, it
denotes a decision situation where lump sum funds
are allocated to the long term assets from which arises the benefit over a period
of year, that is if I incur an expenditure today, I will earn the benefits in the
coming years, that is in near future, year 1,2,3, I will reaps benefits. Now the
capital budgeting decision involves entire process of decision making relating to
acquisition of an asset from which returns are received over longer period,
examples are to buy machinery, if I buy machinery today, I will reap its benefit in
a longer period because I will use it in production and my production will continue
year after year. Second to undertake a research and development program, thir.
FINANCIAL MANAGEMENT (PART 4) INTRODUCTION OF CAPITAL .docx
1. FINANCIAL MANAGEMENT (PART 4)
INTRODUCTION OF
CAPITAL BUDGETING PART- 1
1. INTRODUCTION
Dear students, welcome to the lecture series on capital
budgeting. Today in this
lecture, we shall learn about meaning, nature and importance of
capital
budgeting, what is the process involved in capital budgeting and
the types of
capital budgeting decisions. The objective of this lecture is to
understand the
conceptual frame work of capital budgeting, the meaning and
significance of
capital budgeting, the mechanism of capital budgeting process
from identification
of investment opportunities till its implementation and review
and we shall also
learn various type of capital budgeting decisions.
2. 2. TYPES OF EXPENDITURE
We will learn certain basic concepts before understanding the
concept of capital
budgeting. What is investment? Investment is the expenditure in
the expectation
of some benefit; hence expenditure can be of two types, revenue
expenditures
and capital expenditures.
Revenue expenditures are those expenditures which are charged
to profit and loss
account. They are incurred for the following reasons, first to
trade of business that
is for running the business, such expenses are selling and
distribution expenses,
administrative expenses and finance expenses.
Secondly, they are incurred for maintaining the earning capacity
of fixed assets,
example, repairs of machinery, second type of expenditure is
capital expenditure.
3. They are the expenditure which are incurred for acquisition of
fixed assets and for
improving their earning capacity. They are not charged to profit
and loss account
but they are shown as fixed assets in the balance sheet,
example, plant and
machinery building.
3. MEANING OF CAPITAL BUDGET AND CAPITAL
BUDGETING
What is capital budget? It’s a list of expenditure which we need
to incur. Under
capital plans,
we allocate the expenditure towards the various fixed assets.
What is the meaning
of capital budgeting? It is the process of planning the
acquisition of long term
assets.
Let us learn the definition in detail what is capital budgeting.
4. Capital budgeting
decisions are related to allocation of resources to different long
term assets, it
denotes a decision situation where lump sum funds
are allocated to the long term assets from which arises the
benefit over a period
of year, that is if I incur an expenditure today, I will earn the
benefits in the
coming years, that is in near future, year 1,2,3, I will reaps
benefits. Now the
capital budgeting decision involves entire process of decision
making relating to
acquisition of an asset from which returns are received over
longer period,
examples are to buy machinery, if I buy machinery today, I will
reap its benefit in
a longer period because I will use it in production and my
production will continue
year after year. Second to undertake a research and development
program, third
example is diversification of a product line, it means if a
5. company is into the
textile industry,
it can diversify its product line by going into retail business or
to launch a
promotional campaign. These are the examples of capital
budgeting projects.
4. IMPORTANCE OF CAPITAL BUDGETING
What is the importance of capital budgeting? There are
basically five factors which
are important in any capital budgeting decision, they are cost,
time, risk,
irreversible decisions and complexities.
What is cost? Cost means the initial cost of a project, we need
to incur initial cost
on project, initial cost here means cost of acquisition of some
asset and if its
expansion project,
6. we may need some additional working capital, so that cost shall
be added to the
cost of asset or project and if it’s a case of replacement, cost of
replacement of
asset shall be the cost of the project and if I am able to receive
certain salvage
value, by selling that asset, that cost shall be reduced by that
amount of salvage.
We will learn about second thing, that is time element, the
effect of decision is
known only in the near future and not immediately because my
cash out flows are
in the current period while my returns are coming in near future
that is
subsequent years its coming, it’s an irreversible decision, why
it’s an irreversible
decision because once I have employed my funds into the
acquisition of a fixed
asset, I cannot revert back. The funds will be block into that
asset for a longer
period of time, even if I want to come out of that project, I
won’t be able to come
out without losses, example if I invest my money in plant and
7. machinery and if I
am going to market for selling it immediately, I won’t be able to
fetch a same
amount of money as I have purchased, so differential amount
shall be a loss and
that can be substantial. Next comes complexity, decision based
are on forecasting,
forecasting of future events and in flows. How shall I quantify
my inflows, they
shall be quantified on the basis of certain statistical and
probabilistic techniques,
hence I need to be very careful while applying my mind to trace
out the inflows
and projected outflows. Fifth comes risk, the longer the period,
the greater the
risk, uncertainties associated with cash flows are higher as the
period is higher,
hence decision should be taken after a careful review of all the
available
information, with this we have concluded importance and
meaning of capital
8. budgeting.
5. FACTORS AFFECTING CAPITAL BUDGETING
DECISIONS
We shall learn about the factors affecting capital budgeting
decisions. First is net
investment outlet,
it means again the initial cost that is what cost I need to incur.
It shall be the sum
of cost of new asset purchased plus investment in working
capital, less salvage
value of old asset if any,
For example,
our cost of new machinery is 90,000 and I need additional
working capital of
10,000, so we will reach the cost initial cost as 1,00,000 rupees.
If it is a
9. replacement decision,
our cost of replacing the asset shall be initial cost, for example
it is 65,000 rupees
and we can get salvage value of 5,000 rupees by selling that old
asset.
So salvage value shall be deducted from cost of replacing the
old asset, the cost
comes out to be rupees 60,000 and it will amount to net
investment outlay for the
project. Second factor is net cash inflow or benefit, it means
cash flow after tax
and we need to add back depreciation and other amortization.
Why we need to add up depreciations because depreciation is a
non cash item, we
do not need to spend money on such item of financial expenses.
It is a totally non
cash expenses, how shall we compute cash flows after tax? We
will take up the
figure of earnings before interest and tax;
10. reduce the financial charge, that is interest, what we are getting
is earning before
tax, now reduce it from the taxes, what is left out is earnings
after tax, they are
called cash flows after tax. We shall add up depreciation again
in this figure so
arrived, so we will get cash flows, this way, we shall compute
our net cash
inflows. Third factor is project life;
project life means the time period during which a project can
give us positive
cash flows after tax, it is different from physical life of an
asset. It is more an
economic life rather than physical life provided by the supplier.
For example, if an
asset is able to generate cash flows after tax for 5 years of its
life, the project life
shall be 5 years. Next comes is desirable minimum rate of
return, it is also called
as cut off rate or average cost of capital. A project should earn
at least returns
equal to cost of capital, so it’s a selection criterion for
11. accepting or rejecting a
project. If my return from projects comes, greater than cost of
capital, we shall
accept that project. So this is the rate which we need to earn
from a project, it
shall be computed as weighted average cost of capital, there are
prescribed
formula’s for computing weighted average cost of capital.
Moreover it covers the
risk associated with the project as it takes into account interest
element. Last
comes opportunity cost, opportunity cost means cost of forgoing
one alternative to
accept the other. With this, we have completed the factors
affecting capital
budgeting decisions.
6. CAPITAL BUDGETING PROCESS
Students, now we will learn about capital budgeting process.
Process as the names
suggest, it involves lot many steps so we will learn this step by
step.
12. First comes identification of investment opportunity, second
assembling of the
proposed investment, third shall be screening of the project,
fourth economic
evaluation of the proposal, fifth decision making, sixth
preparation of capital
budget, seventh authorization of capital expenditure, eight its
implementation and
ninth and final is performance review. What is identification of
potential
investment opportunity? The first step in capital budgeting
process is identifying of
investment proposal, such identification can be started at any
level of
management.
For example,
suggestions for improvement in the production process can be
13. given by a foreman.
So the generation of investment proposal can be made either by
the grass root
level of people or up to top management. Second comes,
assembling of the
proposal, when the origin of investment proposal has taken
place, then
presentation of the proposal shall take place, the proposal needs
to be presented
in a prescribed format. It shall include date of project, project
identification
number, purpose of the project, estimated total cost of the
project, estimated
start and end time of the project, estimated period by which
earnings shall be
started in the project and estimated cost savings and reduction
in cost. This way,
a proposal shall be presented to the planning committee.
Once the proposal is presented in the prescribed format, the
screening of that
proposal shall be done by budget committee or planning
14. committee. They shall
find out whether this proposal is as per the standard set by the
committee or top
management.
They shall look into the project to find out whether it is line
with the long term
development program of the company or not. If they found
suitable, then further
economic evaluation of these proposal shall be done else it shall
be rejected. Now
the budget committee or planning committee shall do the
economic evaluation of
the proposals that has been screened. Under economic
evaluation, they shall find
out cost benefit analysis
that is they will trade off between the cost and benefits
occurring from that
project. Cost shall be the initial cost and benefits will be the
cash flows which we
are generating over the years, this trade off can be done using
15. capital budgeting
techniques which we will learn later on. These techniques can
be net present
value techniques, payback period techniques, accounting rate of
return techniques
and so on. After it has been evaluated economically, next step is
decision making.
If the project is profitable, that is the benefits exceeds cost, we
will accept that
proposal and send it to the board of directors with the
recommendation. If board
of directors find it appropriate as per all the standards and
norms, they will
allocate their funds to the finance manager for planning the
capital budgets.
Hence capital budgets are plan of expenditure which needs to be
undertaken for
various capital budgeting proposals. Once capital budgets are
chalked out, then
authorization of expenditure shall be given to the respective
heads. After getting
authorization for capital expenditure, the project shall be
executed and
16. expenditure will be incurred on that very project. Once a project
is executed, we
shall find out if any deviation is there between the standards so
set and actual
expenditure incurred, so now from stage of execution,
we are coming to the stage of control, we will find out
deviations. Reasons of
deviations, for this, there shall be certain reports generated
which are called capital expenditure report, inspection reports,
audit reports, we
shall be furnish to top management so that these deviations
either can be traced
out, two possibilities are there, either we will revise the cost
budgets or we shall
control the cost, hence we have completed this capital
budgeting process.
7. TYPES OF CAPITAL BUDGETING DECISIONS
17. Students, having understood the process of capital budgeting,
we shall learn about
types of capital budgeting decisions. Capital budgeting
decisions can be based on
firm’s existence or on nature of decision.
What are the capital budgeting decisions which are based on
firm’s existence?
They can be either for cost reduction or for revenue expansion.
Cost reduction
decisions shall focused on reduction of operating cost and
improving efficiency
while revenue expansion decisions will focus on increasing sale,
new products,
product version etc. under cost reduction decisions, two types of
decisions are
there, replacement decisions or modernization decision. Under
revenue expansion
18. decisions, again two sorts of decisions are there, first
expansion, another is
diversification decision. What is replacement decision?
Replacement decision means to replace the existing asset with a
new and
improved one, example; version of the equipment has changed.
It mostly happens in the case of technology, computers. Second
is modernization,
install new machinery in the place of old one which has become
technological
outdated, for example, in a Handloom, earlier, certain manual
machine was used,
now that will be replace by totally new machine with advanced
technologies.
This is called modernization.
Now we will learn about revenue expansion decisions. First one
19. is expansion,
expansion means to add capacity to existing product line, to
meet increase
demands, to improve production facilities and to increase
market share of existing
products. Second is diversification, diversification means to
going into new
business or to a new product line, for example,
X company was dealing in a textile industry, now it wants to put
its hand into the
retail industry, so that is called diversification. Earlier a
company was producing
garments, now it wants to produce Pharmaceuticals, so this way
product has been
expanded or industry such has been expanded, this is called
diversification. Now
there are certain decisions which are based on nature of
decisions and they are
very crucial while solving the problems of capital budgeting.
