Vaccine Delivery
•
3 likes•542 views

This project identified opportunities for radical improvements in vaccine delivery and uptake towards the achievement of excellence and near-total vaccine coverage in regions similar to Bihar, India. - Conduct user-centered research and design to improve vaccine delivery. - Study behaviors, practices and attitudes of frontline workers and recipients. - Identify key dimensions of the delivery challenge. - Generate and validate concepts and solutions through collaborative brainstorming and dialogue with field data.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Vaccine Delivery
Similar to Vaccine Delivery (20)
Recently uploaded
Recently uploaded (20)
Vaccine Delivery
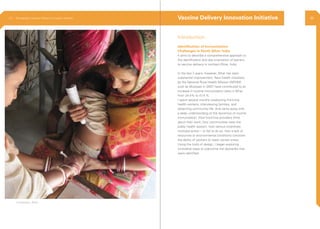
- 1. Introduction Identification of Immunization Challenges in North Bihar, India It aims to describe a comprehensive approach to the identification and documentation of barriers to vaccine delivery in northern Bihar, India. In the last 3 years, however, Bihar has seen substantial improvement. New health initiatives by the National Rural Health Mission (NRHM) such as Muskaan in 2007, have contributed to an increase in routine immunization rates in Bihar from 24.4% to 41.4 %. I spent several months shadowing front-line health workers, interviewing families, and observing community life. And came away with a deep understanding of the dynamics of routine immunization: How front-line providers think about their work; how communities view the public health system; how various incentives motivate action – or fail to do so; how a lack of resources or environmental conditions constrain the ability of workers to reach certain areas. Using the tools of design, I began exploring innovative ways to overcome the obstacles that were identified. Vaccine Delivery Innovation Initiative Kishanganj, Bihar 2.3 Ethnography | Vaccine Delivery Innovation Initiative 36
- 2. Size of the circle denotes, time spend in the perticular phase Objective 9 months Research Framework Analysis Concept Detailing Conclusion Methodologies Fieldwork Concept Generation ConceptTesting & Refinement Project Phases 2.3 Ethnography | Vaccine Delivery Innovation Initiative Experience Designer 38
- 3. This project identified opportunities for radical improvements in vaccine delivery and uptake towards the achievement of excellence and near- total vaccine coverage in regions similar to Bihar. • Conduct user-centered research and design to improve vaccine delivery. • Study behaviors, practices and attitudes of frontline workers and recipients. • Identify key dimensions of the delivery challenge. • Generate and validate concepts and solutions through collaborative brainstorming and dialogue with field data. Acc. - Accountant ANM - Auxiliary Nurse Midwife ASHA - Accredited Social Health Activist AWW - Anganwadi worker BCG - Bacillus Calmette-Guerin CDPO - Child Development Project Officer DIO - District Immunization Officer DLHS - District level household survey DPT - Diptheria Pertusis Tetanus EM - External Monitor HH - Head of Household HM - Health Manager ICDS - Integrated Child Development Scheme LS - Lady Supervisor MO - Medical Officer MOIC - Medical Officer in Charge NFHS - National Family Health Survey OPV - Oral Polio Vaccine PHC - Primary Health Centre PPP - Public Private Partnership RCH - Reproductive and Child Health RI - Routine Immunization RL - Religious Leader SC/ST - Scheduled Cast/Scheduled Tribe UNICEF - United Nations Children Fund UIP - Universal Immunization Programme VH - Village Head WHO - World Health Organization Glossary Objective MOIC (Medical Officer incharge diagnosing a patient 2.3 Ethnography | Vaccine Delivery Innovation Initiative 40
- 4. 3 Framework The framework guided us through out project. The team began to formulate hypothesis based on the initial round of background research dummy field work. The steps were Secondary Research Probe on the historical changes in India’s immunization status, key initiatives their impacts and immunization practices in Bihar were gathered Dummy feild work To get an idea of the real scenario on field an initial dummy field work was conducted, which can acted as a good starting point Expert Interviews A list of immunologist and public health programs experts were interviewed to gauge the existing scenario of immunization in Bihar Hypothesis creation A tentative list of questions arising from dummy field work and literature review were framedExpert Interviews MOIC addressing the ANM in the weekly Tuesday meeting 2.3 Ethnography | Vaccine Delivery Innovation Initiative 42