20. They are mutually exclusive decisions; accept reject decisions
or capital rationing.
What is a mutually exclusive decision? Acceptance of one
alternative will result in
rejection of another alternative, for example, if I accept
machine A, the rejection
of machine B is automatically done,
accept reject decisions are those decisions where projects are
independent, that
means they do not compete with each other for the selection
criteria. If they are
profitable, they will be accepted, if they are not profitable, they
won’t be
accepted. Provided company has funds available for accepting
those projects. Now
comes capital rationing, capital rationing decisions are those
21. decisions where
funds are not adequate while proposals are too many, means
proposal A can also
be accepted, B can also be accepted and C can also be accepted
but I don’t have
so much of fund that I can cover all the three proposals, so I
will do the rationing,
the most profitable project will be given preference afterwards
less profitable and
then the least profitable. This way, we have concluded the type
of capital
budgeting decisions.
Global Health
Research and Policy
Min et al. Global Health Research and Policy (2016) 1:14
DOI 10.1186/s41256-016-0014-7
RESEARCH Open Access
The global spread of Middle East
respiratory syndrome: an analysis fusing
traditional epidemiological tracing and
molecular phylodynamics
22. Jae Min1* , Eleonora Cella2,3,4, Massimo Ciccozzi2,5,
Antonello Pelosi2, Marco Salemi4 and Mattia Prosperi1*
Abstract
Background: Since its discovery in 2012, over 1700 confirmed
cases of Middle East Respiratory Syndrome (MERS)
have been documented worldwide and more than a third of those
cases have died. While the greatest number of
cases has occurred in Saudi Arabia, the recent export of MERS-
coronavirus (MERS-CoV) to Republic of Korea showed
that a pandemic is a possibility that cannot be ignored. Due to
the deficit of knowledge in transmission
methodology, targeted treatment and possible vaccines,
understanding this virus should be a priority. Our aim was
to combine epidemiological data from literature with genetic
information from viruses sequenced around the
world to present a phylodynamic picture of MERS spread
molecular level to global scale.
Methods: We performed a qualitative meta-analysis of all
laboratory confirmed cases worldwide to date based on
literature, with emphasis on international transmission and
healthcare associated infections. In parallel, we used
publicly available MERS-CoV genomes from GenBank to create
a phylogeographic tree, detailing geospatial timeline
of viral evolution.
Results: Several healthcare associated outbreaks starting with
the retrospectively identified hospital outbreak in
Jordan to the most recent outbreak in Riyadh, Saudi Arabia have
occurred. MERS has also crossed many oceans,
entering multiple nations in eight waves between 2012 and
2015. In this paper, the spatiotemporal history of MERS
cases, as documented epidemiologically, was examined by
Bayesian phylogenetic analysis. Distribution of
24. the data made available in this article, unless otherwise stated.
http://crossmark.crossref.org/dialog/?doi=10.1186/s41256-016-
0014-7&domain=pdf
http://orcid.org/0000-0003-4112-9583
mailto:[email protected]
mailto:[email protected]
http://creativecommons.org/licenses/by/4.0/
http://creativecommons.org/publicdomain/zero/1.0/
Min et al. Global Health Research and Policy (2016) 1:14 Page
2 of 14
Background
After the identification of a novel coronavirus (CoV) in
2012, later named Middle East Respiratory Syndrome
(MERS)-CoV, there has been a rise in cases reported
worldwide. As of June 23, 2016, the World Health
Organization (WHO) reported 1768 confirmed cases and
630 deaths, yielding case fatality of 35.6% [1]. Cases have
been reported from 27 countries, spanning European,
Asian, North American and African continents (Fig. 1).
Majority of the cases occur in the MERS endemic region
of Middle East, but the recent export of the virus to Korea
showed that MERS-CoV can spread rapidly if unchecked
by early detection and infection control measures [2]. The
number of cases has climbed since its initial discovery,
with just 9 cases identified in 2012, 168 in 2013, 768 in
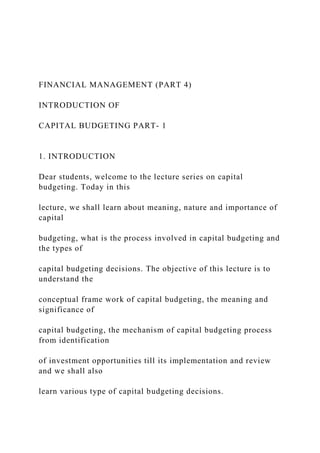
2014, 683 in 2015 and 140 so far in 2016 (Fig. 2).
MERS-CoV
MERS-CoV is the second coronavirus after Severe Acute
Respiratory Syndrome (SARS)-CoV with the potential to
cause a pandemic [3]. Characterized by its ‘corona’ or
crown shape, it is a single-stranded RNA virus with ap-
proximately 30,000 nucleotides in its genome.
25. While current literature mostly concur that camels are
important zoonotic reservoirs for MERS-CoV, there has
been some evidence that bats might be primary viral
reservoirs and that MERS-CoV will jump to a different host
such as dromedary camels, and subsequently humans, when
opportunities arise; similar transmission dynamic has been
observed with SARS-CoV where palm civets acted as inter-
mediary host between bats and humans [4, 5]. However
coronaviruses isolated from bats are more genetically distant
from human MERS-CoV than those isolated from camels,
which have shown very high similarities to humans’ [6].
Virus transmission from camels is thought to be con-
nected to consuming camel milk or urine, working with
Fig. 1 Map of MERS cases reported worldwide as of June 2016
according t
color indicates countries that reported less than or equal to 5
cases, includ
Germany, Greece, Italy, Kuwait, Lebanon, Malaysia,
Netherlands, Philippines,
color shows countries with greater than 5 but less than 100
cases (Iran, Jor
countries have had more than 101 cases (Saudi Arabia and
Korea)
camels and/or handling camel products [7]. Secondary
transmissions are largely associated with hospitals or close
contacts of MERS cases. As shown with the family cluster
in the United Kingdom (UK), relatives or people living in
close contact with an infected patient are susceptible to
the pathogen even outside of hospital settings [8].
While the exact methods of MERS-CoV transmissions
are unknown respiratory droplet and aerosol transmissions
are cited as most probable, but there is no conclusive
evidence on how close a person has to be for exposure and
26. what protection is most suitable [3, 9]. For example, the
Korean Ministry of Health and Welfare (KMoH) classified
close contacts as those who were within 2 meters of MERS-
CoV infected patient or in contact with respiratory droplets
without personal protective equipment, yet the extent to
which of those close contacts were infected is unknown
[10]. It has been hypothesized that camels can transmit a
higher dose of viruses to humans while the quantity is lower
between humans, and that MERS-CoV has not fully
adapted for human-to-human transmission [11, 12]. Food,
oral-fecal, and fomite transmissions are also possible trans-
mission routes since the virus has been detected in camel
milk, patient fecal sample and hospital surfaces [13–16].
Middle East Respiratory Syndrome
Patients with MERS have a wide range of symptoms from
being completely asymptomatic to suffering from severe
respiratory illnesses. Fever cough, chills and myalgia are
some of the most commonly reported symptoms in mild
cases, but respiratory distress, kidney failure and septic
shock have been reported in acute cases [17, 18]. There
are neither vaccines nor specific medications against
MERS-CoV, so treatments are usually palliative in nature
[17, 19]. More than a third of those infected with MERS-
CoV die [1]. For comparative perspective, case fatality was
one in ten for the SARS pandemic of 2003 [20].
o WHO [1]. Countries in grey have had no cases of MERS.
Light pink
ing imported cases (Algeria, Austria, Bahrain, China, Egypt,
France,
Thailand, Tunisia, Turkey, UK, United States, and Yemen),
medium pink
dan, Oman, Qatar, and United Arab Emirates), and red colored
27. Fig. 2 Summary of MERS cases from March 2012 to May 2016.
Incidences summarized by month and by 4 regions of the globe
where infected
patients have been found: Middle East, Europe/North America,
Africa, and Asia. Orange line indicates cumulative number of
cases
Min et al. Global Health Research and Policy (2016) 1:14 Page
3 of 14
Research is yet to be done on the relationship between
symptoms and transmissibility. Given that clinical proce-
dures for acute patients can generate aerosolized viral
particles, patients with severe respiratory distress would be
more likely to transmit the virus compared to asymptomatic
patients, but transmissibility of airborne MERS-CoV is un-
known [12]. In addition, research in transmission is essential
with regards to ‘superspreaders’ who are sources for large
number of cases for healthcare associated outbreaks [21].
Possibility of global outbreak
The uncertainty of pathogen transmission, lack of vaccine
against MERS-CoV and deficit in MERS specific treat-
ments make public health interventions challenging to
design [22]. With ease of international travel, the possibility
of MERS spread is present in all nations. Notably, countries
without MERS endemic are unfamiliar with the infectious
agent that may be imported by travelers and are, therefore,
particularly vulnerable.
In this paper we reviewed epidemiological contact
tracing information from public health agencies and
peer-reviewed literature, in order to see geographic and
temporal distribution of MERS cases around the globe.
Concurrently, we used genetic sequences to infer trans-
mission dynamics and inter-host evolution of MERS-
CoV. The combined analysis was used to present a phy-
28. lodynamic picture, detailing international, zoonotic and
healthcare associated transmissions at genetic and
population levels. These analyses can be used to under-
stand pathogen spread and to implement public health
measures to curb a pandemic [23].
Methods
Literature review
Detailed review of current literature was conducted using
the five-step model of Khan et al. [24]. The literature
searches on PubMed used following keywords: “Middle
East Respiratory Syndrome”, “MERS” and “MERS CoV”.
The article’s potential relevance to our topic was examined
initially by article title then by abstract content. Included
papers were case reports and articles on phylogenetics,
healthcare related outbreaks and epidemiology, and we ex-
cluded papers on viral structure and model organism re-
search. Relevant publications from national and
international public health agencies were reviewed as well.
WHO’s Disease Outbreak News and MERS risk assess-
ments spanning September 2012 to June 2016 were used
as primary sources to create a map of global transmissions
[1]. The data were supplemented with the European
Centre for Disease Prevention and Control (ECDC)’s
Communicable Disease Threats Reports and Korean Cen-
ter for Disease Control and Prevention (KCDC) and
KMoH reports published online [25, 26]. Number of cases
in hospital settings and non-hospital settings were com-
pared using Mann-Whitney U test in SAS software v9.4
for Windows [27]. Following the literature review, forest
plots of basic reproduction numbers were created using
DistillerSR Forest Plot Generator [28].
MERS-CoV genetic sequences
MERS-CoV sequences isolated from humans and camels
were downloaded from the GenBank repository and are
29. listed in Additional file 1 [29]. Combined Open Reading
Frames 1a and 1b (ORF1a/b) region was chosen specific-
ally for the high number of sequences available and low
phylogenetic noise in order to create the most inform-
ative phylodynamic analyses. Duplicate sequences from
single patients were excluded to explore inter-host dy-
namics without intra-host evolution, and only sequences
with known date and place (city, state or country) of col-
lection were included. Based on the metadata associated
with the GenBank accession, we created three datasets:
first with all CoV sequences isolated from both humans
and camels, second dataset with solely sequences from
humans, and third only with sequence from camels.
The sequences were aligned using Clustal X and manu-
ally edited using BioEdit [30, 31]. Then the best fitting nu-
cleotide substitution model was chosen via hierarchical
likelihood ratio test with ModelTest implemented in
PAUP*4.0 [32, 33].
Min et al. Global Health Research and Policy (2016) 1:14 Page
4 of 14
Preliminary analysis
Three preliminary analyses were performed prior to
Bayesian analysis: recombination, phylogenetic signal and
temporal signal tests. First, identification of recombinant
strains was done using Bootscan/Recscan method in
RDP4 with default window size and parameters [34, 35].
Second phylogenetic signals in the datasets were inves-
tigated with TREE-PUZZLE [36]. It reported maximum
likelihood for each new tree generated as a single dot on
a triangle. The distribution of these dots among the
seven zones of the triangle indicated their phylogenetic
30. signals: if a dot was located in the central triangle, its
tree had unresolved phylogeny with star-like structure. If
a dot was located in the sides of the triangle, the phyl-
ogeny was network like and only partially resolved.
Lastly, if the dot was positioned in one of the three cor-
ners, the tree topology was considered fully resolved
[37].
Third, amount of evolutionary change over time, or
temporal signal, from the sequences was examined using
TempEst [38]. The three datasets were analyzed separately
using default parameters.
Coalescent model for demographic history
In order to conduct Bayesian phylogenetic analyses on
MERS-CoV evolution three parameters for demographic
growth model were tested: (1) molecular clock, (2) prior
probability distribution and (3) marginal likelihood esti-
mator. First, molecular clock was calibrated using dates
of sample collection with the Bayesian Markov Chain
Monte Carlo (MCMC) method in BEAST v1.8 [39]. Both
strict and relaxed molecular clocks were tested, but re-
laxed clock with underlying lognormal distribution was
superior. For the investigation of demographic growth of
MERS-CoV ORF1a/b, four independent MCMC runs
were carried out each with one of the following coales-
cent prior probability distributions: constant population
size, exponential growth, Bayesian Gaussian Markov
Random Field (GMRF) skyride plot and Bayesian skyline
plot [40–42]. Both parameters listed above were tested
with path sampling and stepping stone marginal likeli-
hood estimators [43, 44].
Best fitting model was chosen by comparing the Bayes
Factors [45]. If log (Bayes Factor) was >1 and <3, there
was weak evidence against the model with lower mar-
31. ginal likelihood [43]. Higher log values indicated stron-
ger evidence, such that values greater than 3 and 5 were
considered to give strong and very strong evidence,
respectively.
For all three datasets, the MCMC sampler was run for
at least 50 million generations, sampling every 5000 gen-
erations. Only parameter estimates with effective sample
size (ESS) greater than 250 were accepted to ensure
proper mixing of the MCMC.
Phylogeographic analyses
Phylogeographic analyses were conducted also using
Bayesian-MCMC method in BEAST using (1) best fitting
nucleotide substitution model chosen by ModelTest, (2)
relaxed molecular clock with underlying lognormal rate
distribution, (3) GMRF skyride plot as demographic
model and (4) evolutionary rate previously estimated
with sample collection dates. For all three datasets, the
MCMC chains were run for at least 100 million genera-
tions and sampled every 10,000 steps. Using the stand-
ard continuous time Markov chain over discrete
sampling locations (31 cities and countries) and Bayesian
Stochastic Search Variable Selection procedures to infer
social network, phylogeographic analyses were carried
out for total and human datasets [46]. For the camel
subset, continuous geographical trait analysis was used
since spatial distribution of the MERS-CoV from camels
was presumed not to be independent of their genetic
phylogeny [47].
Maximum clade credibility trees which had the largest
product of posterior clade probabilities, were selected
after 10% burn-in using Tree Annotator, part of the
BEAST package [39]. Calculations of posterior probabil-
ity were used to establish statistical support for mono-
phyletic clades.
32. Results
Phylodynamic analysis
We retrieved 196 MERS-CoV sequences from GenBank
88 from camels and 108 from humans, to analyze
molecular evolution of the coronavirus over time
(Additional file 1). All available ORF1a/b sequences as of
March 16, 2016 were included and their dates ranged
from April 2012 to the latest deposited sequences of
June 2015. These sequences were from: China, Egypt,
France, Germany, Oman, Qatar, Saudi Arabia, Korea,
Thailand, UAE, UK and US [48]. Main dataset with all
sequences, subset with only sequences from humans,
and third subset with sequences from camels were
created.
Sequences were aligned with Clustal X and four were
removed due to poor alignment (GenBank accession
numbers: KJ361499 KJ156916, KJ156941 and KJ156942).
Due to possibilities of recombinant MERS-CoV
strains, aligned sequences were tested for recombination
via RDP4 [49–51]. Sequences 441SA15 and 451SA15
had similarities to two different strains, 470SA15 and
355SA13 and were removed from the dataset since re-
combinant strains could convolute the evolutionary ana-
lysis (results shown in Additional file 2: Figure S1).
Then the phylogenetic content of ORF1a/b region was
investigated by likelihood mapping method to ensure
that there were enough signals to compute phylogenies
[36]. The percentage of dots, or noise level, falling in the
Min et al. Global Health Research and Policy (2016) 1:14 Page
33. 5 of 14
central triangle was 1.4% for all sequences, 2.3% for hu-
man sequences only, and 3.2% for camel sequences only
(Additional file 2: Figure S2a, b and c respectively). For
all three datasets, the three corners of the triangles
summed to be greater than 95% and the central triangles
had less than 30% noise, so we expected fully resolved,
tree-like phylogenies [37].
Temporal signal of the sequences was also investi-
gated. Temporal signal refers to how much genetic
change has taken place between sampling times which is
especially important in this case since samples were col-
lected over time [38]. In order to make molecular clock
inferences, genetic distances on phylogenetic trees have
to be translated into temporal distances. Root-to-tip di-
vergence plots are shown in Additional file 2: Figure
S3a, b and c; no major deviations from the regression
line were observed indicating that the genetic divergence
of the sequence more or less align with what is expected
given the sequence sampling date. The regression plots
for the main dataset and the human subset had R2
values of 0.75 and 0.63, respectively, indicating a strong
association while the camel subset had R2 of 0.42 which
was weaker but still positive.
Finally the datasets were analyzed for their evolution-
ary history over time and space using BEAST. The
Tamura-Nei 93 (TN93) evolutionary model with gamma
distribution G = 0.05 was chosen by ModelTest as best
fit. The GMRF skyride plot with stepping stone marginal
likelihood estimator was selected as the best demo-
graphic model by BEAST. Phylogeographic trees of the
main dataset is shown in Fig. 3 and the camel set is
shown in Fig. 4 (main dataset colored according to
34. countries is available as Additional file 2: Figure S4 and
human set trees are included as Additional file 2: Figures
S5 and S6).
Overview of outbreaks and exports
Over 1300 MERS cases, or almost 80% of global inci-
dence, have been reported from Saudi Arabia [1]. Korea
has the second highest number of cases (n = 185) and
United Arab Emirates (UAE) with 83 cases is third [1].
In the past three years since discovery of MERS-CoV,
eight major healthcare associated outbreaks have been
reported worldwide; the ninth wave recently occurring
in multiple cities of Saudi Arabia. Those described here
are based on cases with documented nosocomial trans-
mission and are indicated by blue colored clusters in
Fig. 5. Cases of MERS patients traveling internationally
are indicated by arrows representing the direction of
their travel and probable zoonotic transmission cases are
marked by brown camels in the same figure.
The first hospital related outbreak was in Zarqa,
Jordan where 2 cases were confirmed for MERS-CoV
and 11 were declared probable cases retrospectively [52].
At the time of this outbreak in April, source of the re-
spiratory illnesses was unknown, but it was later deter-
mined to be identical to the novel coronavirus (MERS-
CoV) identified in the following September [52–54]. In
total, nine cases were reported in 2012, and these early
sequences, 389JO12, can be seen at the top of the tree in
Fig. 3.
In January of 2013, UK reported an intra-familial clus-
ter of 3 where the index case had traveled to Pakistan
and Saudi Arabia [8]. The three cases (245GB13, 9GB13
and 10GB13 in Fig. 3) formed a distinct cluster in our
tree, as expected, since the viruses isolated would have
35. great genetic similarity consistent with proximity of the
dates and location of infection. Secondary transmission
occurred in France where the CoV was transmitted to a
patient sharing a hospital room with a MERS confirmed
case who had traveled to UAE [55, 56].
A major outbreak at several hospitals in the Al-Hasa
region of Saudi Arabia occurred around April 2013 where
epidemiological investigation linked 23 MERS cases to
dialysis and intensive care units [57–59]. These are indi-
cated in orange near the middle of the phylogenetic tree
(Fig. 3). From June to August of the same year, there was a
community outbreak in Hafr al-Batin where 12 patients
were infected [60]. Although there was a transmission to a
healthcare worker, the rest of the patients in this cluster
were presumed to have gathered for the large, regional
camel market, and therefore, both zoonotic and human-
to-human transmissions may have occurred simultan-
eously. Interestingly, both the Al-Hasa and Hafr-al-Batin
outbreaks cluster with sequences from Riyadh, which may
indicate travel of persons, and possibly MERS-CoV with
them, to and from this capital city.
In the following year from March to June of 2014, the
biggest outbreak to date was reported from multiple
countries: Saudi Arabia, UAE, Iran and Jordan [61–64].
Sequences from patients during this time distinctly
separated into three clusters, Jeddah cluster (in green),
Abu Dhabi cluster (red) and Riyadh cluster (pink), and
they can be seen forming independent clades on the
tree. And concurrently, there were at least 13 cases of
exported MERS in UAE, Jordan, Philippines, Malaysia,
Algeria, Egypt, Greece, Netherlands, Qatar, United States
(US), Turkey and Austria via travelers who visited Saudi
Arabia as shown in Fig. 5 [1, 26, 65–67].
In 2015, a traveler who visited the Arabian Peninsula
36. was the index case in the largest outbreak of MERS out-
side of the Middle East, affecting 185 patients and inciting
national panic in South Korea [2, 19, 68]. Nosocomial
transmissions were reported from six hospitals, especially
prevalent in two major medical centers, where 3 super-
spreaders have been linked to 166 cases [2]. When total
number of cases are compared, nosocomial incidence is
distinctly greater than incidence of community acquired
Fig. 3 (See legend on next page.)
Min et al. Global Health Research and Policy (2016) 1:14 Page
6 of 14
(See figure on previous page.)
Fig. 3 Time-scaled phylogeographic tree of MERS-CoV
ORF1a/b sequences isolated from humans and camels. Each
color shown in legend represents
city or region of sampled sequence (tip branches) as well as
ancestral lineage (internal branches) inferred by Bayesian
phylogeography. Vertical blue
lines encompass sequences collected at the time of outbreaks
and brown camel symbols indicate sequences isolated from
camels. An asterisk (*) along
the branch represents the posterior probability for each clade
greater than 0.90. Double asterisks (**) indicate > 0.95. Triple
asterisks (***) indicate >0.99
Min et al. Global Health Research and Policy (2016) 1:14 Page
7 of 14
or zoonotic infections (size differences are statistically sig-
37. nificant, p < 0.0001) and superspreading may be the cul-
prit. Son of a Korean MERS patient traveled to China and
tested positive there (313CN15) [69]. The cluster involving
Korean and Chinese samples seem most closely related to
Saudi Arabian strain (465SA15) which was isolated from
Hofuf.
In the Middle East, there was an outbreak in King
Abulaziz Medical Center in Riyadh with 130 cases from
June to August as well as multi-facility outbreaks in
Riyadh and Madinah from September to November of
2015 [1, 26, 70]. In 2016, an outbreak in Buraidah of
Fig. 4 Time-scaled phylogeographic tree of MERS-CoV
ORF1a/b sequences
region of sampled sequence (tip branches) as well as ancestral
lineage (int
posterior probability for the clade >0.90. ** for >0.95 and ***
for >0.99
Saudi Arabia occurred in February and March [1, 26].
And recently, an outbreak in a Riyadh hospital with 24
cases due to superspreading occurred mid-2016 [71].
Basic reproduction number
A wide range of basic reproduction numbers (R0) from
0.32 to 1.3, has been reported for MERS and are summa-
rized in Fig. 6 [9, 14, 21, 72–79]. Most researchers agree
that MERS has a low potential to become a pandemic at
this point in time, but once the CoV is introduced in a
nosocomial setting, the R0 can range from 2 to 6.7 and
even from 7 to 19.3 [75, 78].
isolated from camels. Each color shown in legend represents
city or
ernal branches) inferred by Bayesian phylogeography. *
represents
41. Month 10 11 12 1 2
2016
3 4 5
Fig. 5 Worldwide epidemiological contact tracing summarized
for MERS cases from April 2012 to May 2016. Countries are
listed on the left and
timeline is shown across the middle as x-axis, years indicated
on top of the horizontal black line and months below. Circles
represent the number
of MERS cases reported for the month and blue color is used to
indicate times when hospital related clusters were reported.