- 5. 1. Beneficiary Home visit 3. Depth Interview 2. Day - In - Life Ethnography 4. Mini Group Discussion 5. Clinics Visit Home visits with specific profiles such as pregnant mothers and neonatal families were conducted in order to understand the difficulties in following the current immunization process. Specific question areas around challenges of infrastructure, societal influences like caste and community were probed to gain insights around the perceptions of the service. To acquire insights around process of delivery, information dissemination and policy making a series of interviews were conducted with In order to understand the life and professional context of field workers namely ANM, ASHA, AWW who travel through the countryside dispensing healthcare services. They were followed on their daily route for three consecutive days. Insights around, 1. Challenges, Coping strategies and Needs of Health Workers 2. Qualitative insights into qualities of Moti vation and Initiative for Health Workers 3. Understanding of Roles and Responsibility of Health Workers 4. Service Delivery Drawbacks, were gathered Group discussion involving individual frontline healthworkers namely ANM, AWW and ASHA provided insights into glitches during recruitment, government bureaucracy. They identified challenges of the existing problems areas such as untimely payment of incentive, lack of transportation to Hard-to-Reach Areas render them ineffective to providing routine services. Ethnographic visits at vaccination clinics and local dispensaries reveled that most of them are quacks and are minting money out of the consumers. There knowledge comes form assisting doctors. It providing insights into the coping strategies of the consumers and pointed out reasons for consulting such a facility. Parents and Elder members of the Family District Immunization Officer, Accredited Chief Medical Officer, WHO officials Asha, AWW and ANM Private health practitioners and quacks Auxillary Nurse Midwife, Accredited Social Health Activist, AnganWadi Worker, Lady Health Visitor Methodology Senior Healthcare Officers. They being involved in the daily mechanism of delivering healthcare service, provided factual insights on the existing service model, context difficulties, challenges of delivery and identifying best practices of the current model, therefore, provided possible solution areas for designing new systems and models. 2.3 Ethnography | Vaccine Delivery Innovation Initiative 44
- 6. Design Diary A tool to document concepts and problem statements in form of sketches and doodles and to document a challenge or innovation opportunity during field work. It brought fresh perspective to classic problems of service delivery. Some of these ideas which were later built upon as leading concepts. Vaccine carrier box & disposal system 1. Description It is important to maintain an ecological balance and hence an effective disposal system is needed. 2. Observation • Inappropriate disposal outside Anganwadi Centre • The syringes are either burnt or thrown outside the PHC • The ANM needs to carry about 15-16 items on a RI day 3. Concept Vaccine carrier box serves as a vaccine temperature control unit. However, given its size and space, its full potential has not been explored. 4. Solution Description • An Integrated Vaccine Carrier which allows hub cutter, disposal and storage space. • At the PHC, all the vaccine carrier can be docked and the waste can be disposed in a single action format. 5. Impact and Value • Careless disposal often leads the used syringes falling in the hands of children. • Waste material collected over a period can be effectively utilized. ANM Registers Vitamin - A Hub Cutter Iron Tablets ORS Syringes Vaccine Carrier 3. Paraphernallia, ANM carries every RI day or Syringe Disposal Storage space1 2 Dock Station at Public Health Center (PHC) 2.3 Ethnography | Vaccine Delivery Innovation Initiative 46
- 7. Enhanced authority & Identification 1. Description Enhanced authority and identification can facilitate reach and increased awareness among recipients 2. Observation • ANM on her way to AWW centre but AWW and recipients of the zone are unaware of her arrival • Dress codes provided to the FHWs are barely used 3. Concept Frontline healthworkers do not have an identification tag, this often leads to beneficiaries not trusting them or not turning up on the immunization day. The beneficiaries lack awareness about these healthworkers, their duties and schedule. ID card that updated the center name where the ANM needs to go As the ID card enter the coverage zone, the operator sitting at the PHC is updated. The operator then announces arrival of the ANM in the locality through local media such as loudspeakers, radio, mobile phones 4. Impact and Value achieved • Mention of a person’s name on a media source is considered highly there by creating an authority in the minds of recipients • Such sources can prove to be useful in terms of generating a community-wide awareness of the profile of these FHWs. 2.3 Ethnography | Vaccine Delivery Innovation Initiative 48