Brown camel
symbols indicate possible zoonotic transmissions due to
handling of camels or consumption of its products. Key is
shown in the upper right
hand corner. Arrows indicate travel of MERS cases, with the
tail of the arrow indicating country the patient visited prior to
getting diagnosed in
the country indicated by the arrowhead. In case of multinational
travel, extra arrowheads are used to represent travel stops
Min et al. Global Health Research and Policy (2016) 1:14 Page
8 of 14
Zoonotic transmissions
After two farm workers tested positive for the CoV,
Qatar and WHO carried out an investigation of camel
related MERS cases in October 2013 [80]. All 14 of their
camels tested positive for MERS-CoV antibodies and 11
were positive for the virus itself. The partial sequences
of the MERS-CoV sampled from camels were found gen-
etically similar to the human samples. Parallel case was
observed in Saudi Arabia, where researchers were able
to pinpoint the specific camel that carried a 100% genet-
ically identical virus as the patient [81]. These sequences
42. (11SA13 and 12SA13) can be seen clustering together at
the top of Fig. 4.
Sequences from camels can be seen interspersed
throughout the tree in Fig. 3. When the camel sequences
are examined alone (Fig. 4) it is easy to see that MERS-
CoV from UAE form distinct clusters on their own (in
red) while those from Saudi Arabia seem to have mul-
tiple clades. In our camel subset analysis, the United
Arab Emirates clade diverged from Saudi Arabian
sequences early, right after our estimated time to most
recent common ancestor (tMRCA) of all taxa (March
2012 with 95% confidence intervals: July 2011-November
2012). This clade also includes some Al-Hasa sequences;
Al-Hasa is the easternmost region of Saudi Arabia and
therefore, geographically closest to UAE. The intermixing
of Jeddah and Riyadh sequences in the bottom half of the
tree may be explained by the camel trades that occur be-
tween these two large cities.
We analyzed the data separately for sequences isolated
from humans and camels in order to ascertain when the
introduction of MERS-CoV occurred in humans. For the
main dataset with sequences from humans and camels,
tMRCA was estimated to be September 2008 (95% Con-
fidence Interval: September 2005-June 2011) of Riyadh,
Saudi Arabia origin. For the human subset, tMRCA for
all taxa was March 2011 (CI: June 2009-November
2011), and for the camel subset, tMRCA was March
2012 (CI: July 2011-November 2012) as mentioned
above.
Fig. 6 Summary of reported basic reproduction numbers from
literature. (a) includes all basic reproductive numbers found
43. through literature
search. (b) Close-up excludes hospital specific outbreak R0’s
Min et al. Global Health Research and Policy (2016) 1:14 Page
9 of 14
Discussion
There were three aims for this paper: (1) to examine
case incidence trends over time and geographic area
using epidemiological information, (2) to trace evolu-
tionary history of the virus in circulation using genetic
data and (3) to explore ways in which these two analyses
can be combined to design public health interventions.
While we aimed to have a thorough and complete rep-
resentation of all contact tracing conducted the data may
not be exhaustive. We chose PubMed as the source for
peer-reviewed literature since it contains relevant articles
from life science and medical journals, and we believe the
flexibility in article search and use of MeSH terms are its
strong points. In addition, the database and GenBank are
overseen by the same organization (National Library of
Medicine), which allowed us to link sequence meta-data
with literature. However, PubMed does not include disser-
tations and conference proceedings that may be relevant
and may be biased against articles written in languages
other than English.
Non-heterogeneous sequencing of MERS-CoV is a
limitation of this study. Some patients have been
sampled and had their MERS-CoV sequenced multiple
times while others were not reached. Duplicate se-
quences from single patients were excluded based on
available meta-data since sampling bias can create ap-
parent sinks that are not present in reality [82]. Better
sampling and meta-data annotation would greatly aid
further analysis in this regard.
44. Saudi Arabian sequences dominate the phylogeo-
graphic tree with greatest number of sequences and
large number of probable ancestors (Figs. 3 and 4). This
was expected since overwhelming majority of MERS
cases have been reported there. Although Saudi Arabia
had the largest amount of genetic sequences available
which may skew the phylogenetic analysis, it also had
the most number of MERS cases. Thus, the number of
sequences was relatively proportional to the number of
cases for the country. Saudi Arabia was the most fre-
quent ancestor for many foreign exports, and phylogen-
etic data indicated that the direction of probable
transmission was always from MERS endemic region of
Middle East to non-endemic regions, such as Europe
and Asia.
Min et al. Global Health Research and Policy (2016) 1:14 Page
10 of 14
It has previously been posited that an area with great
population such as central Saudi Arabia, may be a hub
of genetically diverse MERS-CoV’s, introduced by pas-
sage of people and animals [83]. For example, the two
cases exported to US were genetically dissimilar even
though they were both healthcare workers returning
from Saudi Arabia, the 348US14 sequence clustered with
the hospital outbreak of Jeddah 2014 while the other US
sequence 349US14 formed a distinct clade with Riyadh
[84]. The Jeddah sequences seem most genetically simi-
lar to MERS-CoV isolated from a camel in Qatar
(286QA14), even though Jeddah is located in the West
coast of Saudi Arabia and Qatar borders the East. The
intermixing of geographic backgrounds and phylogenetic
clustering seem consistent with the theory on presence
45. of several circulating MERS-CoV’s in Arabian Peninsula
due to movement of animals and people. Geographical
distribution of camels and human MERS-CoV cases are
found to be highly correlated [85]. Since majority of hu-
man cases have been concentrated in the Middle East
and camels in this region showed high seroprevalence of
MERS-CoV antibodies, there has been ongoing testing
in other camel dwelling regions, such as Africa and Asia
[86–89]. Seropositivity ranging from 14.3 to 100% have
been found in countries with dromedaries and a nice
summary covering these studies is provided by Omrani
et al. [90].
The later tMRCA for the camels (March 2012) relative
to tMRCA for CoV isolated from humans (March 2011),
was unexpected since antibodies against MERS-CoV
have been detected in camels from samples archived as
early as 1980s, but this may be due to dearth of early se-
quences from camels [87, 88, 91]. Earliest CoV isolates
from camels were sequenced in 2013 and the short sam-
pling timeframe from 2013 to 2015 makes the root of
the tree less than reliable [92, 93]. While antibodies have
been isolated from archived samples, the virus itself has
not been successfully recovered; these historical samples
may have been isolated in the latter part of the infection
or much later after virus has cleared from the system.
Other studies have shown that the virus most likely
circulated in camels first becoming genetically diver-
gent even within a single country, before jumping to
human hosts, and because of the wide prevalence of
seropositivity along with different lineages of CoV in
camels, more MERS-CoV infections from camels to
humans are bound to occur in the future [49, 87]. Never-
theless, this hypothesis cannot be validated without testing
for MERS-CoV antibodies or even MERS-CoV in historical
human samples [17].
46. Seasonality of MERS has been previously hypothesized
from the high incidence of cases during spring and early
summer months and it has been postulated that this may
be correlated to the camel birthing pattern; young,
newborn camels encountering MERS-CoV for the first
time may get ill and transmit the virus to humans [13, 94,
95]. However, outbreaks in latter half of 2015 and early
2016 countered against the expected seasonality [96].
Infectiousness of MERS-CoV isolated from camels has
been demonstrated by Raj et al., and shepherds and
slaughterhouse workers have been shown to have 15 to
23 times higher proportion of individuals with MERS
antibodies than the general population [97, 98]. And
zoonotic transmission is an important factor to take into
account since evolutionary rates of the virus may be dif-
ferent in humans and camels [99]. As MERS-CoV in
camels seem to be much more prevalent and as shown
here, genetically diverse, contacts with camels should be
engaged with proper personal protection equipment,
and public awareness about MERS-CoV infection related
to camels should be raised.
In surveys conducted regarding MERS awareness of
the Saudi Arabian public, less than half (47.1% and
48.9%) were aware that bats and camels could be pri-
mary sources of MERS-CoV [100, 101]. And there was
an optimistic outlook on the fatality rate and treatment
of the viral infection which may in turn be factors keep-
ing the mild cases from seeking medical attention. Only
half of the pilgrims surveyed by Alqahtani et al. were
aware of MERS and about quarter stated drinking camel
milk or visiting a camel farm as possible activities to be
pursued during Hajj [102]. In a 2013 study, no MERS-
CoV was detected amongst over 1000 pilgrims tested,
47. but 2% of those tested in 2014 were positive [103, 104].
The crowded living quarters during Hajj can impair
adequate infection control, so health agencies have recom-
mend visiting pilgrims to carefully wash hands, consume
hygienic foods and isolate themselves when ill [105, 106].
Awareness among health care providers should be raised
as well. Superspreading is commonly observed in hospital
settings because of the sustained contact in close quarters,
medical treatments generating aerosolized virus and sus-
ceptibility of hospitalized patients [21]. Even in the endemic
nation of Saudi Arabia, the Ministry of Health identified is-
sues such as ambiguity on MERS case definition, inad-
equate infection control and overcrowding to be sources of
hospital outbreaks [107]. Similar concerns have been raised
in Korea as well; doctor shopping and suboptimal infection
control due to crowded hospital rooms seem to have prop-
agated the spread nationwide [19].
An interesting facet of this international analysis was
the difference in outcomes for MERS-CoV infected pa-
tients depending on where they are located. About 41% of
patients in the Middle Eastern and African countries died
[1]. Fatality in Europe was 47% where about half of those
infected died, most likely due to severity of illness in cases
transported there for treatment. Asian countries, on the
other hand, have an atypical 20.3% case fatality.
Min et al. Global Health Research and Policy (2016) 1:14 Page
11 of 14
We attempted to estimate the basic reproduction
number via Bayesian analysis but the mixing of human
and camel sequences with multiple introductions of
MERS-CoV from animals to humans was not possible
48. to model. However, from the literature review, many re-
searchers seem to have reached consistent conclusion
that the R0 is less than 1 even in endemic countries;
notable deviations arose only when MERS-CoV was in-
troduced to a hospital setting then R0 increased by
folds. Superspreading has been cited to be responsible
for this trend since the exponential number of trans-
missions by a few can raise the R0 [76].
Although fundamental and gravely essential part of
epidemiological investigation contact tracing is costly, labor
intensive and prone to human error. Along with many
cases where possible sources of transmissions are unknown,
zoonotic transmissions were at times conjectural, based on
patients’ occupation or recall of food consumption. Never-
theless, we were able to illustrate known and probable
transmission events starting from first known cases of
MERS to recent cases of 2016. In addition, we have
conducted Bayesian phylogeographic analysis of MERS-
CoV strains in both humans and camels, which is the most
up-to-date and comprehensive, to our knowledge.
Purely epidemiological data such as incidence reports
and contact tracing can be prone to inaccuracies but can
provide background information on individual cases and
population level transmission. Genetic data circumvents
human errors and presents quantitative information about
an infectious agent, but it is not fully informative without
accompanying details on collection. Using phylodynamics
to investigate evolutionary history of pathogen can add in-
dispensable details to curb an outbreak such as identifying
most closely related cases and predicting origin of the
virus, revealing additional details at molecular level when
epidemiological tracing is inadequate. As demonstrated
with MERS, combining these two methods in a holistic
approach is valuable for understanding pathogen history
49. and transmission in order to implement effective public
health measures.
Conclusion
Through combination of epidemiological data and genetic
analysis, we present evolutionary history of MERS-CoV
affecting Middle East and beyond with focus on hospital
outbreaks and zoonotic transmissions.
Additional files
Additional file 1: Table S1. List of sequences used for analysis.
Column
“Label” corresponds to labels for sequences. presented in
Figures 3 and 4
with country (by 2-letter ISO country code) and year of
collection; countries,
sources, and dates (month-year) are based on information in
GenBank or
related publication (indicated in Reference column). (DOCX
128 kb)
Additional file 2: Figure S1. Results of recombination analysis.
Out of
all 196 MERS-CoV ORF1a/b sequences, two strains were
detected by
Bootscan/Recscan method in RDP as recombinant strains.
Figure S2.
Likelihood mapping of MERS ORF1a/b (a) main dataset, (b)
human
subset, and (c) camel subset. Main dataset has both camel and
human
sequences. Each dot represents the likelihoods of the three
possible
unrooted trees for a set of four randomly selected sequences:
dots close
to the corners represent tree-like phylogenetic signal and those
50. at the
sides represent network-like signal. The central area of the
likelihood map
represents star-like signal of unresolved phylogenetic
information. Figure S3.
Temporal signal analysis using TempEst. Plots of the root-to-tip
genetic
distance against sampling time are shown for phylogenies
estimated from
three alignments: (a) main dataset with both human and camel
sequences,
(b) human sequences, and (c) camel sequences. Figure S4.
Time-scaled
phylogeographic tree of MERS-CoV ORF1a/b sequences
isolated from
humans and camels by country. Each color shown in legend
represents
country of sampled sequence (tip branches) as well as ancestral
lineage
(internal branches) inferred by Bayesian phylogeography.
Brown camel
symbols represent MERS-CoV sequences isolated from camels.
* represents
posterior probability for the clade >0.90. ** >0.95 and ***
>0.99. Figure S5.
Time-scaled phylogeographic tree of MERS-CoV ORF1a/b
sequences isolated
from humans by city. Each color shown in legend represents
city or region
of sampled sequence (tip branches) as well as ancestral lineage
(internal
branches) inferred by Bayesian phylogeography. * represents
posterior
probability for the clade >0.90. ** for >0.95 and *** for >0.99.
Figure S6.
Time-scaled phylogeographic tree of MERS-CoV ORF1a/b
51. sequences isolated
from humans by country. Each color shown in legend represents
country of
sampled sequence (tip branches) as well as ancestral lineage
(internal
branches) inferred by Bayesian phylogeography. * represents
posterior
probability for the clade >0.90. ** for >0.95 and *** for >0.99.
(ZIP 945 kb)
Abbreviations
CoV: Coronavirus; MCMC: Markov chain Monte Carlo; MERS:
Middle East
respiratory syndrome; MERS-CoV: Middle East respiratory
syndrome-
coronavirus; SARS: Severe acute respiratory syndrome;
tMRCA: Time to most
recent common ancestor
Acknowledgements
None.
Funding
MP and JM are supported by the Virogenesis project. The
VIROGENESIS
project receives funding from the European Union’s Horizon
2020 research
and innovation program under grant agreement No. 634650.
Availability of data and materials
List of all sequences accessed from GenBank [29] are included
in the
Additional file 1.
Authors’ contributions
MS and MP framed the research question. JM collected
52. literature data and EC
conducted all preliminary and bioinformatics analyses with
support from MC. JM
prepared the manuscript. All authors reviewed and approved the
manuscript.
Competing interests
The authors declare that they have no competing interests.
Consent for publication
Not applicable.
Ethics approval and consent to participate
Not applicable.
Author details
1Department of Epidemiology, College of Public Health &
Health Professions
and College of Medicine, University of Florida, 2004 Mowry
Rd, Gainesville, FL
32610-0231, USA. 2Department of Infectious, Parasitic and
Immune-mediated
Diseases, National Institute of Health, Viale Regina Elena, 299,
00161 Rome,
Italy. 3Department of Public Health and Infectious Diseases,
Sapienza
University of Rome, Piazzale Aldo Moro, 5, 00185 Rome, Italy.
4Department of
dx.doi.org/10.1186/s41256-016-0014-7
dx.doi.org/10.1186/s41256-016-0014-7
Min et al. Global Health Research and Policy (2016) 1:14 Page
12 of 14
Pathology, Immunology and Laboratory Medicine, Emerging
53. Pathogens
Institute, University of Florida, 2055 Mowry Rd, Gainesville,
FL 32611, USA.
5Department of Clinical Pathology and Microbiology
Laboratory, University of
Biomedical Campus, Via Alvaro del Portillo, 21, Rome, Italy.
Received: 14 July 2016 Accepted: 14 September 2016
References
1. World Health Organization. WHO | Middle East respiratory
syndrome
coronavirus (MERS-CoV). World Health Organization. 2016.
http://www.who.
int/emergencies/mers-cov/en/. Accessed 26 Jun 2016.
2. Cowling BJ, Park M, Fang VJ, Wu P, Leung GM, Wu JT.
Preliminary
epidemiological assessment of MERS-CoV outbreak in South
Korea, May to
June 2015. Euro Surveill. 2015;20(25):7–13.
3. Chan JFW, Lau SKP, To KKW, Cheng VCC, Woo PCY, Yuen
K-Y. Middle East
Respiratory Syndrome Coronavirus: another zoonotic
betacoronavirus
causing SARS-like disease. Clin Microbiol Rev. 2015;28:465–
522.
4. Coleman CM, Frieman MB. Coronaviruses: important
emerging human
pathogens. J Virol. 2014;88:5209–12.
5. Hu B, Ge X, Wang L-F, Shi Z. Bat origin of human
coronaviruses. Virol J.
54. 2015;12:221.
6. Mohd HA, Al-Tawfiq JA, Memish ZA. Middle East
Respiratory Syndrome
Coronavirus (MERS-CoV) origin and animal reservoir. Virol J.
2016;13:87.
7. van den Brand JM, Smits SL, Haagmans BL. Pathogenesis of
Middle East
respiratory syndrome coronavirus. J Pathol. 2015;235:175–84.
8. Health Protection Agency. Evidence of person-to-person
transmission within
a family cluster of novel coronavirus infections, United
Kingdom, February
2013. Euro Surveill. European Centre for Disease Prevention
and Control
(ECDC) - Health Comunication Unit; 2013.
http://www.eurosurveillance.org/
ViewArticle.aspx?ArticleId=20427. Accessed 21 Dec 2015.
9. Alsolamy S. Middle East Respiratory Syndrome. Crit Care
Med. 2015;43:1283–
90.
10. Korean Ministry of Health and Welfare, Korean Center for
Disease Control
and Prevention. 2015 메르스 [MERS] Incidence Handling Guide.
2015.
http://cdc.go.kr/CDC/cms/cmsFileDownload.jsp?fid=5747&cid=
63292&
fieldName=attach1&index=1. Accessed 19 Oct 2015.
11. Milne-Price S, Miazgowicz KL, Munster VJ. The emergence
of the Middle
East Respiratory Syndrome coronavirus. Pathog Dis.
55. 2014;71:121–36.
12. de Sousa R, Reusken C, Koopmans M. MERS coronavirus:
data gaps for
laboratory preparedness. J Clin Virol. 2014;59:4–11.
13. Al-Tawfiq JA, Memish Z. Middle East respiratory syndrome
coronavirus:
epidemiology and disease control measures. Infect Drug Resist.
2014;3:
281–7.
14. Mackay IM, Arden KE. Middle East respiratory syndrome:
an emerging
coronavirus infection tracked by the crowd. Virus Res.
2015;202:60–88.
15. Otter JA, Donskey C, Yezli S, Douthwaite S, Goldenberg
SD, Weber DJ.
Transmission of SARS and MERS coronaviruses and influenza
virus in
healthcare settings: the possible role of dry surface
contamination. J Hosp
Infect. 2016;92:235–50.
16. Bin SY, Heo JY, Song MS, Lee J, Kim EH, Park SJ, et al.
Environmental
contamination and viral shedding in MERS patients during
MERS-CoV
outbreak in South Korea. Clin Infect Dis. 2015;62:755–60.
17. Zumla A, Hui DS, Perlman S. Middle East respiratory
syndrome. Lancet. 2015;
386:995–1007.
18. Al-Tawfiq JA, Memish ZA. Middle East respiratory
56. syndrome coronavirus:
transmission and phylogenetic evolution. Trends Microbiol.
2014;22:573–9.
19. Ki M. 2015 MERS outbreak in Korea: hospital-to-hospital
transmission.
Epidemiol Health. 2015;37:e2015033.
20. Lu G, Wang Q, Gao GF. Bat-to-human: spike features
determining “host
jump” of coronaviruses SARS-CoV, MERS-CoV, and beyond.
Trends Microbiol.
2015;23:468–78.
21. Chowell G, Abdirizak F, Lee S, Lee J, Jung E, Nishiura H,
et al. Transmission
characteristics of MERS and SARS in the healthcare setting: a
comparative
study. BMC Med. 2015;13:210.
22. Durai P, Batool M, Shah M, Choi S. Middle East respiratory
syndrome
coronavirus: transmission, virology and therapeutic targeting to
aid in
outbreak control. Exp Mol Med. 2015;47:e181.
23. Grenfell BT, Pybus OG, Gog JR, Wood JLN, Daly JM,
Mumford JA, et al.
Unifying the epidemiological and evolutionary dynamics of
pathogens.
Science. 2004;303:327–32.
24. Khan KS, Kunz R, Kleijnen J, Antes G. Five steps to
conducting a systematic
review. J R Soc Med. 2003;96:118–21.
25. Korean Ministry of Health and Wellfare. Hospitals with
57. known MERS
exposure July 10. 2015.
http://photos.state.gov/libraries/korea/187344/ACS/
List_of_MERS_affected_Hospitals.pdf. Accessed 19 Oct 2015.
26. European Centre for Disease Prevention and Control. News
and
epidemiological updates. 2016.
http://ecdc.europa.eu/en/healthtopics/
coronavirus-
infections/Pages/news_and_epidemiological_updates.aspx.
Accessed 26 June 2016.
27. SAS. http://www.sas.com/en_us/software/sas9.html.
Accessed 1 Aug 2015.
28. Evidence Partners. DistillerSR Forest Plot Generator.
https://distillercer.com/
resources/forest-plot-generator/. Accessed 2 May 2016.
29. NCBI. GenBank. http://www.ncbi.nlm.nih.gov/genbank/.
Accessed 16 Mar
2016.
30. Thompson JD, Gibson TJ, Plewniak F, Jeanmougin F,
Higgins DG. The
CLUSTAL_X windows interface: flexible strategies for multiple
sequence
alignment aided by quality analysis tools. Nucleic Acids Res.
1997;25:4876–82.
31. Hall T. BioEdit: a user-friendly biological sequence
alignment editor and
analysis program for Windows 95/98/NT. Nucleic Acids Symp
Ser. 1999;41:
95–8.
58. 32. Swofford DL. PAUP*. Phylogenetic Analysis Using
Parsimony (*and Other
Methods). Vers. 4.0. Sunderland, Massachusetts: Sinauer
Associates; 2002.
http://people.sc.fsu.edu/~dswofford/paup_test/. Accessed 22 Jan
2016.
33. Posada D, Crandall KA. MODELTEST: testing the model of
DNA substitution.
Bioinformatics. 1998;14:817–8.
34. Martin DP, Murrell B, Golden M, Khoosal A, Muhire B.
RDP4: detection and
analysis of recombination patterns in virus genomes. Virus
Evol. 2015;1:1–5.
35. Martin D, Posada D, Crandall K, Williamson C. A modified
bootscan
algorithm for automated identification of recombinant
sequences and
recombination breakpoints. AIDS Res Hum Retroviruses.
2005;21:98–102.
36. Schmidt HA, Strimmer K, Vingron M, von Haeseler A.
TREE-PUZZLE:
maximum likelihood phylogenetic analysis using quartets and
parallel
computing. Bioinformatics. 2002;18:502–4.