- 8. Analysis Tracking Recipient Organizational Dynamics Identification & Compilation of Ethnographic Data Broader challenge areas were identified from the data set. They were then further categorized into sub-heads, address each topic while ideating for potential solution. One of the key questions addressed, how to track the recipients when they missed a scheduled vaccination day or a new birth? The tools utilized to do so are 1. Spatial Mapping - Maps created by ANM’s of their coverage zones were studied. 2. Record Keeping - With about 14-15 registers to maintain, it is a big challenge to update. These Reporting structure vary highly from district to district. This results in confusion about the roles and responsibilities of FHWs. Roles and Responsibilities of FHWs and Perceptions of their job are often misinterpreted. They are more often perceived as doctors by locals and consulted for medications and even for critical health issues. registers were studied for loopholes and why they act as a challenge 3. Micro Plan - A yearly plan made by Immunization officers, where ANMs are alloted coverage zones Spatial Mapping Record Keeping 2.3 Ethnography | Vaccine Delivery Innovation Initiative 50
- 9. Challenges and Barrier to Routine Immunization Concept ofTime andTemporality 1. Logistical Issues: Unavailability of basic facilities such as transportation and field tool such registers, medicines, injections, etc. 2. Soft Practices: Many jury-rigged methods were adopted by FHWs on field such as no real-time updation of records, instead they note down information in small pieces of paper. The concept of timing in these rural areas are mostly day-to-day basis, as most of these family do not have a calender. Therefore, making it tough for them to remember the exact date when their child was scheduled for immunization. ANM’s note records on rough paper while on field Local methods used by ANM’s to identify Immunization age ( The child who is able to touch his ear with the left hand is 5 years and above, while the other two are not) No proper roads Clocks and calendars with deities pictures are one of the most common artifacts found in the rural households 2.3 Ethnography | Vaccine Delivery Innovation Initiative 52
- 10. Socio-Cultural Practices 1. Natal Practices: Cultural factor in rural locations act as a major hindrance toward timely immunization. For instance, muslim families do not allow the mother to come out of the house for a month as they consider this period to be impure. 2. Child Protection and Safety: Black threads around the baby’s arm or neck is tied after 6 days of birth, this leads to the child not getting his first shot of BCG and OPV1 vaccine. 23 yr old lady, mother of three. According to Hindu customs the mother is not allowed to step outside her room for a month, as she is considered impure right after her delivery 2.3 Ethnography | Vaccine Delivery Innovation Initiative 54
- 11. Bubble Mapping: Key Stakeholders Experience Flow MappingHeuristic tools for channelizing analysis In order to focus the research analysis and analyse key players of the RI ecology, it was necessary to identify Key Stakeholders. Bubble mapping these key stakeholders illustrated the significance of the roles played by each player. It also helps reveal their proximity in terms of interaction. Frontline health worker and recipient family are central players here. Generated experience flow diagrams for frontline healthworkers and recipient families by sequentially mapping their work practices and daily routine. It revealed coordination between different players in the RI system during various activities. Highlighted the challenges faced by FHWs and the adaptive practices employed to counter them. MOIC ANM AWW AWWs DAI ASHA Mother & Child ASHA’s Husband Father Private Practitioner Stakeholder Ecology Advance Preparation - Preparation of the site not done in advance leading to chaotic worldspace ANM arrival at RI site - ANM may arrive late after the vaccine carrier is delivered Courier man comes to the session site Leaves from session site Set up the RI site Goes to mobilize recipients Goes to mobilize recipients ASHA comes to the site ANM arrives at the RI site Goes to the session site Reluctant to go to RI site Families reaches RI site with the health card Family comes to RI site without health cardRecipient not found at home She comes to the site She consults the ANM for list of due recipients and goes for mobilizing Stays back at session site Courier Boy AWW ASHA ANM Recipient Key Players Pre Administration Key Co-ordination Issues 2.3 Ethnography | Vaccine Delivery Innovation Initiative 56
- 12. Power Dynamics Social Interaction To understand the power a player shares over another power level were plotted. This helped in revealing sources whose power can be utilized to effect changes, as well as for creating supervision mechanisms. A heuristic tool to map the interaction levels of each player in the system. Frequencies of social interaction could then be employed for designing communication strategies for the mother and the recipient family. It also helped reveal under utilized resources that can be employed for key performance areas. Central players Other players 0.5pt0.75pt1pt1.5pt2pt3pt MOIC HM Acc. EM VH LS ASHA ANM AWW Mother CDPO HH RL Acc. ANM ASHA AWW CDPO EM HH HM LS MOIC RL VH - Accountant - Auxiliary Nurse Midwife - Accredited Social Health Activist - Anganwadi worker - Child Development Project Officer - External Monitor - Head of Household - Health Manager - Lady Supervisor - Medical Officer in Charge - Religious Leader - Village Head Central players Other players 1pt 0.5pt1.75pt2pt3pt4pt5pt AWW ASHA other ASHA ANM AWW Mother MOIC HM Acc. EM VH other ANMLS CDPO HH RL Identified key performance areas in the RI system Enrollment of new recipients Mobilization Enable repeat encounter Education Supervision Performance evaluation of FHWs 2.3 Ethnography | Vaccine Delivery Innovation Initiative 58