37. Strimmer K, von Haeseler A. Likelihood-mapping: a simple
method to
visualize phylogenetic content of a sequence alignment. Proc
Natl Acad Sci
U S A. 1997;94:6815–9.
59. 38. Rambaut A, Lam TT, Carvalho LM, Pybus OG. Exploring
the temporal
structure of heterochronous sequences using TempEst (formerly
Path-O-
Gen). Virus Evol. 2016;2:vew007.
39. Drummond AJ, Suchard MA, Xie D, Rambaut A. Bayesian
phylogenetics with
BEAUti and the BEAST 1.7. Mol Biol Evol. 2012;29:1969–73.
40. Drummond AJ, Rambaut A, Shapiro B, Pybus OG. Bayesian
coalescent
inference of past population dynamics from molecular
sequences. Mol Biol
Evol. 2005;22:1185–92.
41. Minin VN, Bloomquist EW, Suchard MA. Smooth skyride
through a rough
skyline: Bayesian coalescent-based inference of population
dynamics. Mol
Biol Evol. 2008;25:1459–71.
42. Drummond AJ, Nicholls GK, Rodrigo AG, Solomon W.
Estimating mutation
parameters, population history and genealogy simultaneously
from
temporally spaced sequence data. Genetics. 2002;161:1307–20.
43. Baele G, Lemey P, Bedford T, Rambaut A, Suchard MA,
Alekseyenko AV.
Improving the accuracy of demographic and molecular clock
model
comparison while accommodating phylogenetic uncertainty.
Mol Biol Evol.
2012;29:2157–67.
60. 44. Baele G, Lemey P. Bayesian evolutionary model testing in
the
phylogenomics era: matching model complexity with
computational
efficiency. Bioinformatics. 2013;29:1970–9.
45. Kass RE, Raftery AE. Bayes factors. J Am Stat Assoc.
1995;90:773–95.
46. Lemey P, Rambaut A, Drummond AJ, Suchard MA.
Bayesian
phylogeography finds its roots. PLoS Comput Biol.
2009;5:e1000520.
47. Lemey P, Rambaut A, Welch JJ, Suchard MA.
Phylogeography takes a relaxed
random walk in continuous space and time. Mol Biol Evol.
2010;27:1877–85.
48. Drosten C, Seilmaier M, Corman VM, Hartmann W,
Scheible G, Sack S, et al.
Clinical features and virological analysis of a case of Middle
East respiratory
syndrome coronavirus infection. Lancet Infect Dis.
2013;13:745–51.
49. Sabir JSM, Lam TT-Y, Ahmed MMM, Li L, Shen Y, Abo-
Aba SE, et al. Co-
circulation of three camel coronavirus species and
recombination of MERS-
CoVs in Saudi Arabia. Science. 2016;351:81–4.
50. Seong M-W, Kim SY, Corman VM, Kim TS, Cho SI, Kim
MJ, et al.
Microevolution of outbreak-associated Middle East Respiratory
Syndrome
61. Coronavirus, South Korea, 2015. Emerg Infect Dis.
2016;22:327–30.
Min et al. Global Health Research and Policy (2016) 1:14 Page
13 of 14
51. Kim JI, Kim Y-J, Lemey P, Lee I, Park S, Bae J-Y, et al.
The recent ancestry of
Middle East respiratory syndrome coronavirus in Korea has
been shaped by
recombination. Sci Rep. 2016;6:18825.
52. Hijawi B, Abdallat M, Sayaydeh A, Alqasrawi S, Haddadin
A, Jaarour N, et al.
Novel coronavirus infections in Jordan, April 2012:
epidemiological findings
from a retrospective investigation. East Mediterr Heal J.
2013;19:S12–8.
53. van Boheemen S, de Graaf M, Lauber C, Bestebroer TM,
Raj VS, Zaki AM, et al.
Genomic characterization of a newly discovered coronavirus
associated with
acute respiratory distress syndrome in humans. MBio.
2012;3:e00473–12.
54. Bermingham A, Chand MA, Brown CS, Aarons E, Tong C,
Langrish C, et al.
Severe respiratory illness caused by a novel coronavirus, in a
patient
transferred to the United Kingdom from the Middle East,
September 2012.
Euro Surveillance. 2012;17:20290.
55. Mailles A, Blanckaert K, Chaud P, van der Werf S, Lina B,
62. Caro V, et al. First
cases of middle east respiratory syndrome coronavirus (MERS-
COV)
infections in France, investigations and implications for the
prevention of
human-to-human transmission, France, May 2013. Euro
Surveill. 2013;18.
56. Guery B, Poissy J, el Mansouf L, Séjourné C, Ettahar N,
Lemaire X, et al.
Clinical features and viral diagnosis of two cases of infection
with Middle
East Respiratory Syndrome coronavirus: a report of nosocomial
transmission.
Lancet. 2013;381:2265–72.
57. Assiri A, Al-Tawfiq JA, Al-Rabeeah AA, Al-Rabiah FA, Al-
Hajjar S, Al-Barrak A,
et al. Epidemiological, demographic, and clinical characteristics
of 47 cases
of Middle East respiratory syndrome coronavirus disease from
Saudi Arabia:
a descriptive study. Lancet Infect Dis. 2013;13:752–61.
58. Assiri A, McGeer A, Perl TM, Price CS, Al Rabeeah AA,
Cummings DAT, et al.
Hospital outbreak of Middle East respiratory syndrome
coronavirus. N Engl J
Med. 2013;369:407–16.
59. Cotten M, Watson SJ, Kellam P, Al-Rabeeah AA,
Makhdoom HQ, Assiri A,
et al. Transmission and evolution of the Middle East respiratory
syndrome
coronavirus in Saudi Arabia: a descriptive genomic study.
Lancet. 2013;382:
63. 1993–2002.
60. Memish ZA, Cotten M, Watson SJ, Kellam P, Zumla A,
Alhakeem RF, et al.
Community case clusters of Middle East Respiratory Syndrome
Coronavirus
in Hafr Al-Batin, Kingdom of Saudi Arabia: a descriptive
genomic study. Int J
Infect Dis. 2014;23:63–8.
61. Yavarian J, Rezaei F, Shadab A, Soroush M, Gooya MM,
Azad TM. Cluster of
Middle East Respiratory Syndrome Coronavirus infections in
Iran, 2014.
Emerg Infect Dis. 2015;21:362–4.
62. Fagbo SF, Skakni L, Chu DKW, Garbati MA, Joseph M,
Peiris M, et al.
Molecular epidemiology of hospital outbreak of Middle East
Respiratory
Syndrome, Riyadh, Saudi Arabia, 2014. Emerg Infect Dis.
2015;21:1981–8.
63. Hastings DL, Tokars JI, Abdel Aziz IZAM, Alkhaldi KZ,
Bensadek AT, Alraddadi
BM, et al. Outbreak of Middle East Respiratory Syndrome at
tertiary care
hospital, Jeddah, Saudi Arabia, 2014. Emerg Infect Dis.
2016;22:794–801.
64. Oboho IK, Tomczyk SM, Al-Asmari AM, Banjar AA, Al-
Mugti H, Aloraini MS,
et al. 2014 MERS-CoV outbreak in Jeddah — a link to health
care facilities. N
Engl J Med. 2015;372:846–54.
64. 65. Drosten C, Muth D, Corman VM, Hussain R, Al Masri M,
HajOmar W, et al. An
observational, laboratory-based study of outbreaks of Middle
East
Respiratory Syndrome Coronavirus in Jeddah and Riyadh,
Kingdom of Saudi
Arabia, 2014. Clin Infect Dis. 2015;60:369–77.
66. Kraaij-Dirkzwager M, Timen A, Dirksen K, Gelinck L,
Leyten E, Groeneveld P,
et al. Middle East respiratory syndrome coronavirus (MERS-
CoV) infections in
two returning travellers in the Netherlands, May 2014. Euro
Surveill. 2014;
19(21):2–7.
67. Kossyvakis A, Tao Y, Lu X, Pogka V, Tsiodras S,
Emmanouil M, et al.
Laboratory investigation and phylogenetic analysis of an
imported Middle
East Respiratory Syndrome Coronavirus case in Greece. PLoS
One. 2015;10:
e0125809.
68. Korean Center for Disease Control and Prevention. Middle
East Respiratory
Syndrome Coronavirus outbreak in the Republic of Korea, 2015.
Osong
Public Health Res Perspect. 2015;6:269–78.
69. Lu R, Wang Y, Wang W, Nie K, Zhao Y, Su J, et al.
Complete genome
sequence of Middle East Respiratory Syndrome Coronavirus
(MERS-CoV)
from the first imported MERS-CoV case in China. Genome
Announc. 2015;3:
65. e00818–15.
70. Balkhy HH, Alenazi TH, Alshamrani MM, Baffoe-Bonnie H,
Al-Abdely HM, El-
Saed A, et al. Nosocomial outbreak of Middle East Respiratory
Syndrome in
a large tertiary care hospital — Riyadh, Saudi Arabia, 2015.
Morb Mortal
Wkly Rep. 2016;65:163–4.
71. World Health Organization. Middle East respiratory
syndrome coronavirus
(MERS-CoV) – Saudi Arabia. 2016.
http://www.who.int/csr/don/21-june-2016-
mers-saudi-arabia/en/. Accessed 23 Jun 2016.
72. Cauchemez S, Fraser C, Van Kerkhove MD, Donnelly CA,
Riley S, Rambaut A,
et al. Middle East respiratory syndrome coronavirus:
quantification of the
extent of the epidemic, surveillance biases, and transmissibility.
Lancet Infec
Dis. 2014;14:50–6.
73. Breban R, Riou J, Fontanet A. Interhuman transmissibility
of Middle East
respiratory syndrome coronavirus: estimation of pandemic risk.
Lancet. 2013;
382:694–9.
74. Poletto C, Pelat C, Lévy-Bruhl D, Yazdanpanah Y, Boëlle P,
Colizza V.
Assessment of the Middle East respiratory syndrome
coronavirus (MERS-CoV)
epidemic in the Middle East and risk of international spread
using a novel
maximum likelihood analysis approach. Euro Surveill.
66. 2014;19(23):13–22.
75. Majumder MS, Rivers C, Lofgren E, Fisman D. Estimation
of MERS-
Coronavirus reproductive number and case fatality rate for the
spring 2014
Saudi Arabia outbreak: insights from publicly available data.
PLoS Curr. 2014;
6:ecurrents.outbreaks.98d2f8f3382d84f390736cd5f5fe133c.
76. Kucharski AJ, Althaus CL. The role of superspreading in
Middle East
respiratory syndrome coronavirus (MERS-CoV) transmission.
Euro Surveill.
2015;20(25):14–18.
77. Nishiura H, Miyamatsu Y, Chowell G, Saitoh M. Assessing
the risk of
observing multiple generations of Middle East respiratory
syndrome (MERS)
cases given an imported case. Euro Surveill. 2015;20(27):6–11.
78. Hsieh Y-H. 2015 Middle East Respiratory Syndrome
Coronavirus (MERS-CoV)
nosocomial outbreak in South Korea: insights from modeling.
PeerJ. 2015;3:e1505.
79. Kucharski AJ, Edmunds WJ. Characterizing the transmission
potential of
zoonotic infections from minor outbreaks. PLoS Comput Biol.
2015;11:
e1004154.
80. Haagmans BL, Al Dhahiry SHS, Reusken CBEM, Raj VS,
Galiano M, Myers R,
et al. Middle East respiratory syndrome coronavirus in
67. dromedary camels: an
outbreak investigation. Lancet Infect Dis. 2014;14:140–5.
81. Azhar EI, El-Kafrawy SA, Farraj SA, Hassan AM, Al-Saeed
MS, Hashem AM, et
al. Evidence for camel-to-human transmission of MERS
Coronavirus. N Engl J
Med. 2014;370:2499–505.
82. Frost SDW, Pybus OG, Gog JR, Viboud C, Bonhoeffer S,
Bedford T. Eight
challenges in phylodynamic inference. Epidemics. 2015;10:88–
92.
83. Cotten M, Watson SJ, Zumla AI, Makhdoom HQ, Palser AL,
Ong SH, et al.
Spread, circulation, and evolution of the Middle East
Respiratory Syndrome
Coronavirus. MBio. 2014;5:e01062–13.
84. Kapoor M, Pringle K, Kumar A, Dearth S, Liu L, Lovchik J,
et al. Clinical and
laboratory findings of the first imported case of Middle East
Respiratory
Syndrome Coronavirus to the United States. Clin Infect Dis.
2014;59:1511–8.
85. Hemida MG, Elmoslemany A, Al-Hizab F, Alnaeem A,
Almathen F, Faye B,
et al. Dromedary camels and the transmission of Middle East
Respiratory
Syndrome Coronavirus (MERS-CoV). Transbound Emerg Dis.
2015. doi:10.
1111/tbed.12401.
86. Perera R, Wang P, Gomaa M, El-Shesheny R, Kandeil A,
68. Bagato O, et al.
Seroepidemiology for MERS coronavirus using
microneutralisation and
pseudoparticle virus neutralisation assays reveal a high
prevalence of
antibody in dromedary camels in Egypt, June 2013. Euro
Surveill. 2013;
18(36):8–14.
87. Alagaili AN, Briese T, Mishra N, Kapoor V, Sameroff SC,
de Wit E, et al. Middle
East Respiratory Syndrome Coronavirus infection in dromedary
camels in
Saudi Arabia. MBio. 2014;5:e00884–14.
88. Alexandersen S, Kobinger GP, Soule G, Wernery U. Middle
East Respiratory
Syndrome Coronavirus antibody reactors among camels in
Dubai, United
Arab Emirates, in 2005. Transbound Emerg Dis. 2014;61:105–8.
89. Nowotny N, Kolodziejek J. Middle East respiratory
syndrome coronavirus
(MERS-CoV) in dromedary camels, Oman, 2013. Euro Surveill.
2014;19:20781.
90. Omrani AS, Al-Tawfiq JA, Memish ZA. Middle East
respiratory syndrome
coronavirus (MERS-CoV): animal to human interaction. Pathog
Glob Health.
2015;109:354–62.
91. Müller MA, Corman VM, Jores J, Meyer B, Younan M,
Liljander A, et al. MERS
Coronavirus Neutralizing Antibodies in Camels, Eastern Africa,
1983–1997.
69. Emerg Infect Dis. 2014;20:2093–5.
92. Briese T, Mishra N, Jain K, Zalmout IS, Jabado OJ, Karesh
WB, et al. Middle
East Respiratory Syndrome Coronavirus quasispecies that
include
homologues of human isolates revealed through whole-genome
analysis
and virus cultured from dromedary camels in Saudi Arabia.
MBio. 2014;5:
e01146–14.
Min et al. Global Health Research and Policy (2016) 1:14 Page
14 of 14
93. Chu DKW, Poon LLM, Gomaa MM, Shehata MM, Perera
RAPM, Abu Zeid D,
et al. MERS Coronaviruses in dromedary Camels, Egypt. Emerg
Infect Dis.
2014;20:1049–53.
94. Wernery U, Corman VM, Wong EYM, Tsang AKL, Muth D,
Lau SKP, et al.
Acute Middle East Respiratory Syndrome Coronavirus infection
in livestock
dromedaries, Dubai, 2014. Emerg Infect Dis. 2015;21:1019–22.
95. Memish ZA, Cotten M, Meyer B, Watson SJ, Alsahafi AJ,
Al Rabeeah AA, et al.
Human infection with MERS Coronavirus after exposure to
infected camels,
Saudi Arabia, 2013. Emerg Infect Dis. 2014;20:1012–5.
96. Wernery U, El Rasoul IH, Wong EY, Joseph M, Chen Y,
Jose S, et al. A
70. phylogenetically distinct Middle East respiratory syndrome
coronavirus
detected in a dromedary calf from a closed dairy herd in Dubai
with rising
seroprevalence with age. Emerg Microbes Infect. 2015;4:e74.
97. Müller MA, Meyer B, Corman VM, Al-Masri M, Turkestani
A, Ritz D, et al.
Presence of Middle East respiratory syndrome coronavirus
antibodies in
Saudi Arabia: a nationwide, cross-sectional, serological study.
Lancet Infect
Dis. 2015;15:559–64.
98. Raj VS, Farag EABA, Reusken CBEM, Lamers MM, Pas
SD, Voermans J, et al.
Isolation of MERS Coronavirus from a dromedary camel, Qatar,
2014. Emerg
Infect Dis. 2014;20:1339–42.
99. Gray RR, Salemi M. Integrative molecular phylogeography
in the context of
infectious diseases on the human-animal interface. Parasitology.
2012;139:
1939–51.
100. Al-Mohrej OA, Al-Shirian SD, Al-Otaibi SK, Tamim HM,
Masuadi EM, Fakhoury
HM. Is the Saudi public aware of Middle East respiratory
syndrome? J Infect
Public Health. 2016;9:259–66.
101. Almutairi KM, Al Helih EM, Moussa M, Boshaiqah AE,
Saleh Alajilan A,
Vinluan JM, et al. Awareness, attitudes, and practices related to
coronavirus
71. pandemic among public in Saudi Arabia. Fam Community
Health. 2015;38:
332–40.
102. Alqahtani AS, Wiley KE, Tashani M, Heywood AE,
Willaby HW, BinDhim NF,
et al. Camel exposure and knowledge about MERS-CoV among
Australian
Hajj pilgrims in 2014. Virol Sin. 2016;31:89–93.
103. Barasheed O, Rashid H, Alfelali M, Tashani M, Azeem M,
Bokhary H, et al.
Viral respiratory infections among Hajj pilgrims in 2013. Virol
Sin. 2014;29:
364–71.
104. Memish ZA, Al-Tawfiq JA, Makhdoom HQ, Al-Rabeeah
AA, Assiri A,
Alhakeem RF, et al. Screening for Middle East respiratory
syndrome
coronavirus infection in hospital patients and their healthcare
worker and
family contacts: a prospective descriptive study. Clin Microbiol
Infect. 2014;
20:469–74.
105. Department of Health. Travel Health Service Advice for
pilgrims visiting
Mecca, Saudi Arabia (Hajj and Umrah). Government of
HKSAR. 2014. http://
www.travelhealth.gov.hk/english/travel_special_needs/pilgrims.
html.
Accessed 29 Dec 2015.
106. Watson JT, Gerber SI. Middle East Respiratory Syndrome
(MERS). In: Brunette
72. GW, editor. CDC Heal Inf Int Travel. New York: Centers for
Disease Control
and Prevention; 2016.
http://wwwnc.cdc.gov/travel/yellowbook/2016/
infectious-diseases-related-to-travel/middle-east-respiratory-
syndrome-mers.
Accessed 29 Dec 2015.
107. Kingdom of Saudi Arabia Ministry of Health. Weekly
Monitor MERS-CoV.
2016. http://www.moh.gov.sa/en/CCC/Documents/Volume-2-
Issue15-
Tuesday-April 12-2016%E2%80%8B.pdf. Accessed 2 July 2016.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript at
www.biomedcentral.com/submit
Submit your next manuscript to BioMed Central
and we will help you at every step:
AbstractBackgroundMethodsResultsConclusionBackgroundMER
S-CoVMiddle East Respiratory SyndromePossibility of global
outbreakMethodsLiterature reviewMERS-CoV genetic
sequencesPreliminary analysisCoalescent model for
demographic historyPhylogeographic
analysesResultsPhylodynamic analysisOverview of outbreaks
and exportsBasic reproduction numberZoonotic
transmissionsDiscussionConclusionAdditional filesshow
[a]AcknowledgementsFundingAvailability of data and
materialsAuthors’ contributionsCompeting interestsConsent for
73. publicationEthics approval and consent to participateAuthor
detailsReferences
Middle East Respiratory Syndrome
Yaseen M. Arabi, M.D., Hanan H. Balkhy, M.D., Frederick G.
Hayden, M.D., Abderrezak
Bouchama, M.D., Thomas Luke, M.D., J. Kenneth Baillie, M.D.,
Ph.D., Awad Al-Omari, M.D.,
Ali H. Hajeer, Ph.D., Mikiko Senga, Ph.D., Mark R. Denison,
M.D., Jonathan S. Nguyen-Van-
Tam, D.M., Nahoko Shindo, M.D., Ph.D., Alison Bermingham,
Ph.D., James D. Chappell,
M.D., Ph.D., Maria D. Van Kerkhove, Ph.D., and Robert A.
Fowler, M.D., C.M., M.S. (Epi)
From the Departments of Intensive Care (Y.M.A., A.
Bouchama), Infection Prevention and Control
(H.H.B.), and Pathology and Laboratory (A.H.H.), King
Abdulaziz Medical City, King Saud bin
Abdulaziz University for Health Sciences, King Abdullah
International Medical Research Center
(Y.M.A., H.H.B., A. Bouchama, A.H.H.), the Department of
Intensive Care, Dr. Sulaiman Al-Habib
Group Hospitals (A.A.-O.), and Alfaisal University (A.A.-O.)
— all in Riyadh, Saudi Arabia; the
Department of Medicine, Division of Infectious Diseases and
International Health, University of
Virginia School of Medicine, Charlottesville (F.G.H.); the
Department of Viral and Rickettsial
Diseases, Naval Medical Research Center, Silver Spring, MD
(T.L.); the Roslin Institute,
University of Edinburgh, and Intensive Care Unit, Royal
Infirmary of Edinburgh, Edinburgh
(J.K.B.), the Health Protection and Influenza Research Group,
74. Division of Epidemiology and
Public Health, University of Nottingham, Nottingham (J.S.N.-
V.-T.), and the Virus Reference
Laboratory, Public Health England, London (A. Bermingham)
— all in the United Kingdom; the
Department of Pandemic and Epidemic Diseases, World Health
Organization, Geneva (M.S.,
N.S., R.A.F.); the Department of Pediatrics, Vanderbilt
University School of Medicine, Nashville
(M.R.D., J.D.C.); the Center for Global Health, Institut Pasteur,
Paris (M.D.V.K.); and the Institute
of Health Policy Management and Evaluation, University of
Toronto, and the Department of
Critical Care Medicine and Department of Medicine,
Sunnybrook Health Sciences Centre — both
in Toronto (R.A.F.).
Summary
Between September 2012 and January 20, 2017, the World
Health Organization (WHO) received
reports from 27 countries of 1879 laboratory-confirmed cases in
humans of the Middle East
Address reprint requests to Dr. Arabi at King Saud bin
Abdulaziz University for Health Sciences, King Abdulaziz
Medical City, P.O.
Box 22490, Riyadh, 11426, Saudi Arabia, or at
[email protected]
Dr. Bermingham is deceased.
Drs. Senga and Shindo are staff members of and Drs. Fowler,
Hayden, Nguyen-Van-Tam, and Van Kerkhove are consultants
for the
World Health Organization. The authors alone are responsible
75. for the views expressed in this article, and they do not
necessarily
represent the decisions, policy, or views of the World Health
Organization. Dr. Luke is an employee of the U.S. Federal
Government.
The views expressed in this article are his and do not
necessarily reflect the official policy or position of the
Department of the Navy,
Department of Defense, or the U.S. Government. This work was
prepared as part of his official duties. Title 17 U.S.C. §105
provides
that “Copyright protection under this title is not available for
any work of the United States Government.” Title 17 U.S.C.
§101 defines
a U.S. Government work as a work prepared by a military
service member or employee of the U.S. Government as part of
that
person’s official duties.
Disclosure forms provided by the authors are available with the
full text of this article at NEJM.org.
We thank Sibylle Bernard Stoecklin for her help in generating
the data for Figure 1.