- 13. 1. Identifying & Locating recipients Identifying Challenges • FHWs do not have a concrete knowledge of their coverage areas (both boundaries and households) • ASHAs do not cover their zones thoroughly on RI day because they are too big 2.Tracking FHWs are unable to accurately track recipients because record-keeping tools are not easily searchable, most health cards are either damaged or lost. 3. Supervision No supervision or feedback mechanisms for frontline health workers and other officials result in “apathy” and lack of accountability in the health care system. 4. Communication • Recipient families are unaware of the significance of RI because it is not promoted at all in the community. • Recipient families also lack understanding of the significance of complete immunization. Consequently, dropouts occur when their children experience side-effects. 5. Planning Planning is not data driven ; FHWs are not aware of the right denominator and not motivated to enroll many new recipients in the system. 6.Training Health workers are not trained well enough to convince families that resist immunization. Conceptualization Communication Concepts generated to create awareness among beneficiary families Comparison chart depicting a healthy immunized child and a weak un-immunized child in pain Audio activated toys in order to create awareness among the mothers who are mostly housewives Balloon marking at the immunization center in order to mark a specific location 2.3 Ethnography | Vaccine Delivery Innovation Initiative 60
- 14. Identifying & Locating One of the key challenges faced by the FHWs, is to located prospective beneficiaries as well as spot beneficiaries for subsequent doses. Supervision Currently there is a major lack in the supervision of ground level staff. This particular work on an effective mechanism to increase supervision without physical presence of supervisors AWW conducts a survey of her area, and passes the information to the data operator at the PHC. A 2-D aerial map of the village is generated AWW carries a navigational device which provides her with a 3D view of her area. The devices provides her with the shortest routes to reach the beneficiary As she closes the house, the devices marks the house and gives an audio feedback. The AWW reaches the house, takes a photograph of the beneficiary and send it to the database. A kiosk at every RI site, which monitors the attendance of FHWs, takes feedback from recipient families and displays information of the due beneficiaries. The kiosk transfers the data to the central PHC which takes out a performance report of the FHWs based on targets. Village information Block information District information State information Stepwise data is collected and uploaded, starting from village to state level on to an online portal. This portal can be accessed by any of the senior supervisors at any point of time. 2.3 Ethnography | Vaccine Delivery Innovation Initiative 62
- 15. Tracking Recipients AWW encounters a pregnant lady, she takes down all the basic information and informs the ANM At birth the ANM provides the child with a unique ID and gives her a card which mentions the next vaccine due date. On the RI day, child’s medical history is accessed through the unique ID and he is administered with the right dose of vaccine. The digital device provides the ANM with the list of children she needs to administer on that day and the missed recipients. Communication • The concept of introducing a toy which creates awareness about R.I. should also talk about the due date of vaccine • The concept of comparing a healthy and an unhealthy child pictorially will prove beneficial as it will also communicate with the illiterate recipients Identifying & Locating • Click photographs of new recipients will work. • The idea of introducing a GPS will aid there search. Supervision • A performance merit list displayed on the PHC’s notice board will motivate all the FHWs. • The kiosk should be setup at most of the AWC with an operator in the initial days. • The kiosk can also provide meeting timings. Tracking • Formal training will be required in order to optimally use this technology. They seem very satisfied with the idea of replacing survey registers with a digital device. • They like the idea of a digital device as compared to maintaining bulky survey registers. Concept Testing 2.3 Ethnography | Vaccine Delivery Innovation Initiative 64