This article is dedicated to all patients and families who have
suffered because of Middle East respiratory syndrome, as well
as to the
memory of Dr. Allison Bermingham, scientist and colleague,
who died unexpectedly during the preparation of this work.
Europe PMC Funders Group
Author Manuscript
N Engl J Med. Author manuscript; available in PMC 2017
August 09.
Published in final edited form as:
76. N Engl J Med. 2017 February 09; 376(6): 584–594.
doi:10.1056/NEJMsr1408795.
E
urope P
M
C
F
unders A
uthor M
anuscripts
E
urope P
M
C
F
unders A
uthor M
anuscripts
http://www.nejm.org/
respiratory syndrome (MERS) caused by infection with the
MERS coronavirus (MERS-CoV) and
at least 659 related deaths. Cases of MERS-CoV infection
continue to occur, including sporadic
77. zoonotic infections in humans across the Arabian Peninsula,
occasional importations and
associated clusters in other regions, and outbreaks of
nonsustained human-to-human transmission
in health care settings. Dromedary camels are considered to be
the most likely source of animal-to-
human transmission. MERS-CoV enters host cells after binding
the dipeptidyl peptidase 4
(DPP-4) receptor and the carcinoembryonic antigen–related
cell-adhesion molecule 5
(CEACAM5) cofactor ligand, and it replicates efficiently in the
human respiratory epithelium.
Illness begins after an incubation period of 2 to 14 days and
frequently results in hypoxemic
respiratory failure and the need for multiorgan support.
However, asymptomatic and mild cases
also occur. Real-time reverse-transcription–polymerase-chain-
reaction (RT-PCR) testing of
respiratory secretions is the mainstay for diagnosis, and samples
from the lower respiratory tract
have the greatest yield among seriously ill patients. There is no
antiviral therapy of proven
efficacy, and thus treatment remains largely supportive;
potential vaccines are at an early
78. developmental stage. There are multiple gaps in knowledge
regarding the evolution and
transmission of the virus, disease pathogenesis, treatment, and
prospects for a vaccine. The
ongoing occurrence of MERS in humans and the associated high
mortality call for a continued
collaborative approach toward gaining a better understanding of
the infection both in humans and
in animals.
MERS-CoV was first identified in September 20121 in a patient
from Saudi Arabia who had
hypoxemic respiratory failure and multiorgan illness.
Subsequent cases have included infections in
humans across the Arabian Peninsula, occasional importations
and associated clusters in other
regions, and outbreaks of nonsustained human-to-human
transmission in health care settings (Fig.
1).
Epidemiology
Overview
As of January 20, 2017, the WHO had received reports from 27
countries of 1879 cases of
laboratory-confirmed MERS and at least 659 related deaths
79. (percentage of fatal cases, 35%).
2 Approximately 80% of reported cases have been linked to
exposure in Saudi Arabia (Fig.
2). Transmission of MERS-CoV between dromedary camels and
humans has been
documented in several countries. Human-to-human transmission
in health care settings
accounts for the majority of reported cases to date, although
human-to-human transmission
in household settings has also been identified (Fig. 3).
Animal-to-Human Transmission
Seroepidemiologic studies have shown that antibodies to
MERS-CoV are present in
dromedary camels (Camelus dromedarius) throughout the
Middle East and Africa, and
studies indicate that MERS-CoV has circulated among
dromedaries for at least three
decades. Although MERS-CoV RNA has been detected in
respiratory and other bodily
secretions, particularly among juvenile dromedaries, infections
in dromedaries may cause
only mild upper respiratory manifestations. Investigations of
animals in close proximity to
reported cases in humans support the theory that dromedaries
80. are the most likely source of
Arabi et al. Page 2
N Engl J Med. Author manuscript; available in PMC 2017
August 09.
E
urope P
M
C
F
unders A
uthor M
anuscripts
E
urope P
M
C
F
unders A
uthor M
anuscripts
animal-to-human transmission.5 One case–control study showed
that persons presenting
81. with community-acquired MERS were 7 times as likely as
controls to have had direct
exposure to dromedaries during the preceding 2 weeks.6 In
addition, seroepidemiologic
studies indicate that infection may be associated with
occupational exposures to
dromedaries. In one study conducted in Saudi Arabia, the rate
of MERS-CoV seropositivity
was 15 times as high in shepherds and 23 times as high in
slaughterhouse workers as in the
general population.7 There is high sequence homology between
the viruses from sporadic
cases in humans and the implicated dromedaries. Although the
routes of transmission remain
unclear, they appear to include contact with infectious nasal or
other bodily secretions and
possibly the consumption of raw dromedary products (e.g.,
unpasteurized milk). Although
dromedary-to-human transmission of MERS-CoV is now well
recognized, direct exposure
to dromedaries has been documented in only 40% of primary
cases.6 (For further details, see
Tables S1 and S2 in the Supplementary Appendix, available
with the full text of this article
82. at NEJM.org.)
Human-to-Human Transmission
Non–Health Care Settings—Human-to-human transmission
appears to be infrequent
outside health care settings but has been documented after close
household contact with
infected persons.8 Among 280 household contacts evaluated in
a study conducted in Saudi
Arabia, 4.3% had positive results for MERS-CoV on realtime
RT-PCR assay or serologic
assay.9 In one household cluster in which 24% of 79 extended
family members were
affected, risk factors for infection included sleeping in an index
patient’s room and touching
respiratory secretions from an index patient.10 Very little or no
household transmission has
been detected in other countries in which MERS-CoV infections
have been reported,11 and
no sustained human-to-human transmission has been
documented in any country to date.
One seroepidemiologic study conducted in Saudi Arabia with
the use of samples collected in
2012–2013 showed that antibodies to MERS-CoV were present
in 0.15% of 10,009
83. participants; this finding suggests that more than 40,000
unrecognized infections may have
occurred.7 During the 2014 outbreak in Jeddah, Saudi Arabia,
25% of MERS cases were
reported to be asymptomatic.12 The role of persons with
asymptomatic infections in human-
to-human transmission remains unclear but may be
underappreciated.7,13 Increasingly
sensitive surveillance strategies and follow-up for all contacts
are contributing to the
increased recognition of asymptomatic cases.12,14
Health Care Settings—The earliest cases of MERS were
identified retrospectively in a
hospital-associated cluster in Jordan in April 2012,15 and
transmission within health care
settings has remained a prominent epidemiologic feature of
MERS. During the 2014 MERS
outbreak in Jeddah, 31% of the affected patients were health
care personnel, and 88% of the
affected patients who were not health care personnel had been
admitted to or visited a health
care facility within 14 days before symptom onset.12 During
2015 and 2016, nosocomial
outbreaks occurred in health care facilities in Jordan,2 South
Korea,14 and Saudi Arabia.16
84. In the Korean outbreak, which has been the largest outbreak
outside the Middle East,
transmission from a single infected person led to 186 cases and
36 deaths (case fatality rate,
19.4%) across multiple health care facilities.14 Overcrowded
emergency departments,
Arabi et al. Page 3
N Engl J Med. Author manuscript; available in PMC 2017
August 09.
E
urope P
M
C
F
unders A
uthor M
anuscripts
E
urope P
M
C
F
unders A
85. uthor M
anuscripts
delays in diagnosis, and substandard practices for infection
control have been identified as
contributing factors in outbreaks that occur in health care
settings.12,17
Available epidemiologic observations suggest that human-to-
human transmission occurs
primarily through close contact with a patient who has
confirmed MERS, most likely
through respiratory droplets. The risk of transmission appears to
be greater during the
performance of aerosol-generating procedures without adequate
personal protection or
proper room ventilation.18 In addition, contamination of
environmental surfaces in patient
rooms with MERS-CoV may result in transmission.19,20 One
study isolated the infectious
virus from air samples from MERS isolation wards, although
this finding requires
confirmation.20
Travel to and from the Arabian Peninsula—Persons with MERS
who have been
86. identified in regions other than the Arabian Peninsula have
either recently traveled to the
Arabian Peninsula or have had contact with someone returning
from the Arabian Peninsula.
21 Despite the large number of persons visiting Saudi Arabia
yearly for the Hajj and Umrah
pilgrimages, no pilgrimage-related cases of MERS have been
reported.22 Although two
Dutch pilgrims returning from the 2014 Hajj received a
diagnosis of MERS,11 the source of
their infection remains unclear, and other members who traveled
in the same tour group
reported visiting camel markets and consuming raw camel milk
during activity unrelated to
Hajj. Saudi Arabian authorities have banned the presence of
camels near holy sites to
minimize exposure to potentially infected camels.23
Host Risk Factors
The majority of severe MERS cases have occurred in adults
older than 50 years of age who
have coexisting conditions such as diabetes, hypertension,
cardiac disease, obesity, chronic
respiratory disease, end-stage renal disease, or cancer or in
persons receiving
87. immunosuppressive therapy (Table S5 in the Supplementary
Appendix). Older age and
chronic respiratory illness have been associated with death
among infected patients.17 Mild
and asymptomatic infections have occurred predominantly
among young and healthy
persons, including health care workers.12,17 Clinically
recognized infections among
children are uncommon.24 Host genetic risk factors have not
been documented to date.
Virology
MERS-CoV is the sixth coronavirus and the first
betacoronavirus of the C phylogenetic
lineage known to infect humans.25 (Lineage A includes HCoV-
OC43 and HCoV-HKU1,
and lineage B includes the severe acute respiratory syndrome
[SARS] coronavirus [SARS-
CoV].) Similar to other coronaviruses, MERS-CoV is
enveloped, contains a very large (30
kb) single-stranded positive-sense RNA genome,26 and
replicates in the host-cell cytoplasm.
Sixteen nonstructural proteins serve roles in replication,
including a novel RNA
88. proofreading exonuclease that regulates replication fidelity27
(Table S3 in the
Supplementary Appendix). MERS-CoV tropism is determined
primarily by binding of the
virus spike glycoprotein to the cell-surface molecule, DPP-4
(Fig. 3). Attachment and entry
are further facilitated by a recently discovered cellular cofactor,
CEACAM5.28 The spike
glycoprotein can be activated to its fusogenic form by the host-
cell transmembrane serine
Arabi et al. Page 4
N Engl J Med. Author manuscript; available in PMC 2017
August 09.
E
urope P
M
C
F
unders A
uthor M
anuscripts
E
urope P
M
89. C
F
unders A
uthor M
anuscripts
protease TMPRSS2, endosomal cathepsins, and furin; this
suggests that there are multiple
possible pathways of spike maturation, viral entry into the cell,
and virion assembly.29,30
Circulating strains of human MERS-CoV to date appear to
represent a single serotype.31
Serum from convalescent patients with MERS29 and
neutralizing monoclonal antibodies to
the receptor-binding site of the spike glycoprotein inhibit
infection of cells by the virus.
32,33
Human Pathogenesis
Host-Cell Targets
DPP-4 is widely expressed on human cells, including
fibroblasts, intestinal epithelial cells,
and hepatocytes, and it has weak expression in the lung.34
CEACAM5 has a pattern of
90. expression that is more specific to cell type. In the gene-
expression atlas FANTOM5,34 only
a small number of tissues have detectable expression of both
DPP-4 and CEACAM5,
including tissues from the trachea, throat, small intestine, colon,
and appendix. In a finding
consistent with this observation, MERS-CoV has been shown to
replicate well in human cell
lines derived from respiratory and intestinal epithelium.35
In an ex vivo model of human lung-tissue infection, DPP-4
expression, MERS-CoV antigen,
and viral particles were found in bronchial epithelial cells, type
I and type II alveolar
pneumocytes, and vascular endothelial cells; the result was cell
death and diffuse alveolar
damage (Fig. 3).36 Alveolar macrophages appeared to be
relatively spared.36 A similar
pattern of DPP-4 distribution and viral replication has been seen
in nonhuman primate
models.37,38
Viral Kinetics
MERS-CoV RNA is detected more frequently and at higher viral
loads in samples from the